You might also like
- ATI Medication FormDocument5 pagesATI Medication FormElaine De Vera100% (1)
- Family Planning Service Record Form IDocument4 pagesFamily Planning Service Record Form IBarangay Lam-anNo ratings yet
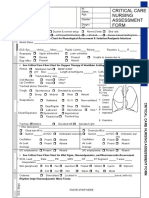
- Idoc - Pub - Critical Care Nursing Assessment FormDocument3 pagesIdoc - Pub - Critical Care Nursing Assessment FormNamra AnsariNo ratings yet
- Annotated BibliographyDocument3 pagesAnnotated Bibliographyapi-462495619No ratings yet
- Psychology WebDocument27 pagesPsychology WebしまののえだにNo ratings yet
- CHAPTER 1 Hospital PharmacyDocument25 pagesCHAPTER 1 Hospital PharmacyMurtaza Haider100% (2)
- Individual Dental Health Record: Republic of The PhilippinesDocument2 pagesIndividual Dental Health Record: Republic of The PhilippinesAto SupNo ratings yet
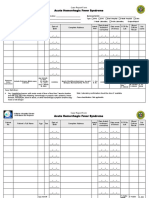
- Acute Hemorrhagic Fever - CRFDocument1 pageAcute Hemorrhagic Fever - CRFMary Anne Grace GarridoNo ratings yet
- EMA Monitoring Chart 2021Document2 pagesEMA Monitoring Chart 2021Abdullah Khan ShahiNo ratings yet
- Dental Health Record Teaching and Non-Teaching Personnel: Index: DMFTDocument2 pagesDental Health Record Teaching and Non-Teaching Personnel: Index: DMFTEmerson NunezNo ratings yet
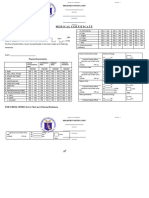
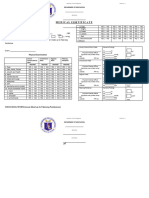
- Medical For Athletes 1Document2 pagesMedical For Athletes 1ERWIN PEJINo ratings yet
- Acute Hemorrhagic Fever Syndrome - Ver Oct 12 2012 PDFDocument2 pagesAcute Hemorrhagic Fever Syndrome - Ver Oct 12 2012 PDFCHICKYNo ratings yet
- Xray Order FormDocument1 pageXray Order FormSN Malenadu CreationNo ratings yet
- Monitoring Sheet ISU Dummy ChartDocument6 pagesMonitoring Sheet ISU Dummy ChartMhar IcelNo ratings yet
- Big Eyes Small Mouth-2nd Edition PDFDocument2 pagesBig Eyes Small Mouth-2nd Edition PDFOxgardNo ratings yet
- Non-Neonatal Tetanus: (ICD 10 Code: A35)Document2 pagesNon-Neonatal Tetanus: (ICD 10 Code: A35)CHICKY100% (1)
- A.V. Aids by PRIYANKADocument26 pagesA.V. Aids by PRIYANKAPriyanka SheoranNo ratings yet
- 2024 - Medical For Athletes 1Document2 pages2024 - Medical For Athletes 1DIONELTON PELAYONo ratings yet
- Dental BHSS 2019Document1 pageDental BHSS 2019roulette laypNo ratings yet
- Ecatalog Maret 2019 - RevDocument8 pagesEcatalog Maret 2019 - RevRisqon Anjahiranda AdiputraNo ratings yet
- Medical For Athletes 1Document2 pagesMedical For Athletes 1Leah CarnateNo ratings yet
- YAago Medical-1Document1 pageYAago Medical-1Terence VeronaNo ratings yet
- Medical For Athletes 1 1Document1 pageMedical For Athletes 1 1Lloyd Benitez De GuzmanNo ratings yet
- Jack RoadDocument2 pagesJack RoadbrayanalbiaaulNo ratings yet
- Monitoring & Mutu FarmasiDocument4 pagesMonitoring & Mutu FarmasisupraptiNo ratings yet
- 100 Ob Intensive Nov2023 MergedDocument44 pages100 Ob Intensive Nov2023 MergedErika ArceoNo ratings yet
- Prescription Abbreviations Used in PharmacyDocument2 pagesPrescription Abbreviations Used in PharmacySolCharmerNo ratings yet
- Penjadwalan Operasi Mei 05.05.21Document1 pagePenjadwalan Operasi Mei 05.05.21Adriel BenedictNo ratings yet
- Web Version ASA Anaesthesia RecordDocument2 pagesWeb Version ASA Anaesthesia RecorderyxspNo ratings yet
