You might also like
- COVID 19 Pandemic PlanDocument32 pagesCOVID 19 Pandemic PlanElspeth Kernebone83% (12)
- FOUNDATION COURSE IN MAKE-UP ARTISTRYDocument114 pagesFOUNDATION COURSE IN MAKE-UP ARTISTRYContract100% (1)
- Cupping TherapyDocument20 pagesCupping TherapyMohamed AttiaNo ratings yet
- Proposed COVID-19 Response PlanDocument12 pagesProposed COVID-19 Response PlanRabindra Raj PantaNo ratings yet
- iHFG Part B Community Health UnitDocument18 pagesiHFG Part B Community Health UnitEmmanuel OENo ratings yet
- CIDA Guidelines For Construction SitesDocument14 pagesCIDA Guidelines For Construction SitesAudithya KahawattaNo ratings yet
- NCM 119 Module Safety Part 2 Standards Lesson Safety National Quality Forum 2009Document59 pagesNCM 119 Module Safety Part 2 Standards Lesson Safety National Quality Forum 2009Maria Victoria A. PraxidesNo ratings yet
- Care Skill Assignment Nikhil PhilipDocument16 pagesCare Skill Assignment Nikhil PhilipMuhammad DanishNo ratings yet
- COVID-19 A Guide to Self Preparedness for Crisis Management: 1, #2From EverandCOVID-19 A Guide to Self Preparedness for Crisis Management: 1, #2Rating: 5 out of 5 stars5/5 (1)
- Hospital-Infection-Prevention-and-Control-Manual 2022Document349 pagesHospital-Infection-Prevention-and-Control-Manual 2022Jp Rizal IPCC100% (1)
- Infect Control ProceduresDocument94 pagesInfect Control ProceduresKabita123 NepzzNo ratings yet
- COVID-19 Key To Prevention & Survival: 1, #1From EverandCOVID-19 Key To Prevention & Survival: 1, #1Rating: 5 out of 5 stars5/5 (1)
- National immunization guidance during COVID-19 pandemicDocument59 pagesNational immunization guidance during COVID-19 pandemicchikoNo ratings yet
- Guidelines For The Management of COVID-19 in Health FacilitiesDocument35 pagesGuidelines For The Management of COVID-19 in Health FacilitiesherathhmasNo ratings yet
- COVID-19 Patient Friendly EbookDocument55 pagesCOVID-19 Patient Friendly EbookYarmand WaqarNo ratings yet
- Handbook of COVID19 Prevention and Treatment PDFDocument68 pagesHandbook of COVID19 Prevention and Treatment PDFZaw Min TunNo ratings yet
- Handbook of COVID 19 Prevention en Mobile PDFDocument68 pagesHandbook of COVID 19 Prevention en Mobile PDFIvonne Flores FernándezNo ratings yet
- Coronavirus Guidelines For BusinessDocument12 pagesCoronavirus Guidelines For BusinessBusinessTech100% (5)
- WHO 2019 nCoV Clinical 2021.1 EngDocument81 pagesWHO 2019 nCoV Clinical 2021.1 EngAmjad Ali AfridiNo ratings yet
- Screening and Triage of Patients With Suspected or Confirmed COVID-19Document24 pagesScreening and Triage of Patients With Suspected or Confirmed COVID-19LinaRizaNavalesMonteroNo ratings yet
- National Guidelines For Management of COVID-19 23 April-2020Document95 pagesNational Guidelines For Management of COVID-19 23 April-2020Bashir KabuyeNo ratings yet
- Pneumonia in Adults Diagnosis and Management PDF 35109868127173Document22 pagesPneumonia in Adults Diagnosis and Management PDF 35109868127173mshadadark100% (1)
- COVID-19 Guidance for Shared AccommodationDocument25 pagesCOVID-19 Guidance for Shared Accommodationalex_grgNo ratings yet
- Guidance Routine Immunization Services COVID 19 PandemicDocument12 pagesGuidance Routine Immunization Services COVID 19 PandemicNnnNo ratings yet
