You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- UP Law BOC 2022 Criminal LawDocument335 pagesUP Law BOC 2022 Criminal LawRoberto Galano Jr.100% (9)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- UP Law BOC 2022 Commercial LawDocument305 pagesUP Law BOC 2022 Commercial LawRoberto Galano Jr.100% (3)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- AGNOR - Proposed PSIPOP Creation - IS and Annexes Sec SchoolsDocument2 pagesAGNOR - Proposed PSIPOP Creation - IS and Annexes Sec SchoolsRoberto Galano Jr.No ratings yet
- Investigation RJK 782Document1 pageInvestigation RJK 782Roberto Galano Jr.No ratings yet
- 2023 Purple Notes in Labor LawDocument249 pages2023 Purple Notes in Labor LawRoberto Galano Jr.100% (5)
- NBissanletter 4 LTODocument2 pagesNBissanletter 4 LTORoberto Galano Jr.No ratings yet
- Adn List of Examinees From Online Jke 07 2023Document5 pagesAdn List of Examinees From Online Jke 07 2023Roberto Galano Jr.No ratings yet
- Court Clearance Endosred ToDocument2 pagesCourt Clearance Endosred ToRoberto Galano Jr.No ratings yet
- Tambok C Marh - JorieDocument4 pagesTambok C Marh - JorieRoberto Galano Jr.No ratings yet
- T.A NLCDocument1 pageT.A NLCRoberto Galano Jr.No ratings yet
- Referral of Cases To Legal ResearcherDocument5 pagesReferral of Cases To Legal ResearcherRoberto Galano Jr.No ratings yet
- Based On The Documents Submitted TalingtingDocument2 pagesBased On The Documents Submitted TalingtingRoberto Galano Jr.No ratings yet
- Hon LetterDocument1 pageHon LetterRoberto Galano Jr.No ratings yet
- Notice of Hearing WestDocument2 pagesNotice of Hearing WestRoberto Galano Jr.No ratings yet
- SampleDocument3 pagesSampleRoberto Galano Jr.No ratings yet
- Updates On The Forestry Related Cases Filed in Cort National Prosecution Office DOJ of CNCTDocument1 pageUpdates On The Forestry Related Cases Filed in Cort National Prosecution Office DOJ of CNCTRoberto Galano Jr.No ratings yet
- Fire Incident Investigation ReportDocument7 pagesFire Incident Investigation ReportRoberto Galano Jr.100% (1)
- Commercial Law 2021Document385 pagesCommercial Law 2021Roberto Galano Jr.0% (1)
- GP Lolong Minutes of The HearingDocument5 pagesGP Lolong Minutes of The HearingRoberto Galano Jr.No ratings yet
- Hearing Officer Statement For The Administering of An OathDocument2 pagesHearing Officer Statement For The Administering of An OathRoberto Galano Jr.No ratings yet
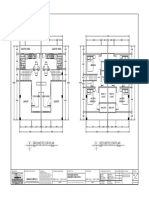
- Floor PlanDocument1 pageFloor PlanRoberto Galano Jr.No ratings yet
- Bayog LumberDocument2 pagesBayog LumberRoberto Galano Jr.No ratings yet
- Alubijid ReportDocument3 pagesAlubijid ReportRoberto Galano Jr.No ratings yet
- Bnhs Apr EditedDocument2 pagesBnhs Apr EditedRoberto Galano Jr.No ratings yet
- 366pcs. AWA 3260Document5 pages366pcs. AWA 3260Roberto Galano Jr.No ratings yet
- 1st Memo NasipitDocument1 page1st Memo NasipitRoberto Galano Jr.No ratings yet
- Letter For Ocular InspectionDocument2 pagesLetter For Ocular InspectionRoberto Galano Jr.100% (2)
- Department of Environment and Natural Resources Provincial Environment and Natural Resources Tiniwisan, Butuan City Individual Work From Home PlanDocument1 pageDepartment of Environment and Natural Resources Provincial Environment and Natural Resources Tiniwisan, Butuan City Individual Work From Home PlanRoberto Galano Jr.No ratings yet
- Summons: Petition, Copy of Which Is Attached, Together With The Annexes. If You Fail To AnswerDocument1 pageSummons: Petition, Copy of Which Is Attached, Together With The Annexes. If You Fail To AnswerRoberto Galano Jr.No ratings yet