You might also like
- Plasenta Dan SelaputDocument18 pagesPlasenta Dan SelaputRahmi Mutia UlfaNo ratings yet
- Day 1Document21 pagesDay 1Ahmed DorghamNo ratings yet
- Anatomy of Normal PlacentaDocument8 pagesAnatomy of Normal PlacentaMaharani KartikaNo ratings yet
- Anatomy of Normal PlacentaDocument8 pagesAnatomy of Normal Placentaareejk_94No ratings yet
- Ferlilisation, Implantation and Changes in PregnancyDocument7 pagesFerlilisation, Implantation and Changes in PregnancyLuke MatupiNo ratings yet
- Additional Notes On Placenta-1Document4 pagesAdditional Notes On Placenta-1Cearlene GalleonNo ratings yet
- Module 3 Process of Conception MaternalDocument7 pagesModule 3 Process of Conception MaternalJustine FloresNo ratings yet
- Postimplantation Development in MammalianDocument52 pagesPostimplantation Development in MammalianBiology BảoNo ratings yet
- Placenta: Fetomaternal Organ. Fetal Part Maternal Part Transport SystemDocument21 pagesPlacenta: Fetomaternal Organ. Fetal Part Maternal Part Transport SystemAntonela CeremușNo ratings yet
- Fertilization Fetal DevelopmentDocument97 pagesFertilization Fetal DevelopmentXo Yem100% (1)
- Cleavage and ImplantationDocument20 pagesCleavage and Implantationpavi7muruganathanNo ratings yet
- By - Prof. Saeed MakaremDocument27 pagesBy - Prof. Saeed MakaremIncredible DivineNo ratings yet
- 2nd WeekDocument16 pages2nd WeektuyuNo ratings yet
- Placenta DevelopmentDocument13 pagesPlacenta DevelopmentSudesh TomarNo ratings yet
- ImplantationDocument16 pagesImplantationapi-249972919No ratings yet
- PLACENTADocument21 pagesPLACENTAHem Kumari75% (4)
- Bif Emb Ls 8 PlacentaDocument77 pagesBif Emb Ls 8 PlacentaJude Chisom Jnr NwaugoNo ratings yet
- The Development of The EmbryoDocument80 pagesThe Development of The EmbryovictorNo ratings yet
- Classification of Placenta PDFDocument5 pagesClassification of Placenta PDFAdarsh jainNo ratings yet
- Classification of Placenta PDFDocument5 pagesClassification of Placenta PDFAdarsh jainNo ratings yet
- Classification of Placenta PDFDocument5 pagesClassification of Placenta PDFAdarsh jainNo ratings yet
- 02 - Stages - of - Pregnancy - NCM 207Document6 pages02 - Stages - of - Pregnancy - NCM 207mayangernszNo ratings yet
- Placenta Types and GradingDocument37 pagesPlacenta Types and GradingNishant RajNo ratings yet
- Ginther, 1998 Equine PregnancyDocument32 pagesGinther, 1998 Equine PregnancyAdrian Ayala GutierrezNo ratings yet
- THE FETUS and PLACENTADocument50 pagesTHE FETUS and PLACENTAKyla CalsoNo ratings yet
- MCN Lec - Chapter 3Document18 pagesMCN Lec - Chapter 3David LomentigarNo ratings yet
- Human Fertilization Is The Union of A Human Egg and SpermDocument7 pagesHuman Fertilization Is The Union of A Human Egg and Spermoxidalaj100% (1)
- Lec 2Document37 pagesLec 2ibrahim.21hm32No ratings yet
- 2nd Week Devt PDFDocument22 pages2nd Week Devt PDFbookaccountNo ratings yet
- Lab 9b - Embryonic DevelopmentDocument17 pagesLab 9b - Embryonic Developmentn4ctvpjvj7No ratings yet
- NCM 107 Module-5 - Conception-NOTESDocument2 pagesNCM 107 Module-5 - Conception-NOTESKisha BethelNo ratings yet
- (OB) 1.05 Implantation and Embryogenesis - Dr. AttabanDocument8 pages(OB) 1.05 Implantation and Embryogenesis - Dr. AttabanMarlon BauagNo ratings yet
- Abnormal ImplantationDocument3 pagesAbnormal ImplantationMuhammet Fatih CantepeNo ratings yet