- National immunization guidance during COVID-19 pandemicDocument64 pagesNational immunization guidance during COVID-19 pandemickepegawaian RSUD CabangbunginNo ratings yet
- Full COVID-19 coverage for Filipino health workers and patientsDocument32 pagesFull COVID-19 coverage for Filipino health workers and patientsGeneXpert Lab LCPNo ratings yet
- Coronavirus (COVID-19) Cleaning Guidelines For Workplaces: Information For Business Owners, Managers and CleanersDocument62 pagesCoronavirus (COVID-19) Cleaning Guidelines For Workplaces: Information For Business Owners, Managers and CleanersindahNo ratings yet
- COVID-19 Healthcare Settings SummaryDocument27 pagesCOVID-19 Healthcare Settings SummaryBeugh RiveraNo ratings yet
- WHO 2019 NCoV Vaccines SAGE Background 2020.1 EngDocument28 pagesWHO 2019 NCoV Vaccines SAGE Background 2020.1 EngMaría Francisca SánchezNo ratings yet
- Covid19 Rapid Guideline Pneumonia in Adults in The CommunityDocument15 pagesCovid19 Rapid Guideline Pneumonia in Adults in The CommunityDusan OrescaninNo ratings yet
- COVID Guidelines Final.23.04.2020.r2 From CIDA - ICTADDocument14 pagesCOVID Guidelines Final.23.04.2020.r2 From CIDA - ICTADganaa haranNo ratings yet
- WASH Sector response to COVID-19 in Cox's BazarDocument15 pagesWASH Sector response to COVID-19 in Cox's BazarHonorat Brice. H.No ratings yet
- Clinical Guide For The Management and Care of Critically Ill Adults With COVID-19 During The Coronavirus PandemicDocument27 pagesClinical Guide For The Management and Care of Critically Ill Adults With COVID-19 During The Coronavirus PandemicPurwadi SujalmoNo ratings yet
- National COVID-19 Infection Prevention and Control GuidelinesDocument28 pagesNational COVID-19 Infection Prevention and Control GuidelinesiamdarnNo ratings yet
- COVID-19 - Infection Control For Persons With SARS-CoV-2 Infection - UpToDateDocument35 pagesCOVID-19 - Infection Control For Persons With SARS-CoV-2 Infection - UpToDateDuy Hùng HoàngNo ratings yet
- Pediatric Surgery IPC Guidance During COVID-19Document22 pagesPediatric Surgery IPC Guidance During COVID-19Dokter GamingNo ratings yet
- DSAMH Guidance For OTPs UPDATEDDocument13 pagesDSAMH Guidance For OTPs UPDATEDJoe AronsonNo ratings yet
- Coronavirus Disease 2019 (COVID-19) - Anesthetic Concerns, Including Airway Management and Infection ControlDocument32 pagesCoronavirus Disease 2019 (COVID-19) - Anesthetic Concerns, Including Airway Management and Infection ControlT GalenNo ratings yet
- WHO 2019 NCoV Clinical 2021.2 EngDocument116 pagesWHO 2019 NCoV Clinical 2021.2 EngRafail RustamovNo ratings yet
- Infection Prevention and Control During Health Care When Coronavirus Disease (COVID-19) Is Suspected or ConfirmedDocument13 pagesInfection Prevention and Control During Health Care When Coronavirus Disease (COVID-19) Is Suspected or ConfirmedDina PrilyaNo ratings yet
- IPC Module For COVID-19 For Frontline HCW - 20.3.2020Document40 pagesIPC Module For COVID-19 For Frontline HCW - 20.3.2020gourabNo ratings yet
- Coronavirus Disease 2019 Guidelines v1.1.Document33 pagesCoronavirus Disease 2019 Guidelines v1.1.S71% (7)
- Infection Prevention and Control For Seasonal Respiratory Infections in Health and Care SettingsDocument29 pagesInfection Prevention and Control For Seasonal Respiratory Infections in Health and Care Settingsmulyono ajiNo ratings yet
