You might also like
- Complementary and Alternative Medical Lab Testing Part 5: GastrointestinalFrom EverandComplementary and Alternative Medical Lab Testing Part 5: GastrointestinalNo ratings yet
- Refractory Gastroesophageal Reflux Disease Diagnosis and ManagementDocument12 pagesRefractory Gastroesophageal Reflux Disease Diagnosis and Managementg-46005995No ratings yet
- Richter 2017Document10 pagesRichter 2017Rachel RiosNo ratings yet
- Gastroparesis Updates On Pathogenesis and Management: ReviewDocument11 pagesGastroparesis Updates On Pathogenesis and Management: Reviewputri permata SariNo ratings yet
- JGastr10 GERDDocument8 pagesJGastr10 GERDEnderNo ratings yet
- Pathophysiology of Functional Dyspepsia: ReviewDocument6 pagesPathophysiology of Functional Dyspepsia: ReviewTobi JulfiartoNo ratings yet
- Optimal Management of Severe Symptomatic Gastroesophageal Reflux DiseaseDocument17 pagesOptimal Management of Severe Symptomatic Gastroesophageal Reflux DiseaseGianella VegasNo ratings yet
- Prevalence of Gastroesophageal Reflux Disease (GERD) in Dyspepsia Patients in Primary Referral HospitalDocument6 pagesPrevalence of Gastroesophageal Reflux Disease (GERD) in Dyspepsia Patients in Primary Referral HospitalAbrar TaraNo ratings yet
- Pathophysiology of Functional Dyspepsia: ReviewDocument6 pagesPathophysiology of Functional Dyspepsia: ReviewRaisa AlifiaNo ratings yet
- CTC Gerd FinalDocument36 pagesCTC Gerd FinaljaipreyraNo ratings yet
- Exploring The Spectrum of GERD: Myths and Realities: Special ArticleDocument9 pagesExploring The Spectrum of GERD: Myths and Realities: Special ArticleedopriyantomoNo ratings yet
- SSAT Maintenance of Certification: Literature Review On Gastroesophageal Reflux Disease and Hiatal HerniaDocument5 pagesSSAT Maintenance of Certification: Literature Review On Gastroesophageal Reflux Disease and Hiatal HerniaGosadorNo ratings yet
- Role of Acid and Weakly Acidic Reflux in Gastroesophageal Reflux Disease Off Proton Pump Inhibitor TherapyDocument7 pagesRole of Acid and Weakly Acidic Reflux in Gastroesophageal Reflux Disease Off Proton Pump Inhibitor TherapyDumitru VladNo ratings yet
- Prevalensi 1Document6 pagesPrevalensi 1sahama2508No ratings yet
- Erge NejmDocument10 pagesErge Nejmliz salcedoNo ratings yet
- Pi Is 1542356517313071Document12 pagesPi Is 1542356517313071Julenda CintarinovaNo ratings yet
- Aga: Clinical Practice UpdateDocument12 pagesAga: Clinical Practice UpdatextineNo ratings yet
- Validation of The Gerdq Questionnaire For The Diagnosis of Gastro-Oesophageal Re Ux DiseaseDocument9 pagesValidation of The Gerdq Questionnaire For The Diagnosis of Gastro-Oesophageal Re Ux DiseaseSharan KaurNo ratings yet
- Associations of Circulating Gut Hormone and Adipocytokine Levels With The Spectrum of Gastroesophageal Reflux DiseaseDocument12 pagesAssociations of Circulating Gut Hormone and Adipocytokine Levels With The Spectrum of Gastroesophageal Reflux DiseasekasabeNo ratings yet
- GerdDocument10 pagesGerdMulia NtiNo ratings yet
- Makalah Pleno B 16 (GERD)Document17 pagesMakalah Pleno B 16 (GERD)jack gantengNo ratings yet
- Eight Weeks of Esomeprazole Therapy Reduces Symptom Relapse, Compared With 4 Weeks, in Patients With Los Angeles Grade A or B Erosive EsophagitisDocument9 pagesEight Weeks of Esomeprazole Therapy Reduces Symptom Relapse, Compared With 4 Weeks, in Patients With Los Angeles Grade A or B Erosive EsophagitisBeau PhatruetaiNo ratings yet
- Nejmcp 2114026Document10 pagesNejmcp 2114026Cristina Adriana PopaNo ratings yet
- Contenidos: Calculadoras Interacciones de FármacosDocument28 pagesContenidos: Calculadoras Interacciones de FármacosFredyRodriguezGarciaNo ratings yet
- Nejmcp 2114026Document10 pagesNejmcp 2114026Engin AltınkayaNo ratings yet
- HTTPS:WWW Ncbi NLM Nih gov:pmc:articles:PMC4133436:pdf:WJGPT-5-105Document9 pagesHTTPS:WWW Ncbi NLM Nih gov:pmc:articles:PMC4133436:pdf:WJGPT-5-105Doni SaragihNo ratings yet
