You might also like
- Maternity Benefit: What Do I Need To Complete This Application Form?Document16 pagesMaternity Benefit: What Do I Need To Complete This Application Form?Vlad PerjuNo ratings yet
- Authority FormDocument2 pagesAuthority Formrosegr332No ratings yet
- Your Extras and Medical Claim Form: SECTION A: Your DetailsDocument3 pagesYour Extras and Medical Claim Form: SECTION A: Your DetailsTGNo ratings yet
- Change of Details FormDocument4 pagesChange of Details FormJonathan EvansNo ratings yet
- Bupa Claim FormDocument1 pageBupa Claim FormcrazydeveloperNo ratings yet
- Ca5400 Application For A National Insurance NumberDocument4 pagesCa5400 Application For A National Insurance NumberSamuel MutahiNo ratings yet
- Inductions - Application For Employment - v1.5Document4 pagesInductions - Application For Employment - v1.5SEBASTIAN PULIDO MOJICANo ratings yet
- Cancellation Form Refund RequestDocument2 pagesCancellation Form Refund RequestVinh Duong0% (1)
- Update Fund Value and Allocation Mobile AlertsDocument1 pageUpdate Fund Value and Allocation Mobile AlertsArvind SharmaNo ratings yet
- OVFA FormDocument2 pagesOVFA FormanetecdNo ratings yet
- Maturity Form: Policy InformationDocument2 pagesMaturity Form: Policy Informationroodra singh ranawatNo ratings yet
- Muthoot Finance Business Loan XH Enrolment Form v1Document2 pagesMuthoot Finance Business Loan XH Enrolment Form v1Subramanyam JonnaNo ratings yet
- Application For Employment BermudaDocument3 pagesApplication For Employment BermudaNichole ZuillNo ratings yet
- General Guidelines To Fill Up AF FormDocument10 pagesGeneral Guidelines To Fill Up AF FormDiky ArioNo ratings yet
- Application For Reinstatement or Policy ChangeDocument2 pagesApplication For Reinstatement or Policy ChangeCristhelDelaTorreNo ratings yet
- DXN Distributorship Data Update Request Form - Version 4Document1 pageDXN Distributorship Data Update Request Form - Version 4Mohammed muqsithNo ratings yet
- Mark FormDocument2 pagesMark FormDiana Teresa Vargas AristaNo ratings yet
- Care Giver Application Form 2022Document9 pagesCare Giver Application Form 2022JoNo ratings yet
- Public Service Application For ForgivenessDocument9 pagesPublic Service Application For ForgivenessLateshia SpencerNo ratings yet
- Form FA10MSNP2 2Document6 pagesForm FA10MSNP2 2Fatemeh ArefianNo ratings yet
- Application Form Enwealth new AccountDocument2 pagesApplication Form Enwealth new AccounticttumainiNo ratings yet
- HSBC Life - Personal Particulars Update Form For Corporate - GI and HIDocument3 pagesHSBC Life - Personal Particulars Update Form For Corporate - GI and HIKetan VashishthaNo ratings yet
- SGP Generic Claim FormDocument5 pagesSGP Generic Claim FormSanny HamdaniNo ratings yet
- Medical Report For A Canada Pension Plan Disability BenefitDocument14 pagesMedical Report For A Canada Pension Plan Disability BenefitVithursanNo ratings yet
- Application Form - Reduce Monthly Repayment Amount PDFDocument2 pagesApplication Form - Reduce Monthly Repayment Amount PDFasdsaNo ratings yet
- New Hire Package BC - Hourly - FY2022-02-PADocument14 pagesNew Hire Package BC - Hourly - FY2022-02-PARuben 24 :DNo ratings yet
- SG Simplecare Individuals ApplicationDocument8 pagesSG Simplecare Individuals Applicationmanishkpandey07No ratings yet
- App Form ProvidentDocument4 pagesApp Form ProvidentDionisio Mary GraceNo ratings yet
- Canada EiDocument1 pageCanada EishaunNo ratings yet
- Downloadable Rental Ledger TemplateDocument4 pagesDownloadable Rental Ledger TemplatemaroNo ratings yet
- Important Reminders:: (Claim Form)Document1 pageImportant Reminders:: (Claim Form)abejhieNo ratings yet
