You might also like
- Barcode Sticker Request FormDocument2 pagesBarcode Sticker Request FormElvisPreslii59% (17)
- Modification FormDocument2 pagesModification Formshivamsolanki373No ratings yet
- Angel Broking: Account Details Addition / Modification / Deletion Request FormDocument1 pageAngel Broking: Account Details Addition / Modification / Deletion Request FormSushil VermaNo ratings yet
- Angel Broking Pvt. Ltd. Angel Commodities Broking Pvt. LTDDocument2 pagesAngel Broking Pvt. Ltd. Angel Commodities Broking Pvt. LTDManishSankrityayanNo ratings yet
- Form A PDFDocument2 pagesForm A PDFSundar SethNo ratings yet
- Customer Maintenance Form ADocument2 pagesCustomer Maintenance Form AWelkin SkyNo ratings yet
- Account Opening FormDocument22 pagesAccount Opening FormTarun BhardwajNo ratings yet
- Account Details Addition / Modification Request Form (KRA / Trading / DP A/c)Document1 pageAccount Details Addition / Modification Request Form (KRA / Trading / DP A/c)Pankaj AgarwalNo ratings yet
- Application Form b2b Msme July19Document7 pagesApplication Form b2b Msme July19Vishal Kumar SoniNo ratings yet
- Request Form For Changes in Demographics PDFDocument2 pagesRequest Form For Changes in Demographics PDFAmit Gothi0% (1)
- Application For General Changes: (Kindly Fill in Block Letter and Use Black Ink)Document2 pagesApplication For General Changes: (Kindly Fill in Block Letter and Use Black Ink)Nithin K ReethanNo ratings yet
- Module 2 - Technical AnalysisDocument3 pagesModule 2 - Technical AnalysisManmohan TiwariNo ratings yet
- Purchase Order Form TemplateDocument1 pagePurchase Order Form TemplateSuratman Blanck MandhoNo ratings yet
- Common Alteration Form (Caf) : Ddmmyyy YDocument2 pagesCommon Alteration Form (Caf) : Ddmmyyy YSonuNo ratings yet
- Standing Order Application / Information Update FormDocument1 pageStanding Order Application / Information Update FormЛена КиселеваNo ratings yet
- Major Alterations Form.Document1 pageMajor Alterations Form.ASHWINI BHOSALENo ratings yet
- Resident To Nro Conversion FormDocument3 pagesResident To Nro Conversion FormAbhiruchiNo ratings yet
- Yes Bank Changes in Demographics June-2023Document2 pagesYes Bank Changes in Demographics June-2023prashant agarwalNo ratings yet
- Annexure To Connect Life Proposal v6.0Document1 pageAnnexure To Connect Life Proposal v6.0Aryan AgarwalNo ratings yet
- Standardized Customer Request FormDocument7 pagesStandardized Customer Request FormSimar100% (1)
- Application Form AlterationsDocument2 pagesApplication Form AlterationsSonu SinghNo ratings yet
- Minor Alteration Form - Client PDFDocument2 pagesMinor Alteration Form - Client PDFSonu SinghNo ratings yet
- B2B Reloadable Account FormDocument6 pagesB2B Reloadable Account FormQamarNo ratings yet
- Wiretransoutp BlankDocument1 pageWiretransoutp BlankAdv Kunal KapoorNo ratings yet
- Policy Change Form PDFDocument2 pagesPolicy Change Form PDFSGA PHNo ratings yet
- Sbi Home Loan Application FormDocument5 pagesSbi Home Loan Application FormDhawan SandeepNo ratings yet
- Account details update requestDocument1 pageAccount details update requestvickyNo ratings yet
- Re Kyc Form PDFDocument2 pagesRe Kyc Form PDFInter 4DMNo ratings yet
- CustomerDocument2 pagesCustomerAmit KauriNo ratings yet
- Eage Banking Change of Address FormDocument2 pagesEage Banking Change of Address Formalways4gudduNo ratings yet
