You might also like
- Classification of DiureticDocument3 pagesClassification of DiureticJanice Malafu De GuiaNo ratings yet
- Renal 2 MTC PDFDocument55 pagesRenal 2 MTC PDFDrbee10No ratings yet
- Solvent Dyeing PDFDocument23 pagesSolvent Dyeing PDFDhrubo Adhikary100% (1)
- Urine Formation: Yousaf Khan Renal Dialysis LecturerDocument30 pagesUrine Formation: Yousaf Khan Renal Dialysis LecturerSalman KhanNo ratings yet
- Osmotic Regulation and ExcretionDocument46 pagesOsmotic Regulation and ExcretionKhent SyNo ratings yet
- Chapter 24. The Kidney.: 1. The Structure and Function of The NephronDocument8 pagesChapter 24. The Kidney.: 1. The Structure and Function of The NephronjeskevandiemenNo ratings yet
- REN Revision LectureDocument43 pagesREN Revision Lecturegyamfi.rolandNo ratings yet
- 10.excretory SystemDocument16 pages10.excretory SystemLeena HassaninNo ratings yet
- L8-Urine Conc.Document15 pagesL8-Urine Conc.Bryn MasvaureNo ratings yet
- LOOP OF HENLE (Modified)Document25 pagesLOOP OF HENLE (Modified)Chuleha SethNo ratings yet
- Physiology 2nd Semestercm - Cs S.F.ADocument52 pagesPhysiology 2nd Semestercm - Cs S.F.AVeronica Nica MaisteriucNo ratings yet
- 5 RenalDocument10 pages5 RenalAli EllaffiNo ratings yet
- SHS.108.Lect-10 Tubular ReabsorptionDocument61 pagesSHS.108.Lect-10 Tubular ReabsorptionAzlan YasirNo ratings yet
- Process in Urine Formation: Chapter: 9 HomeostasisDocument14 pagesProcess in Urine Formation: Chapter: 9 HomeostasisC.W.DalilaNo ratings yet
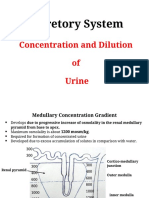
- Concentration and Dilution of UrineDocument26 pagesConcentration and Dilution of UrineHakimah K. SuhaimiNo ratings yet
- L5&6-Tubular Reabsorption& SecretionDocument38 pagesL5&6-Tubular Reabsorption& SecretionsairahhannahNo ratings yet
- IM II - Fluids and Electrolytes (Lecture Trans)Document18 pagesIM II - Fluids and Electrolytes (Lecture Trans)Robert Francis DikioNo ratings yet
- Diuretics TableDocument6 pagesDiuretics TableVie TNo ratings yet
- Applied Renal PhysiologyDocument18 pagesApplied Renal PhysiologyDamián ContrerasNo ratings yet
- Brooks - Renal - Boards Step 1 ReviewDocument43 pagesBrooks - Renal - Boards Step 1 ReviewNyatarNo ratings yet
- Excretory Products and Their Elimination - Shobhit NirwanDocument15 pagesExcretory Products and Their Elimination - Shobhit NirwanArpita VermaNo ratings yet
- AUBFDocument8 pagesAUBFIssha CasañasNo ratings yet
- L4 Regional Transport 2023Document4 pagesL4 Regional Transport 2023bgj9cddvxhNo ratings yet
- RenalDocument134 pagesRenalMaleehaNo ratings yet
- Diuretics 2020Document79 pagesDiuretics 2020Amirhossein SheikhiNo ratings yet
- Lecture 21Document23 pagesLecture 21sara shloulNo ratings yet
- Urine Formation - Human Excretory SystemDocument13 pagesUrine Formation - Human Excretory SystemRaj KumarNo ratings yet
- Fluids and Electrolytes IV FluidsDocument1 pageFluids and Electrolytes IV Fluidsnursing concept mapsNo ratings yet
- Excretory Products and Its EliminationDocument2 pagesExcretory Products and Its Eliminationmariamfernandes6No ratings yet
- Excretory Products and Their EliminationDocument51 pagesExcretory Products and Their Eliminationmadam photonNo ratings yet
- Fisiologi 1 - Introducton Renal PhysiolgyDocument5 pagesFisiologi 1 - Introducton Renal PhysiolgyHachi Nini Shop IINo ratings yet