- Module 5 - Conception NOTESDocument4 pagesModule 5 - Conception NOTESKisha BethelNo ratings yet
- Chapter 3 Stages of Fetal DevelopmentDocument4 pagesChapter 3 Stages of Fetal DevelopmentJohn Dave V. VillarmenteNo ratings yet
- Early EmbryogenesisDocument29 pagesEarly Embryogenesishassan aryaniNo ratings yet
- OB Embryogenesis Fetal Development TransDocument5 pagesOB Embryogenesis Fetal Development TransMian SimporiosNo ratings yet
- EmbryologyDocument16 pagesEmbryologyNikkNo ratings yet
- (OBa) 1.4 Plcental GRWTH and Maturation (Marinas) - PacisDocument6 pages(OBa) 1.4 Plcental GRWTH and Maturation (Marinas) - PacisClyde Yuchengco Cu-unjiengNo ratings yet
- Uni FileDocument17 pagesUni Filemuqadar khanNo ratings yet
- Embryonic Adaptations and Formation of Fetal Membranes Placentations and DeciduaeDocument69 pagesEmbryonic Adaptations and Formation of Fetal Membranes Placentations and DeciduaeApril MarieNo ratings yet
- PlacentaDocument24 pagesPlacentaNibedita 2015No ratings yet
- Animal Reproduction and Development: Stages of Development: Instructor: Ma. Christine E. IbayDocument17 pagesAnimal Reproduction and Development: Stages of Development: Instructor: Ma. Christine E. IbayCruella MajoNo ratings yet
- The Process of ConceptionDocument15 pagesThe Process of ConceptionJobelyn Dela CruzNo ratings yet
- St. Luke's College of Medicine - William H. Quasha Memorial: EmbryologyDocument23 pagesSt. Luke's College of Medicine - William H. Quasha Memorial: EmbryologyMavic VillanuevaNo ratings yet
- Fertilization &implantationDocument30 pagesFertilization &implantationAzza100% (1)
- 2008 - Huppertz - The Anatomy of The Normal PlacentaDocument8 pages2008 - Huppertz - The Anatomy of The Normal Placentaиick LooяNo ratings yet
- Pathology of Trophoblastic DiseaseDocument5 pagesPathology of Trophoblastic Disease2012100% (2)
- Midterm - Ob Normal LectureDocument44 pagesMidterm - Ob Normal LectureLeslie John PalaposNo ratings yet
- Fetal Development: Ms - Virgina Varghese and DR - SoniyaDocument37 pagesFetal Development: Ms - Virgina Varghese and DR - Soniyaalmayasa2002No ratings yet
- Placenta PDFDocument22 pagesPlacenta PDFbookaccountNo ratings yet
- Understanding Implantation Window, A Crucial Phenomenon: ReviewDocument5 pagesUnderstanding Implantation Window, A Crucial Phenomenon: ReviewgilanoNo ratings yet
- 45 HypospadiaDocument50 pages45 HypospadiaMarcella SaputraNo ratings yet
- Carnige Stages EmbryologyDocument2 pagesCarnige Stages EmbryologyDark Melanin Fineapple XoXoNo ratings yet
- SAQ EmbryologyDocument9 pagesSAQ EmbryologyShilpa DuttaNo ratings yet
- FertilizationDocument21 pagesFertilizationRashmi GoswamiNo ratings yet
- Embryology - The First WeekDocument51 pagesEmbryology - The First WeekLugembe MasolaNo ratings yet
- Second Week of Development: Bilaminar Germ Disc: CavityDocument19 pagesSecond Week of Development: Bilaminar Germ Disc: CavityAffry YannyNo ratings yet
- Lec 3Document9 pagesLec 3ibrahim.21hm32No ratings yet
- System InformationDocument547 pagesSystem Informationesmerova6735No ratings yet
- Brand ImageDocument2 pagesBrand Imagedollys59No ratings yet
- Lab Guide: Musculoskeletal AssessmentDocument6 pagesLab Guide: Musculoskeletal AssessmentDaisy MellaNo ratings yet
- Bengaluru BDA RMP 2031 PD Index MapDocument206 pagesBengaluru BDA RMP 2031 PD Index MapmyskmeNo ratings yet