- Efficacy of Transoral Fundoplication Vs Omeprazole For Treatment of Regurgitation in A Randomized Controlled Trial-1Document15 pagesEfficacy of Transoral Fundoplication Vs Omeprazole For Treatment of Regurgitation in A Randomized Controlled Trial-1-Yohanes Firmansyah-No ratings yet
- Document PDF MedDocument1 pageDocument PDF MedCOLA [Chaîne Officielle]No ratings yet
- (2021) GerdDocument23 pages(2021) Gerdadri20121989No ratings yet
- Perspectiva Eap PDFDocument11 pagesPerspectiva Eap PDFAndres Felipe Rojas RodriguezNo ratings yet
- Ghrelin Gene Polymorphisms in Irritable Bowel Syndrome: To The Point ArticleDocument6 pagesGhrelin Gene Polymorphisms in Irritable Bowel Syndrome: To The Point Articlecheese schedarNo ratings yet
- 2 Heartburn PDFDocument8 pages2 Heartburn PDFjeyaprakash jayaramanNo ratings yet
- 2003 A Validated Symptoms Questionnaire Chinese GERDQ For Thediagnosis of Gastro Oesophageal Reflux Disease in The ChinesepopulationDocument7 pages2003 A Validated Symptoms Questionnaire Chinese GERDQ For Thediagnosis of Gastro Oesophageal Reflux Disease in The ChinesepopulationAhmad Yar SukheraNo ratings yet
- Primer: Gastro-Oesophageal Reflux DiseaseDocument23 pagesPrimer: Gastro-Oesophageal Reflux Diseasejcacia17No ratings yet
- Functional (Non-Ulcer) Dyspepsia and Gastroesophageal Refl Ux Disease: One Not Two Diseases ?Document3 pagesFunctional (Non-Ulcer) Dyspepsia and Gastroesophageal Refl Ux Disease: One Not Two Diseases ?Reynalth Andrew SinagaNo ratings yet
- Gejala Dan Penatalaksanaan Penyakit Refluks Gastroesofageal (GERD)Document17 pagesGejala Dan Penatalaksanaan Penyakit Refluks Gastroesofageal (GERD)irmsNo ratings yet
- Impact of Percutaneous Endoscopic Gastrostomy On Gastroesophageal Reflux and Gastric Emptying in Pediatric Patients GER and Gastric Emptying After PEGDocument5 pagesImpact of Percutaneous Endoscopic Gastrostomy On Gastroesophageal Reflux and Gastric Emptying in Pediatric Patients GER and Gastric Emptying After PEGInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Combination of PPI With A Prokinetic Drug in Gastroesophageal Reflux DiseaseDocument19 pagesCombination of PPI With A Prokinetic Drug in Gastroesophageal Reflux DiseaseFebyan AbotNo ratings yet
- Organic Versus Functional: DyspepsiaDocument16 pagesOrganic Versus Functional: DyspepsiahelenaNo ratings yet
- SCArticle4 PDFDocument9 pagesSCArticle4 PDFMuhammad Wim AdhitamaNo ratings yet
- Approach To Uninvestigated DyspepsiaDocument18 pagesApproach To Uninvestigated DyspepsiaAshish SatyalNo ratings yet
- Acid Related DisordersDocument18 pagesAcid Related DisordersMinto SanjoyoNo ratings yet
- Diagnostic Assessment of Diabetic Gastroparesis: Andrea S. Shin and Michael CamilleriDocument7 pagesDiagnostic Assessment of Diabetic Gastroparesis: Andrea S. Shin and Michael CamillerinadiraNo ratings yet
- Konsensus GerdDocument44 pagesKonsensus GerdPink Pinky cimutNo ratings yet
- Non-Pharmacologic Treatment Strategies in Gastroesophageal Reflux DiseaseDocument5 pagesNon-Pharmacologic Treatment Strategies in Gastroesophageal Reflux DiseaseEmirgibraltarNo ratings yet
- Gastroesophageal Reflux Disease Control of Symptoms, Prevention of ComplicationsDocument9 pagesGastroesophageal Reflux Disease Control of Symptoms, Prevention of ComplicationsTiurma SibaraniNo ratings yet
- Functional Heartburn. An Underrecognized Cause of PPI-refractory Symptoms 2019Document8 pagesFunctional Heartburn. An Underrecognized Cause of PPI-refractory Symptoms 2019Ricardo Robles AlfaroNo ratings yet
- Shinozaki Japan VanoprazanDocument9 pagesShinozaki Japan Vanoprazansahama2508No ratings yet
- WJGPT 5 105 PDFDocument9 pagesWJGPT 5 105 PDFMeldhaNo ratings yet
- Journal of Neurogastroenterology and Motility: Young-Gun Kim, Choong-Kyun Noh, and Kwang Jae LeeDocument8 pagesJournal of Neurogastroenterology and Motility: Young-Gun Kim, Choong-Kyun Noh, and Kwang Jae LeeFhienovdhieyHa ThreuvHyNo ratings yet