- Handling of Certain Important Solutes by The Renal TubulesDocument14 pagesHandling of Certain Important Solutes by The Renal TubulesOsama MohamedNo ratings yet
- Excretory Products and Their EliminationDocument9 pagesExcretory Products and Their Eliminationadityaaggarwal821No ratings yet
- Renal FunctionDocument2 pagesRenal FunctionlenoNo ratings yet
- 9-ch 26 - Urinary System CDocument95 pages9-ch 26 - Urinary System Clouise navorNo ratings yet
- Seeley GENITODocument20 pagesSeeley GENITOAce Khiel Peralta100% (1)
- Lo Week 1-1Document11 pagesLo Week 1-1Martien Silviandy SetiawanNo ratings yet
- Fundamental of Urinary System (2020)Document55 pagesFundamental of Urinary System (2020)Nadya PutriNo ratings yet
- CB CH 04 KidneyDocument26 pagesCB CH 04 KidneyDeemaNo ratings yet
- SODIUMDocument4 pagesSODIUMNorhidayah NoordinNo ratings yet
- CH ExcretionDocument9 pagesCH ExcretionlatasabarikNo ratings yet
- DCT and Collecting DuctDocument29 pagesDCT and Collecting DuctayeshaNo ratings yet
- Topic 2 Aubf Renal Function PDFDocument5 pagesTopic 2 Aubf Renal Function PDFBanana QNo ratings yet
- Kidney & NephronDocument3 pagesKidney & NephronrodtanchoNo ratings yet
- Anatomi Dan Fisiologi GinjalDocument33 pagesAnatomi Dan Fisiologi GinjalRizha Zhetira100% (1)
- Activity 36 - Urinary Tubular Reabsorption and SecretionDocument6 pagesActivity 36 - Urinary Tubular Reabsorption and SecretionKaren Joy MagbanuaNo ratings yet
- ANAT 1053 Unit 6 Urinary System Prof Slides Fall 2021Document58 pagesANAT 1053 Unit 6 Urinary System Prof Slides Fall 2021abextekNo ratings yet
- Tubular Reabsorption and SecretionDocument21 pagesTubular Reabsorption and SecretionAhmad KhanNo ratings yet
- LECTURE 2 Urinary System - Histology HB II 2023Document79 pagesLECTURE 2 Urinary System - Histology HB II 2023Emmanuel AssopiahNo ratings yet
- Tubular ReabsorptionDocument42 pagesTubular Reabsorptionmina mounirNo ratings yet
- FS1 R KR7 OMu 7 VZFPL B13 XDocument4 pagesFS1 R KR7 OMu 7 VZFPL B13 Xaadeshthite476No ratings yet
- Excretion IDocument27 pagesExcretion Ierinjoy77No ratings yet
- Renal System 6 1Document30 pagesRenal System 6 1gaurav singhNo ratings yet
- Countercurrent Multiplier and ADHDocument5 pagesCountercurrent Multiplier and ADHAurora TamNo ratings yet
- Biology 102 (4-12-07)Document43 pagesBiology 102 (4-12-07)api-19786313100% (1)
- Renal Physiology Review-SDocument57 pagesRenal Physiology Review-SWilton RemigioNo ratings yet
- Kidney Function - ExcretionDocument15 pagesKidney Function - Excretionznayune82No ratings yet
- 1 Renal FunctionDocument5 pages1 Renal FunctionChristopher BucuNo ratings yet
- KidneyoutlineDocument33 pagesKidneyoutlineapi-273417637No ratings yet
- Acute Tubular Renal AcidosisDocument10 pagesAcute Tubular Renal AcidosisBarda GulanNo ratings yet
- Hydration and Intermolecular Interaction: Infrared Investigations with Polyelectrolyte MembranesFrom EverandHydration and Intermolecular Interaction: Infrared Investigations with Polyelectrolyte MembranesNo ratings yet
- Research Governance HandbookDocument41 pagesResearch Governance HandbookIbrahim QariNo ratings yet
- Research As A Transferable Skill Course OverviewDocument4 pagesResearch As A Transferable Skill Course OverviewIbrahim QariNo ratings yet
- jcm00141 0073Document6 pagesjcm00141 0073Ibrahim QariNo ratings yet
- Basic Swahili Course For TouristsDocument12 pagesBasic Swahili Course For TouristsIbrahim QariNo ratings yet