- Sample Size Determination and Confidence Interval Derivation For Exponential DistributionDocument6 pagesSample Size Determination and Confidence Interval Derivation For Exponential DistributionIsmael NeuNo ratings yet
- Ayaz Ahmed SoomroDocument9 pagesAyaz Ahmed SoomroNoman RathoreNo ratings yet
- Decision Tree PrimerDocument42 pagesDecision Tree PrimerMuzzamil JanjuaNo ratings yet
- US Army Medical Course MD0363100 Electrosurgical Apparatus PDFDocument36 pagesUS Army Medical Course MD0363100 Electrosurgical Apparatus PDFpeterwolf67No ratings yet
- Oc Ik 100008Document1 pageOc Ik 100008Jagjeet SinghNo ratings yet
- HSE Manager JDDocument2 pagesHSE Manager JDRukun SinagaNo ratings yet
- Revealed Comparative AdvantageDocument5 pagesRevealed Comparative AdvantageiamrahulkumarNo ratings yet
- NY Mid-Eastern Group - Aug 2010Document3 pagesNY Mid-Eastern Group - Aug 2010CAP History LibraryNo ratings yet
- Penilaian Kelayakan Usaha Mikro Dengan Kredit Skoring Dan Pengaruhnya Terhadap Pembiayaan Bermasalah Best Practice Lembaga Keuangan Di IndonesiaDocument12 pagesPenilaian Kelayakan Usaha Mikro Dengan Kredit Skoring Dan Pengaruhnya Terhadap Pembiayaan Bermasalah Best Practice Lembaga Keuangan Di IndonesiaRiantriaNo ratings yet
- Tesla - Tunguska Explosion 1908 PDFDocument9 pagesTesla - Tunguska Explosion 1908 PDFMircea Gabriel BalanNo ratings yet
- Critical Issue Leisha CavallaroDocument8 pagesCritical Issue Leisha Cavallaroapi-216287146No ratings yet
- Product Selector Guide Marine Protective Coatings en 196830Document1 pageProduct Selector Guide Marine Protective Coatings en 196830wilberizquierdo1No ratings yet
- Fundraising Guide For Rescue TeamsDocument5 pagesFundraising Guide For Rescue TeamsDecisions For HeroesNo ratings yet
- Tutorial 5 - Flexural Members - Lateral Torsional BucklingDocument32 pagesTutorial 5 - Flexural Members - Lateral Torsional BucklingChan Keng ChunNo ratings yet
- IoT-Based Water Monitoring SystemDocument5 pagesIoT-Based Water Monitoring SystemManuel Luis Delos SantosNo ratings yet
- MCAD ManualDocument38 pagesMCAD ManualsureshrnalNo ratings yet
- Resume ManikandanDocument3 pagesResume ManikandanPMANIKANDANSVNNo ratings yet
- Bachelor of Business Administration: Dr. Saranleen Kaur (Associate Professor) Varun Kashyap (Co-Founder, Letsendorse)Document41 pagesBachelor of Business Administration: Dr. Saranleen Kaur (Associate Professor) Varun Kashyap (Co-Founder, Letsendorse)Yatik GoyalNo ratings yet
- List of Dealers Selected From Cuttack I Range For Tax Audit During 2011-12Document24 pagesList of Dealers Selected From Cuttack I Range For Tax Audit During 2011-12rchowdhury_10No ratings yet
- Xtream 18Document4 pagesXtream 18mhmdmhmood1770100% (1)
- GRADE 9-National Reading ProgramDocument2 pagesGRADE 9-National Reading ProgramJulius Bayaga100% (1)
- Orca Share Media1676505355563 7031773118863093717Document42 pagesOrca Share Media1676505355563 7031773118863093717Charls Aron ReyesNo ratings yet
- Anti LeproticDocument9 pagesAnti LeproticMeenakshi shARMANo ratings yet
- Chapter 1 and Chapter 2 PowerpointDocument14 pagesChapter 1 and Chapter 2 Powerpointapi-252892423No ratings yet
- Production Technology of Cow PeaDocument20 pagesProduction Technology of Cow PeaMUHAMMAD AQEELNo ratings yet
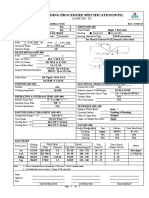
- Welding Procedure Specification (WPS) : (Asme Sec. Ix)Document1 pageWelding Procedure Specification (WPS) : (Asme Sec. Ix)Ahmed Lepda100% (1)