- Change of Personal Particulars FormDocument3 pagesChange of Personal Particulars FormAntony VijayNo ratings yet
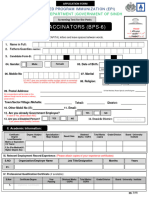
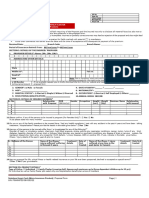
- Vaccinators (Bps-6) : Health Department - Government of SindhDocument3 pagesVaccinators (Bps-6) : Health Department - Government of SindhAbdulrehman NizamaniNo ratings yet
- Paternity Benefit: Employed, Your Employer Must Complete This Form To Certify You AreDocument2 pagesPaternity Benefit: Employed, Your Employer Must Complete This Form To Certify You AreBahia El RefaiNo ratings yet
- Claim Form: You Can Make Your Claim With Cover-More in 3 Simple Steps: Fill Out The Claim FormDocument13 pagesClaim Form: You Can Make Your Claim With Cover-More in 3 Simple Steps: Fill Out The Claim FormLe AnnaNo ratings yet
- Giro Appln Form For FDWDocument2 pagesGiro Appln Form For FDWanie zuNo ratings yet
- Disability Critical Illness Medical Reimbursement or Hospitalization Claim FormDocument5 pagesDisability Critical Illness Medical Reimbursement or Hospitalization Claim FormAkoSiAudreyNo ratings yet
- Apollo Change Request Form PDFDocument1 pageApollo Change Request Form PDFJituNo ratings yet
- Provident Fund: Republic of The Philippines Department of EducationDocument4 pagesProvident Fund: Republic of The Philippines Department of EducationBen T OngNo ratings yet
- Application Submitted ConfirmationDocument6 pagesApplication Submitted Confirmationmae valentineNo ratings yet
- Temporary Rehabilitation Remuneration Form-HR114: Section 1. To Be Completed by The EmployeeDocument3 pagesTemporary Rehabilitation Remuneration Form-HR114: Section 1. To Be Completed by The EmployeeLexNo ratings yet
- Policy Fund Withdrawal Form: FWP/FSC CodeDocument2 pagesPolicy Fund Withdrawal Form: FWP/FSC CodeEra gasperNo ratings yet
- Application Form FA10C New Custom Food Control Plan Under Food Act 2014Document7 pagesApplication Form FA10C New Custom Food Control Plan Under Food Act 2014Fatemeh ArefianNo ratings yet
- Comp/Feb/Int/5034 | PSRF245009032007 NACH mandate instructionDocument2 pagesComp/Feb/Int/5034 | PSRF245009032007 NACH mandate instructionAnithaNo ratings yet
- Surrender Form SummaryDocument3 pagesSurrender Form SummaryDevendra RawoolNo ratings yet
- Imperial AgencyDocument2 pagesImperial AgencySwift DataNo ratings yet
- Separation Document - Ss293 1707en PDocument13 pagesSeparation Document - Ss293 1707en PMark LordNo ratings yet
- Policy Fund Withdrawal FormDocument2 pagesPolicy Fund Withdrawal FormJulius Harvey Prieto BalbasNo ratings yet
- Joining Bupa GlobalDocument12 pagesJoining Bupa GlobalMayar RagabNo ratings yet
- Investigation Request FormDocument2 pagesInvestigation Request FormAhmad HusseinNo ratings yet
- Application FormDocument4 pagesApplication FormNouman KhanNo ratings yet
- Sukshma Hospi CashDocument4 pagesSukshma Hospi CashAdemuyiwa OlaniyiNo ratings yet
- Change Request Form: This Is A Watermark For Trial Version, Register To Get Full One!Document1 pageChange Request Form: This Is A Watermark For Trial Version, Register To Get Full One!Kumari MadhumitaNo ratings yet
- Form 03092015 Application For Pre Need PlansDocument2 pagesForm 03092015 Application For Pre Need PlansRosalyn DelfinNo ratings yet
- Form PDFDocument7 pagesForm PDFPaul BeznerNo ratings yet
- Futuregensurrenderform 25Document2 pagesFuturegensurrenderform 25accountsNo ratings yet
- TCCI Application Form For Local Employment (2022)Document3 pagesTCCI Application Form For Local Employment (2022)Geraldine VergaraNo ratings yet
- Bakery Franchise Application Form TemplateDocument6 pagesBakery Franchise Application Form TemplateardhenduchatterjeeNo ratings yet