- Guidance For Setting Up A Virtual Supported Discharge Service For Covid 19Document20 pagesGuidance For Setting Up A Virtual Supported Discharge Service For Covid 19eimearNo ratings yet
- COVID-19 guidance managing deadDocument15 pagesCOVID-19 guidance managing deadBOSS 2049No ratings yet
- World Day For Safety and Health at Work 2020 - Stop The PandemicDocument52 pagesWorld Day For Safety and Health at Work 2020 - Stop The PandemicZulkarnaenUchihaNo ratings yet
- Guidelines On Safety at Workplace - Covid-19 Final Draft - RDocument8 pagesGuidelines On Safety at Workplace - Covid-19 Final Draft - RGanga Bdr BishwakarmaNo ratings yet
- In The Face of A Pandemic:: Ensuring Safety and Health at WorkDocument52 pagesIn The Face of A Pandemic:: Ensuring Safety and Health at WorkEfren SangcoNo ratings yet
- COVID Module 1 TranscriptDocument3 pagesCOVID Module 1 TranscriptgerajassoNo ratings yet
- Corona Pandemic: by Ria Grover Class XB Roll No.36Document6 pagesCorona Pandemic: by Ria Grover Class XB Roll No.36RIA 92462No ratings yet
- Effects of Covid on Hospital DesignDocument4 pagesEffects of Covid on Hospital DesignChristian LantingNo ratings yet
- WHO 2019 nCoV Clinical 2020.5 EngDocument62 pagesWHO 2019 nCoV Clinical 2020.5 EngTemis Edwin Guzman MartinezNo ratings yet
- UV Lights Effect on COVIDDocument6 pagesUV Lights Effect on COVIDAngelyn MarquezNo ratings yet
- BWI Covid Guidance Eng WebDocument11 pagesBWI Covid Guidance Eng WebKalyana RLNo ratings yet
- Novel Corona Virus Infection GuidelinesDocument28 pagesNovel Corona Virus Infection GuidelinesZharlene PadillaNo ratings yet
- Guidance For Preventing and Controlling COVID-19 Outbreaks in New Zealand Aged Residential CareDocument29 pagesGuidance For Preventing and Controlling COVID-19 Outbreaks in New Zealand Aged Residential CareAleksandr ShnyrovNo ratings yet
- WHO 2019 nCoV HCW - Risk - Factors - Protocol 2020.3 EngDocument48 pagesWHO 2019 nCoV HCW - Risk - Factors - Protocol 2020.3 EngNeova XNo ratings yet
- Guidelines For Post School Education and Training PSET Institutions For Management of and Response To The COVID 19 OutbreakDocument36 pagesGuidelines For Post School Education and Training PSET Institutions For Management of and Response To The COVID 19 OutbreakMichael NcubeNo ratings yet
- HIV Interim Guidance - 2nd Edition - Final May-2020Document23 pagesHIV Interim Guidance - 2nd Edition - Final May-2020JamalNo ratings yet
- Introduction to COVIDDocument7 pagesIntroduction to COVIDqaseem2109No ratings yet
- Novel Coronavirus 2019 (2019-Ncov) Infection: Part Ii - Respiratory Support in The Pediatric Intensive Care Unit in Resource-Limited SettingsDocument9 pagesNovel Coronavirus 2019 (2019-Ncov) Infection: Part Ii - Respiratory Support in The Pediatric Intensive Care Unit in Resource-Limited SettingsHanni HarahapNo ratings yet
- Coronavirus Disease 2019 (COVID-19) GuidelinesDocument13 pagesCoronavirus Disease 2019 (COVID-19) Guidelinesrajesh BNo ratings yet
- COVID-19 Infection in Pregnancy: Healthcare Professional GuidanceDocument61 pagesCOVID-19 Infection in Pregnancy: Healthcare Professional GuidanceIndah AulliaNo ratings yet
- PSMID Covid Guidelines March 31, 20208080312298125101472Document62 pagesPSMID Covid Guidelines March 31, 20208080312298125101472Rina Fajardo - NacinNo ratings yet