- Registration Form Cum Mandate For Electronic Clearing Services (Ecs) /direct Debit/NachDocument2 pagesRegistration Form Cum Mandate For Electronic Clearing Services (Ecs) /direct Debit/NachG.R.AzhaguvelSaranya Professor MechanicalNo ratings yet
- Customer Request FormDocument2 pagesCustomer Request FormJ ANo ratings yet
- Customer Request FormDocument2 pagesCustomer Request FormJ ANo ratings yet
- Customer Request Form UpdateDocument2 pagesCustomer Request Form UpdateJ ANo ratings yet
- Customer Request Form UpdateDocument2 pagesCustomer Request Form UpdateSaidi ReddyNo ratings yet
- PAN BASED NACH MANDATE CUM SIP REGISTRATIONDocument2 pagesPAN BASED NACH MANDATE CUM SIP REGISTRATIONDevesh SinghNo ratings yet
- HDFC FormDocument2 pagesHDFC Formapi-3726365100% (2)
- Request For Change in Custo Er Details M: Change/Update Contact Details - Residence/Office/Mobile No./ Email IDDocument2 pagesRequest For Change in Custo Er Details M: Change/Update Contact Details - Residence/Office/Mobile No./ Email IDPrakash SinghNo ratings yet
- Create Vendor RequestDocument2 pagesCreate Vendor RequestRafika LubisNo ratings yet
- Account Details Modification Request FormDocument2 pagesAccount Details Modification Request FormRajkumar manokaranNo ratings yet
- Vendor - Form CopDocument1 pageVendor - Form CopMaaz KhanNo ratings yet
- Arf - 2018Document6 pagesArf - 2018Vipin GargNo ratings yet
- Apply - For - Dealership - Application Form PDFDocument15 pagesApply - For - Dealership - Application Form PDFabhishekNo ratings yet
- Email FormDocument2 pagesEmail Formajaynigam25No ratings yet
- Request For Change in Policy Details Form English 120816Document1 pageRequest For Change in Policy Details Form English 120816Priya SelvarajNo ratings yet
- Vehicle Insurance Certificate in IndiaDocument2 pagesVehicle Insurance Certificate in IndiaED STORYNo ratings yet
- Registration Form Cum Mandate For Electronic Clearing Services (Ecs) /direct Debit/NachDocument2 pagesRegistration Form Cum Mandate For Electronic Clearing Services (Ecs) /direct Debit/NachPatel DipenNo ratings yet
- service-request-form DBS BankDocument3 pagesservice-request-form DBS BanketishreddyNo ratings yet
- NACH V1.3 - 29122017 - For Preferred DateDocument2 pagesNACH V1.3 - 29122017 - For Preferred DateMadhumita DuttaNo ratings yet
- Standing Instructions Form Internal TransferDocument2 pagesStanding Instructions Form Internal TransferEdgar YoungNo ratings yet
- Savings & Current AccountsDocument6 pagesSavings & Current AccountsAXIS Section GNo ratings yet
- Fixed/Recurring Deposit: Type of AccountDocument4 pagesFixed/Recurring Deposit: Type of Accountking bestNo ratings yet
- Freelook Request Format: Date: Policy NumberDocument2 pagesFreelook Request Format: Date: Policy NumberSatish BojjawarNo ratings yet
- Application Form - TMB Econnect (Corporate) : Regd - Office: 57, V.E. Road Thoothukudi - 628 002 Website: WWW - Tmb.inDocument4 pagesApplication Form - TMB Econnect (Corporate) : Regd - Office: 57, V.E. Road Thoothukudi - 628 002 Website: WWW - Tmb.inPrabu /MWNo ratings yet
- Fixed/Recurring Deposit: Type of AccountDocument4 pagesFixed/Recurring Deposit: Type of AccountHarpreet0gjgkbkv KaurNo ratings yet
- Fixed Deposit Account Opening Form For Existing CustomersDocument4 pagesFixed Deposit Account Opening Form For Existing Customershero romeoNo ratings yet
- Standing Order Request FormDocument2 pagesStanding Order Request FormMonisha ShanmuNo ratings yet
- Vendor Declaration FormDocument2 pagesVendor Declaration FormMuazzamAliNo ratings yet