- Personal Information Sheet PDFDocument2 pagesPersonal Information Sheet PDFRonelyn CalimbayanNo ratings yet
- LP Math 7 (4) (Integers-Division)Document2 pagesLP Math 7 (4) (Integers-Division)Rookie LoraNo ratings yet
- DCMotorsDocument19 pagesDCMotorsAndrew BuckleyNo ratings yet
- Resume of Jhune Perez RTDocument2 pagesResume of Jhune Perez RTByahe Ni GeloNo ratings yet
- Air Matic W222Document4 pagesAir Matic W222Văn Chung LêNo ratings yet
- Information Engineering Facility Tool for Software DevelopmentDocument56 pagesInformation Engineering Facility Tool for Software DevelopmentVivianNo ratings yet
- BDT 135 e-ticket booked for Adhora Ruma's journey from BBSETU_E to DHAKA on SUNDARBAN_EXPRESSDocument1 pageBDT 135 e-ticket booked for Adhora Ruma's journey from BBSETU_E to DHAKA on SUNDARBAN_EXPRESSMS.sumonNo ratings yet
- Accounting & Finance Professional: Uzair Ahmed KhanDocument5 pagesAccounting & Finance Professional: Uzair Ahmed KhanmedicotNo ratings yet
- The Influence of The Mass Media in The Behavior Students A Literature Study PDFDocument9 pagesThe Influence of The Mass Media in The Behavior Students A Literature Study PDFclarissa OrosaNo ratings yet
- MFL Floormap - How To Scan and Get DataDocument18 pagesMFL Floormap - How To Scan and Get DataNguyen PhucNo ratings yet
- Retinopathy Report 2023Document83 pagesRetinopathy Report 2023Hydra ANINo ratings yet
- Catalogo VPFT 4535Document91 pagesCatalogo VPFT 4535PRISCILA FAGUNDESNo ratings yet
- Unit IIIDocument5 pagesUnit IIISandhya FugateNo ratings yet
- Ornek WPS (ASME IX)Document1 pageOrnek WPS (ASME IX)kaynakteknolojiNo ratings yet
- Inventory Management For Retail Companies: A Literature Review and Current TrendsDocument9 pagesInventory Management For Retail Companies: A Literature Review and Current Trendstop techi tamizhaNo ratings yet
- Metal Bellow Seal InstallationDocument4 pagesMetal Bellow Seal InstallationkiranNo ratings yet
- 24 Territory Brochure enDocument12 pages24 Territory Brochure enmohammed sameer100% (1)
- Isee Nses2023 BrochureDocument12 pagesIsee Nses2023 BrochurehksachinNo ratings yet
- Motor Control Circuit Activity Ladder DiagramDocument11 pagesMotor Control Circuit Activity Ladder DiagramAJ LunaNo ratings yet
- CodeTech Annual Inter-School Tech Symposium Results and WinnersDocument21 pagesCodeTech Annual Inter-School Tech Symposium Results and WinnerskhushiNo ratings yet
- A Practical Guide To Artificial Intelligence-Based Image Analysis in RadiologyDocument7 pagesA Practical Guide To Artificial Intelligence-Based Image Analysis in RadiologyGeneNo ratings yet
- Shakirullah Niazi: Professional SummaryDocument4 pagesShakirullah Niazi: Professional SummaryShakir UllahNo ratings yet
- Essar Steel PlantDocument62 pagesEssar Steel PlantKrishnadev C.SNo ratings yet
- Student Assessment GuideDocument72 pagesStudent Assessment GuideDavi MoraesNo ratings yet
- Abrasion TestDocument7 pagesAbrasion TestMohd SyahrulizamNo ratings yet
- Azure InvoiceDocument2 pagesAzure InvoiceAnkit SambhareNo ratings yet
- Practical Application of Refrigerants R600A and R290 in Small Hermetic SystemsDocument20 pagesPractical Application of Refrigerants R600A and R290 in Small Hermetic SystemsTedy Corimanya SoriaNo ratings yet
- Kit de CommunicationDocument3 pagesKit de CommunicationdupontNo ratings yet
- Advanced Construction TechnologyDocument6 pagesAdvanced Construction TechnologyNik SoniNo ratings yet
- RatioandRegressionMethodofEstimation Lecture7 10Document30 pagesRatioandRegressionMethodofEstimation Lecture7 10mrpakistan444No ratings yet
- Installation: Indoor UnitDocument10 pagesInstallation: Indoor UnitJohan FloresNo ratings yet