- Article: Short-Term Treatment With Proton-Pump Inhibitors As A Test For Gastroesophageal Reflux DiseaseDocument11 pagesArticle: Short-Term Treatment With Proton-Pump Inhibitors As A Test For Gastroesophageal Reflux DiseaseAsni Putra JayaNo ratings yet
- Gastroesophagealreflux Diseaseafterbariatric Procedures: Maria S. Altieri,, Aurora D. PryorDocument13 pagesGastroesophagealreflux Diseaseafterbariatric Procedures: Maria S. Altieri,, Aurora D. PryormaryNo ratings yet
- Functional Dyspepsia: Advances in Diagnosis and Therapy: ReviewDocument9 pagesFunctional Dyspepsia: Advances in Diagnosis and Therapy: Reviewjenny puentesNo ratings yet
- Dispepsia 1Document16 pagesDispepsia 1nainggolan Debora15No ratings yet
- Review: Epidemiology, Mechanisms, and Management of Diabetic GastroparesisDocument8 pagesReview: Epidemiology, Mechanisms, and Management of Diabetic GastroparesisIrma KurniawatiNo ratings yet
- RESEARCH - GERD-Q Score DLBS2411-hiresDocument8 pagesRESEARCH - GERD-Q Score DLBS2411-hiresNanangNo ratings yet
- Diagnosis and Management of Functional HeartburnDocument9 pagesDiagnosis and Management of Functional Heartburnal ghiffari muhammad rayhanNo ratings yet
- Gerd GuidelineDocument8 pagesGerd Guidelinets8166No ratings yet
- Combined Slides For Resources RB 2Document65 pagesCombined Slides For Resources RB 2Maria Fernanda Cueto OrtechoNo ratings yet
- GI - Pathophysiology, Evaluation, and Treatment of BloatingDocument11 pagesGI - Pathophysiology, Evaluation, and Treatment of BloatingTriLightNo ratings yet
- TK Sepsis Karena Kandidiasis InvasifDocument23 pagesTK Sepsis Karena Kandidiasis InvasifsamudraandiNo ratings yet
- Efficacy and Safety of Remdesivir As A Potential Antiviral Therapy For Covid-19 An Evidence-Based Case ReportDocument18 pagesEfficacy and Safety of Remdesivir As A Potential Antiviral Therapy For Covid-19 An Evidence-Based Case ReportsamudraandiNo ratings yet
- HYPOKALEMIADocument41 pagesHYPOKALEMIAsamudraandiNo ratings yet
- Cyclosporin in Idiopathic Glomerular Disease AssocDocument20 pagesCyclosporin in Idiopathic Glomerular Disease AssocsamudraandiNo ratings yet
- Case Report A 48 Years Old Male With Wide QRS Complex TachycardiaDocument2 pagesCase Report A 48 Years Old Male With Wide QRS Complex TachycardiasamudraandiNo ratings yet
- Rheumatic Heart Disease With Complication of Atrial FibrillationDocument3 pagesRheumatic Heart Disease With Complication of Atrial FibrillationsamudraandiNo ratings yet
- Abstract NSTEMI + OMIDocument3 pagesAbstract NSTEMI + OMIsamudraandiNo ratings yet
- Sample Selection Criteria (Maximum of 4 Stars) : A A A A B B A BDocument4 pagesSample Selection Criteria (Maximum of 4 Stars) : A A A A B B A BsamudraandiNo ratings yet
- Cover LetterDocument2 pagesCover LettersamudraandiNo ratings yet
- WJG 25 418Document16 pagesWJG 25 418samudraandiNo ratings yet
- JGH 13174Document9 pagesJGH 13174samudraandiNo ratings yet
- 4-Metre Gait Speed As A Functional Outcome Measure in Patients With Chronic Obstructive Pulmonary Disease (COPD)Document3 pages4-Metre Gait Speed As A Functional Outcome Measure in Patients With Chronic Obstructive Pulmonary Disease (COPD)samudraandiNo ratings yet
- Pancreatic Tuberculosis Review ArticleDocument24 pagesPancreatic Tuberculosis Review ArticlesamudraandiNo ratings yet
- Semi Finals in Tle 2015Document3 pagesSemi Finals in Tle 2015LoraineTenorioNo ratings yet
- Implicit Explicit SignalsDocument8 pagesImplicit Explicit SignalsVersoza Nel100% (2)
- Fully Automatic Coffee Machine - Slimissimo - IB - SCOTT UK - 2019Document20 pagesFully Automatic Coffee Machine - Slimissimo - IB - SCOTT UK - 2019lazareviciNo ratings yet
- The Passion For Cacti and Other Succulents: June 2017Document140 pagesThe Passion For Cacti and Other Succulents: June 2017golf2010No ratings yet
- Food Taste Panel Evaluation Form 2Document17 pagesFood Taste Panel Evaluation Form 2Akshat JainNo ratings yet