- Medical For Athletes 1Document2 pagesMedical For Athletes 1Mitchie MuyotNo ratings yet
- Medical For Athletes EDITEDDocument1 pageMedical For Athletes EDITED301416No ratings yet
- Lee, Angel Joacquin - MVTDocument2 pagesLee, Angel Joacquin - MVTcaderaoangelNo ratings yet
- Oral Health Examination Record For Teaching and Non Teaching PersonnelDocument1 pageOral Health Examination Record For Teaching and Non Teaching PersonnelAda RicanaNo ratings yet
- Medical For Athletes 1Document2 pagesMedical For Athletes 1Anna Jessica NallaNo ratings yet
- Medical For Athletes 1Document2 pagesMedical For Athletes 1JONATHAN VILLANUEVANo ratings yet
- Sample - Medical For Athletes Edited With MD JasmineDocument2 pagesSample - Medical For Athletes Edited With MD JasmineCatzuu DmNo ratings yet
- Preop+++Goal Anaesthesia Record FormsDocument5 pagesPreop+++Goal Anaesthesia Record FormsShimelis AssefaNo ratings yet
- 4 - Medical For Athletes 2024Document2 pages4 - Medical For Athletes 2024royNo ratings yet
- 2024 - Medical For Athletes 1Document2 pages2024 - Medical For Athletes 1FEY CARL DELOS SANTOSNo ratings yet
- Medical For Athletes 1 PENAFIELDocument2 pagesMedical For Athletes 1 PENAFIELRodolfo Esmejarda Laycano Jr.No ratings yet
- Medical For Athletes 1.1Document1 pageMedical For Athletes 1.1MARJORIE HERNANDEZNo ratings yet
- Psychiatric Visit1 - AaronVer3Document1 pagePsychiatric Visit1 - AaronVer3api-3764308No ratings yet
- Modul Bedah 2 - DR RianDocument18 pagesModul Bedah 2 - DR RianDendy AgusNo ratings yet
- Medical For Athletes 1Document2 pagesMedical For Athletes 1Lormy Layeka Calderon SiolNo ratings yet
- Medical For Athletes 1Document2 pagesMedical For Athletes 1Tarhata LampatanNo ratings yet
- 2024 - Medical For Athletes 1Document1 page2024 - Medical For Athletes 1FEY CARL DELOS SANTOSNo ratings yet
- 4.a. Medical For Athletes 1Document1 page4.a. Medical For Athletes 1Maria Camille Villanueva SantiagoNo ratings yet
- Medical For Athletes 1Document2 pagesMedical For Athletes 1arminaNo ratings yet
- Medical For Athletes 1 ANDRADEDocument2 pagesMedical For Athletes 1 ANDRADERodolfo Esmejarda Laycano Jr.No ratings yet
- Medical For Athletes 1Document2 pagesMedical For Athletes 1SHIERRA ANNE CARAELNo ratings yet
- LEVANTAMIENTO DIMESION VERTICAL 2 - UnlockedDocument19 pagesLEVANTAMIENTO DIMESION VERTICAL 2 - Unlockedchrystin1981No ratings yet
- Medical For Athletes 1Document2 pagesMedical For Athletes 1Farah IsmurajaNo ratings yet
- Medical For Athletes 1Document1 pageMedical For Athletes 1Alice EdisNo ratings yet
- Demonstratii Imagistice-CompletatDocument51 pagesDemonstratii Imagistice-CompletatAndrei OriţăNo ratings yet
- FoodLifeline ImpactReport 2018 1Document3 pagesFoodLifeline ImpactReport 2018 1PATRICK AWUKU LARBI RDNo ratings yet
- Medical For Athletes 1Document1 pageMedical For Athletes 1Ahr Jhay VillamaterNo ratings yet
- Pedagogical Practicum I Syllabus 2023-1Document8 pagesPedagogical Practicum I Syllabus 2023-1Laura LombanaNo ratings yet
- Medical For Athletes 1Document2 pagesMedical For Athletes 1John Elton PilarNo ratings yet
- Level: (1) N/A (2) Affected Area (3) Affected Area & Related Area (4) : Affect in Detail & Related (5) 8 SysDocument3 pagesLevel: (1) N/A (2) Affected Area (3) Affected Area & Related Area (4) : Affect in Detail & Related (5) 8 SysPatrick ShieldsNo ratings yet