- The Contractor Payment Application Audit: Guidance for Auditing AIA Documents G702 & G703From EverandThe Contractor Payment Application Audit: Guidance for Auditing AIA Documents G702 & G703No ratings yet
- Advisor Contest OND-18Document14 pagesAdvisor Contest OND-18dharam singhNo ratings yet
- BenefitIllustartion Early Cash Plan 15102022173146Document2 pagesBenefitIllustartion Early Cash Plan 15102022173146dharam singhNo ratings yet
- Company Cancelled ChequeDocument1 pageCompany Cancelled Chequedharam singhNo ratings yet
- Nominee Change FormatDocument4 pagesNominee Change Formatdharam singhNo ratings yet
- Parul Sharma BIpdfDocument2 pagesParul Sharma BIpdfdharam singhNo ratings yet
- Proposal Form SLICDocument4 pagesProposal Form SLICdharam singhNo ratings yet
- Common Proposal Form: Tata AIA Life Insurance Company LimitedDocument7 pagesCommon Proposal Form: Tata AIA Life Insurance Company Limiteddharam singhNo ratings yet
- Benefit Illustration For: Policy Year Total Annualised Premiums Paid Till Date Guaranteed Special Surrender BenefitDocument1 pageBenefit Illustration For: Policy Year Total Annualised Premiums Paid Till Date Guaranteed Special Surrender Benefitdharam singhNo ratings yet
- Life Insurance Plan BenefitsDocument1 pageLife Insurance Plan Benefitsdharam singhNo ratings yet
- Manan Bansal BI 20kDocument2 pagesManan Bansal BI 20kdharam singhNo ratings yet
- Life insurance plan for Mr. AggarwalDocument1 pageLife insurance plan for Mr. Aggarwaldharam singhNo ratings yet
- Reya BI 25kDocument2 pagesReya BI 25kdharam singhNo ratings yet
- Sip 1.5l Surbhi GargDocument2 pagesSip 1.5l Surbhi Gargdharam singhNo ratings yet
- Sip 1.5l Surbhi GargDocument2 pagesSip 1.5l Surbhi Gargdharam singhNo ratings yet
- Key Features: Why SBI Life - Smart Champ Insurance Plan?Document2 pagesKey Features: Why SBI Life - Smart Champ Insurance Plan?dharam singhNo ratings yet
- Benefit Illustration For Shriram Life Golden Premier Saver Plan 128N088V02Document2 pagesBenefit Illustration For Shriram Life Golden Premier Saver Plan 128N088V02dharam singhNo ratings yet
- Applicable To All Fcs of Agency ChannelDocument5 pagesApplicable To All Fcs of Agency Channeldharam singhNo ratings yet
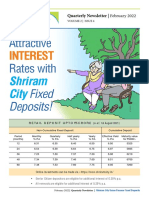
- Attractive Rates With: InterestDocument4 pagesAttractive Rates With: Interestdharam singhNo ratings yet
- Best Fixed Deposit Rates from Top BanksDocument1 pageBest Fixed Deposit Rates from Top Banksdharam singhNo ratings yet
- Dimension Group building commercial area coupon rating yield face value securitiesDocument1 pageDimension Group building commercial area coupon rating yield face value securitiesdharam singhNo ratings yet
- Star Women Care Insurance Policy SummaryDocument2 pagesStar Women Care Insurance Policy Summarydharam singhNo ratings yet
- To, Shriram Life Insurance Company Limited.: Customer Mandate Cum Declaration Form For New BusinessDocument1 pageTo, Shriram Life Insurance Company Limited.: Customer Mandate Cum Declaration Form For New Businessdharam singhNo ratings yet
- D D M M Y Y Y Y D D M M Y Y Y Y D D M M Y Y Y Y: IFD Code: Independent Financial Distributor (Ifd) Registration FormDocument7 pagesD D M M Y Y Y Y D D M M Y Y Y Y D D M M Y Y Y Y: IFD Code: Independent Financial Distributor (Ifd) Registration Formdharam singhNo ratings yet
- The Ultimate SaaS Metrics Cheat SheetDocument2 pagesThe Ultimate SaaS Metrics Cheat SheetTạ Thị Mai - VIVANo ratings yet