- tGr12OM CheResoBookU78910Document110 pagestGr12OM CheResoBookU78910Jamunanantha PranavanNo ratings yet
- SP Essay 1Document14 pagesSP Essay 1api-511870420No ratings yet
- Biophoton RevolutionDocument3 pagesBiophoton RevolutionVyavasayaha Anita BusicNo ratings yet
- Straight LineDocument15 pagesStraight LineAyanNo ratings yet
- Nissan Copper LTDDocument11 pagesNissan Copper LTDankit_shahNo ratings yet
- Dawn of Solar PV CookingDocument5 pagesDawn of Solar PV CookingAbhinav AgrawalNo ratings yet
- Save Water SpeechDocument4 pagesSave Water SpeechHari Prakash Shukla0% (1)
- 18 Ray Optics Revision Notes QuizrrDocument108 pages18 Ray Optics Revision Notes Quizrraafaf.sdfddfaNo ratings yet
- Top Ten Myths About The BrainDocument5 pagesTop Ten Myths About The BrainfayazalamaligNo ratings yet
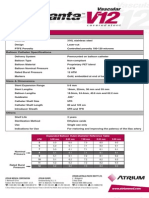
- Advanta V12 Data SheetDocument2 pagesAdvanta V12 Data SheetJuliana MiyagiNo ratings yet
- IV. Network Modeling, Simple SystemDocument16 pagesIV. Network Modeling, Simple SystemJaya BayuNo ratings yet
- RACI Matrix Design For Managing Stakeholders in PRDocument12 pagesRACI Matrix Design For Managing Stakeholders in PRRheza Nugraha Prabareswara100% (1)
- Circle The Best Answer A, B, C, D or EDocument4 pagesCircle The Best Answer A, B, C, D or Ewilder jackNo ratings yet
- Sika - Bitumen: Bitumen Emulsion Waterproof & Protective CoatingDocument3 pagesSika - Bitumen: Bitumen Emulsion Waterproof & Protective Coatingdinu69inNo ratings yet
- Presentation On 4G TechnologyDocument23 pagesPresentation On 4G TechnologyFresh EpicNo ratings yet
- DudjDocument4 pagesDudjsyaiful rinantoNo ratings yet
- Passenger Lift Alert - Health and Safety AuthorityDocument4 pagesPassenger Lift Alert - Health and Safety AuthorityReginald MaswanganyiNo ratings yet
- Emw 2007 FP 02093Document390 pagesEmw 2007 FP 02093boj87No ratings yet
- AKI in ChildrenDocument43 pagesAKI in ChildrenYonas AwgichewNo ratings yet
- C.Abdul Hakeem College of Engineering and Technology, Melvisharam Department of Aeronautical Engineering Academic Year 2020-2021 (ODD)Document1 pageC.Abdul Hakeem College of Engineering and Technology, Melvisharam Department of Aeronautical Engineering Academic Year 2020-2021 (ODD)shabeerNo ratings yet
- Course Syllabus: Course Code Course Title ECTS CreditsDocument3 pagesCourse Syllabus: Course Code Course Title ECTS CreditsHanaa HamadallahNo ratings yet
- World's Standard Model G6A!: Low Signal RelayDocument9 pagesWorld's Standard Model G6A!: Low Signal RelayEgiNo ratings yet
- Keiilf: Training ManualDocument53 pagesKeiilf: Training ManualGary GouveiaNo ratings yet
- Goliath 90 v129 eDocument129 pagesGoliath 90 v129 eerkanNo ratings yet
- Manual Wire Rope Winches Wall-Mounted Wire Rope Winch SW-W: Equipment and ProcessingDocument1 pageManual Wire Rope Winches Wall-Mounted Wire Rope Winch SW-W: Equipment and Processingdrg gocNo ratings yet
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Rating: 3 out of 5 stars3/5 (1)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (3)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (29)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (81)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 4 out of 5 stars4/5 (4)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (5)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (45)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (170)
- Summary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (61)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesFrom EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesRating: 4.5 out of 5 stars4.5/5 (1412)
- How to ADHD: The Ultimate Guide and Strategies for Productivity and Well-BeingFrom EverandHow to ADHD: The Ultimate Guide and Strategies for Productivity and Well-BeingRating: 1 out of 5 stars1/5 (1)
- The Marshmallow Test: Mastering Self-ControlFrom EverandThe Marshmallow Test: Mastering Self-ControlRating: 4.5 out of 5 stars4.5/5 (59)