- China's Novel Coronavirus Response: Guidelines for Governments, Communities, Entities and Individuals to Combat COVID-19From EverandChina's Novel Coronavirus Response: Guidelines for Governments, Communities, Entities and Individuals to Combat COVID-19No ratings yet
- Welcome Student!: InstructionsDocument27 pagesWelcome Student!: InstructionsumaNo ratings yet
- Article in Press: Florence Nightingale's Environmental Theory and Its in Uence On Contemporary Infection ControlDocument8 pagesArticle in Press: Florence Nightingale's Environmental Theory and Its in Uence On Contemporary Infection ControlBalqist Asyawa Andra PutriNo ratings yet
- NLOA Prelims RationalizationDocument7 pagesNLOA Prelims RationalizationVincent JadolNo ratings yet
- Micp Lec (Week 5) Bacteria and DiseaseDocument11 pagesMicp Lec (Week 5) Bacteria and Diseasecaitie miracleNo ratings yet
- Internal Policies And/Or Procedure (Ipp)Document2 pagesInternal Policies And/Or Procedure (Ipp)LENARD GRIJALDONo ratings yet
- Tle 8 Beautycare Q4 M6Document7 pagesTle 8 Beautycare Q4 M6Alessandra MelanioNo ratings yet
- Ghop 2013Document65 pagesGhop 2013petal80No ratings yet
- D Pharm Lecture Notes by Pro. LangdonDocument10 pagesD Pharm Lecture Notes by Pro. LangdonSwathi KNo ratings yet
- PRS Ear Instillation - GlovaDocument3 pagesPRS Ear Instillation - GlovaAndrea Colleen GlovaNo ratings yet
- Dr. Unum Aslams Impressive Public Health CareerDocument5 pagesDr. Unum Aslams Impressive Public Health Careermango chaunsaNo ratings yet
- De Carvalho Nagliate Et Al - 2013 - Measures of Knowledge About Standard PrecautionsDocument6 pagesDe Carvalho Nagliate Et Al - 2013 - Measures of Knowledge About Standard PrecautionsBlake Toscani Apaza PerezNo ratings yet
- NurseCorps Part 6Document38 pagesNurseCorps Part 6smith.kevin1420344No ratings yet
- Ideal CHC Manual - Version 1 - Updated May 2021Document468 pagesIdeal CHC Manual - Version 1 - Updated May 2021Upasna KulasteNo ratings yet
- Environmental Infection ControlDocument52 pagesEnvironmental Infection ControlRAHULNo ratings yet
- Peran Ipp SurveierDocument20 pagesPeran Ipp Surveiersahrun runtiNo ratings yet
- IPAC CHECKLIST FOR CLINICAL OFFICE PRACTICEDocument19 pagesIPAC CHECKLIST FOR CLINICAL OFFICE PRACTICEBABBY ZBOURGNo ratings yet
- HLTINF003 Assessment 2 Infection Control Portfolio V2 2019-3Document6 pagesHLTINF003 Assessment 2 Infection Control Portfolio V2 2019-3MixNo ratings yet
- Safety Seal Certification Checklist: (DILG As Issuing Officer)Document3 pagesSafety Seal Certification Checklist: (DILG As Issuing Officer)bash bashNo ratings yet
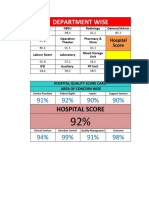
- Hospital quality score card by department and area of concernDocument165 pagesHospital quality score card by department and area of concernsaravananNo ratings yet
- Octave - InserviceDocument3 pagesOctave - Inserviceapi-317388058No ratings yet
- 2022 WHO Framework and Toolkit For IPC in Outbreak PreparednessDocument71 pages2022 WHO Framework and Toolkit For IPC in Outbreak PreparednessCatherina MulyantoNo ratings yet
- Harmonized TTMF Assessment-Tool Final Draft Jul 27 2020Document10 pagesHarmonized TTMF Assessment-Tool Final Draft Jul 27 2020Jay EspinalNo ratings yet
- PPT.2021.IPC Best Practices - Doh Report.Document38 pagesPPT.2021.IPC Best Practices - Doh Report.Lucky OlvisNo ratings yet
- BCG Nursing ProcedureDocument2 pagesBCG Nursing ProcedureBSN 1A- Serrano Evytte Joy B.No ratings yet