- Liquidation Process ExplainedDocument7 pagesLiquidation Process ExplainedAhmad KhanNo ratings yet
- Mortgage Lab pg1Document3 pagesMortgage Lab pg1api-457616660No ratings yet
- BIWS Atlassian 3 Statement Model - VFDocument8 pagesBIWS Atlassian 3 Statement Model - VFJohnny BravoNo ratings yet
- FAR 6.2MC - Noncurrent Liabilities (Part 1) Notes and Loans PayableDocument4 pagesFAR 6.2MC - Noncurrent Liabilities (Part 1) Notes and Loans Payablekateangel ellesoNo ratings yet
- Internal Audit Procedures ManualDocument11 pagesInternal Audit Procedures ManualLeizza Ni Gui DulaNo ratings yet
- Transaction Statement: Account Number: 1632104000026770 Date: 2023-11-08 Currency: INRDocument5 pagesTransaction Statement: Account Number: 1632104000026770 Date: 2023-11-08 Currency: INRwww.manjsahuNo ratings yet
- Final PPT of IndusInd BankDocument14 pagesFinal PPT of IndusInd BanktruptiNo ratings yet
- Deed of PartnershipDocument4 pagesDeed of Partnershipsince1978nsNo ratings yet
- IU Student Bank StatementDocument1 pageIU Student Bank StatementHasnain AliNo ratings yet
- Credit Transactions Reviewer PDFDocument5 pagesCredit Transactions Reviewer PDFJustineNo ratings yet
- Financial ServicesDocument10 pagesFinancial ServicesDinesh Sugumaran100% (4)
- CH04 PPTDocument155 pagesCH04 PPTAbd EL Samee3No ratings yet
- A Reformulation: Intel CorporationDocument15 pagesA Reformulation: Intel Corporationmnhasan150No ratings yet
- Unit 5 PomDocument32 pagesUnit 5 PomDebasis BanerjeeNo ratings yet
- Investment in Equity Securities - IA1Document17 pagesInvestment in Equity Securities - IA1dumpyforhimNo ratings yet
- Glitter and Gold StudioDocument4 pagesGlitter and Gold Studiolaale dijaanNo ratings yet
- Members and ShareholdersDocument2 pagesMembers and Shareholdersimad0% (2)
- Bill of Exchange MaybankDocument3 pagesBill of Exchange MaybankBuayaz GamingNo ratings yet
- Rental Agreement Format ChennaiDocument4 pagesRental Agreement Format Chennaisundarji sundararajuluNo ratings yet
- Forms of Business OrganizationDocument26 pagesForms of Business Organizationtrustme77No ratings yet
- Cushman - Wakefield - MarketBeat - Mumbai Office - Q4 - 2020 - 1634745571430Document2 pagesCushman - Wakefield - MarketBeat - Mumbai Office - Q4 - 2020 - 1634745571430Aditya UdaniNo ratings yet
- World Country Indicator Data ListDocument161 pagesWorld Country Indicator Data ListPrzemysław BanaśNo ratings yet
- Conceptual Framework Accounting Standards: Summary ofDocument5 pagesConceptual Framework Accounting Standards: Summary of버니 모지코No ratings yet
- Microsoft Business Strategy 101Document17 pagesMicrosoft Business Strategy 101Chinmay Chauhan50% (2)
- Annual Report MERK 2012Document108 pagesAnnual Report MERK 2012StefanyNo ratings yet
- FinancialManagement Mplte ChoiceDocument18 pagesFinancialManagement Mplte ChoiceCrish NaNo ratings yet
- Priority Payment: The Status For Payment 78735WQ007TU Is: Pending AuthorisationDocument3 pagesPriority Payment: The Status For Payment 78735WQ007TU Is: Pending AuthorisationShohag RaihanNo ratings yet
- Outlining Period-End Closing For A Product Cost Collector: Unit 3 Lesson 1Document2 pagesOutlining Period-End Closing For A Product Cost Collector: Unit 3 Lesson 1s4hanamm 1809No ratings yet
- Exchange Summary Volume and Open Interest Interest Rates FuturesDocument2 pagesExchange Summary Volume and Open Interest Interest Rates FuturesavadcsNo ratings yet