- Jsa Cal OrificeDocument3 pagesJsa Cal OrificeLangit GanjarNo ratings yet
- Lear Ni Ngmodul E I N Gee103 Phi L I Ppi Nepopul Arcul T Ur EDocument14 pagesLear Ni Ngmodul E I N Gee103 Phi L I Ppi Nepopul Arcul T Ur EWho Killed Panda?No ratings yet
- Medical For Athletes 1Document2 pagesMedical For Athletes 1Patrick RodriguezNo ratings yet
- Medical For Athletes 1Document2 pagesMedical For Athletes 1Rodolfo Esmejarda Laycano Jr.No ratings yet
- Canadian Personal Care Provider Canadian 1st Edition by Wolgin ISBN Test BankDocument6 pagesCanadian Personal Care Provider Canadian 1st Edition by Wolgin ISBN Test Bankrobert100% (25)
- NRSG 5500 Syllabus Su 14 1Document4 pagesNRSG 5500 Syllabus Su 14 1api-310557802No ratings yet
- Temporomandibular DisordersDocument45 pagesTemporomandibular DisordersMohsin HabibNo ratings yet
- Authorised Representative License: Executive Department of Registration and LicensingDocument1 pageAuthorised Representative License: Executive Department of Registration and LicensingFERAS ALSAMAKNo ratings yet
- StuviaDocument4 pagesStuviagNo ratings yet
- US FDA Warning LettersDocument6 pagesUS FDA Warning LettersSangram KendreNo ratings yet
- Glytrin Brand Plan 2016-17 FinalDocument54 pagesGlytrin Brand Plan 2016-17 FinalIndranil PoddarNo ratings yet
- Chapter 5 - Counselling Skills: The GP As An Effective CounsellorDocument19 pagesChapter 5 - Counselling Skills: The GP As An Effective Counsellorprofarmah6150100% (2)
- Module 5 QuizDocument3 pagesModule 5 Quizapi-329063194No ratings yet
- BSN Curriculum Revision Project Plan 2Document2 pagesBSN Curriculum Revision Project Plan 2api-372924050No ratings yet
- LegMed 3Document70 pagesLegMed 3Anthony Tamayosa Del AyreNo ratings yet
- Antiobiotics Use Them Wisely 800 Passage and QuestionsDocument5 pagesAntiobiotics Use Them Wisely 800 Passage and Questionsdinh lanNo ratings yet
- Ebook PDF Core Curriculum For Oncology Nursing 5th Edition PDFDocument41 pagesEbook PDF Core Curriculum For Oncology Nursing 5th Edition PDFcarla.shurtliff473100% (40)
- Theories, Models and FrameworkDocument2 pagesTheories, Models and FrameworkBardiaga JmayNo ratings yet
- LMRASSIGNMENTDocument2 pagesLMRASSIGNMENTjaoNo ratings yet
- Automatic Stop OrdersDocument3 pagesAutomatic Stop OrdersindraNo ratings yet
- Occupational Health & Safety ReportDocument18 pagesOccupational Health & Safety Reportargya nareswaraNo ratings yet
- RivasnicuDocument3 pagesRivasnicuapi-613460741No ratings yet
- Katayani Himeo - Google SearchDocument1 pageKatayani Himeo - Google SearchSonnet XavierNo ratings yet
- Acid& Chemical Burns Part ADocument10 pagesAcid& Chemical Burns Part ASojiNo ratings yet
- Bicalutamide Monograph 1october2011Document5 pagesBicalutamide Monograph 1october2011shorfuddinfcc7816No ratings yet
- Ecpg OrlapDocument258 pagesEcpg OrlapNoha Ibraheem HelmyNo ratings yet
- Aviva Ntu SP Panel ListingDocument20 pagesAviva Ntu SP Panel ListingAnonymous khVxwzn83No ratings yet
- True MedicineDocument52 pagesTrue MedicineMoga RazvanNo ratings yet
- Infection Prevention and Control in Paediatric Office SettingsDocument15 pagesInfection Prevention and Control in Paediatric Office SettingsGhalyRizqiMauludinNo ratings yet