- Susy CourseDocument359 pagesSusy CourseIbrahim QariNo ratings yet
- Russia Political MapDocument1 pageRussia Political MapIbrahim QariNo ratings yet
- Transferable Skills Information PackDocument20 pagesTransferable Skills Information PackIbrahim QariNo ratings yet
- Specification Accredited A Level Gce History A h505Document132 pagesSpecification Accredited A Level Gce History A h505Ibrahim QariNo ratings yet
- References:: 1-Essen4al of Molecular Biology by George M. Malacinski 4 Edi4on 2Document19 pagesReferences:: 1-Essen4al of Molecular Biology by George M. Malacinski 4 Edi4on 2Ibrahim QariNo ratings yet
- Kotobati - كتاب حكم وأمثال شعبية للكاتبة رانيا بوراس.Document87 pagesKotobati - كتاب حكم وأمثال شعبية للكاتبة رانيا بوراس.Ibrahim QariNo ratings yet
- Laos PDFDocument1 pageLaos PDFIbrahim QariNo ratings yet
- Map of ItalyDocument1 pageMap of ItalyIbrahim QariNo ratings yet
- Introduction To Carpentry Tools and JointsDocument8 pagesIntroduction To Carpentry Tools and JointsIbrahim QariNo ratings yet
- Module 4 Considerations and Capacities of Contact LawsDocument4 pagesModule 4 Considerations and Capacities of Contact LawsIbrahim QariNo ratings yet
- Module 2 Ministry of JusticeDocument3 pagesModule 2 Ministry of JusticeIbrahim QariNo ratings yet
- Poland MapDocument1 pagePoland MapIbrahim QariNo ratings yet
- Chapter One: The Role of Marketing Research in Management Decision MakingDocument17 pagesChapter One: The Role of Marketing Research in Management Decision MakingIbrahim QariNo ratings yet
- Emojevwe V Respiratory Physiologyoer1595509Document133 pagesEmojevwe V Respiratory Physiologyoer1595509Ibrahim QariNo ratings yet
- ConjunctivitisDocument1 pageConjunctivitisIbrahim QariNo ratings yet
- Defining Cuisine and Types of Cuisine: Jordan Kocevski, PHD Michael Risteski, PHDDocument12 pagesDefining Cuisine and Types of Cuisine: Jordan Kocevski, PHD Michael Risteski, PHDIbrahim QariNo ratings yet
- Infective ConjunctivitisDocument2 pagesInfective ConjunctivitisIbrahim QariNo ratings yet
- APznzaZjEw5YQRByekcj2P79uwLOg8h--2J_rjMfs_LJYwNtCqpMToKzsAUaeIIcxDgEJS_UeGGsGWhJBs0ek6wChxnVlWvrLFdMxDkgMs...-YWRjq37tAIJmhMiFlLLYpMXYM0iM9pUzxdZK2Zt_Mk4Irf-jH6S85QiKsJKafYuuKN81x9_8AVsu0le2w5FL63Zv_fo-rhvt9tvLUwmFiB3kIVbAHMVZP0g==Document39 pagesAPznzaZjEw5YQRByekcj2P79uwLOg8h--2J_rjMfs_LJYwNtCqpMToKzsAUaeIIcxDgEJS_UeGGsGWhJBs0ek6wChxnVlWvrLFdMxDkgMs...-YWRjq37tAIJmhMiFlLLYpMXYM0iM9pUzxdZK2Zt_Mk4Irf-jH6S85QiKsJKafYuuKN81x9_8AVsu0le2w5FL63Zv_fo-rhvt9tvLUwmFiB3kIVbAHMVZP0g==Ibrahim QariNo ratings yet
- Accounting & Finance (Session-6)Document102 pagesAccounting & Finance (Session-6)Ibrahim QariNo ratings yet
- Accounting & Finance (Session-5)Document52 pagesAccounting & Finance (Session-5)Ibrahim QariNo ratings yet
- Marketing Your ProductDocument101 pagesMarketing Your ProductIbrahim QariNo ratings yet
- Introduction To MarketingDocument17 pagesIntroduction To MarketingIbrahim QariNo ratings yet
- Accounting & Finance (Session-3)Document41 pagesAccounting & Finance (Session-3)Ibrahim QariNo ratings yet
- The Marketing "Mix"Document5 pagesThe Marketing "Mix"Ibrahim QariNo ratings yet
- Accounting & Finance (Session-2)Document33 pagesAccounting & Finance (Session-2)Ibrahim QariNo ratings yet
- Accounting & Finance (Session-8)Document37 pagesAccounting & Finance (Session-8)Ibrahim QariNo ratings yet
- Lecture For Production Well PlanningDocument63 pagesLecture For Production Well PlanningmanashNo ratings yet
- Air PollutionDocument11 pagesAir PollutionrangaNo ratings yet
- 3 - Unit 2 Topic 6 Notes EnergeticsDocument12 pages3 - Unit 2 Topic 6 Notes EnergeticsjjkNo ratings yet
- (GENCHEM) Chemical BondingDocument49 pages(GENCHEM) Chemical BondingTrish GerongNo ratings yet
- WS 2 (15.07.22)Document3 pagesWS 2 (15.07.22)Micheelle JeannethNo ratings yet
- Lab ManualDocument23 pagesLab ManualAndi AbelloNo ratings yet
- 3.AcidBases FinalDocument35 pages3.AcidBases FinalSoham RaneNo ratings yet
- I Science I: JKBOSE Class 10 Science Sample PaperDocument24 pagesI Science I: JKBOSE Class 10 Science Sample PaperEem WritesNo ratings yet
- Lewis Acid-Activated Reactions of Silyl Ketenes For The PreparationDocument8 pagesLewis Acid-Activated Reactions of Silyl Ketenes For The PreparationJonathan MendozaNo ratings yet
- Remote Monitoring and Intelligent Controls of Cathodc Protection System of Gas Transmissino PipelinesDocument96 pagesRemote Monitoring and Intelligent Controls of Cathodc Protection System of Gas Transmissino PipelinesToro JulioNo ratings yet
- EMB - Carboxypeptidase YDocument2 pagesEMB - Carboxypeptidase YJim Well MartinNo ratings yet
- C 311 - 00 Qzmxms0wmaDocument9 pagesC 311 - 00 Qzmxms0wmaTemur LomidzeNo ratings yet
- Advertise in Our Magazine (Click Here) - Subscribe Whatsapp Version of Our Magazine: (Click Here) )Document72 pagesAdvertise in Our Magazine (Click Here) - Subscribe Whatsapp Version of Our Magazine: (Click Here) )Patodia ChemicalsNo ratings yet
- Biogeochemical CyclesDocument18 pagesBiogeochemical CyclesSherina Leona AgellonNo ratings yet
- WOW Notes! DLP Chemistry, Carbon CompoundDocument32 pagesWOW Notes! DLP Chemistry, Carbon Compoundnur asyiqinNo ratings yet
- Isomerism KEC 077 Lecture IV BCE A 079-02-17 PST.Document26 pagesIsomerism KEC 077 Lecture IV BCE A 079-02-17 PST.bsarad115No ratings yet
- Allotropes of Sulfur: From Wikipedia, The Free EncyclopediaDocument10 pagesAllotropes of Sulfur: From Wikipedia, The Free EncyclopediaAshish GoelNo ratings yet
- Autochem2920 Brochure 2017 - 2Document5 pagesAutochem2920 Brochure 2017 - 2bau.bau.bau.bauuNo ratings yet
- Physical ScienceDocument117 pagesPhysical Sciencechi582552No ratings yet
- Inorganic Chemistry 1 - Alkali Metals RevisioDocument7 pagesInorganic Chemistry 1 - Alkali Metals RevisioAshleyn Mary SandersNo ratings yet
- 2022 Chem Bond Tut Qns and SolnsDocument16 pages2022 Chem Bond Tut Qns and SolnsBooNo ratings yet
- CSEC Chemistry June 2017 P2Document18 pagesCSEC Chemistry June 2017 P2Shan CampNo ratings yet
- MSDS of Asi-CalphosDocument4 pagesMSDS of Asi-Calphosthiensuty74No ratings yet
- BMS531 BMS537 Lab Manual 2022Document33 pagesBMS531 BMS537 Lab Manual 2022Siti Khadijah Binti Abu SaamahNo ratings yet
- Calcite - WikipediaDocument7 pagesCalcite - Wikipediaivana yustyariniNo ratings yet
- MIC 304-322 Metabolism 2021 - 22 Noteset 3Document16 pagesMIC 304-322 Metabolism 2021 - 22 Noteset 3kilanko timilehinNo ratings yet
- Tom's Thesis SubmittedDocument155 pagesTom's Thesis Submittedapi-19973956No ratings yet
- Chapter - 1 - Atoms Molecules StoichiometryDocument25 pagesChapter - 1 - Atoms Molecules StoichiometrylidiaepNo ratings yet
- 2020 Exam: Sample QuestionsDocument7 pages2020 Exam: Sample Questions소피아No ratings yet