You might also like
- Method Statement and Risk Assessment-1Document54 pagesMethod Statement and Risk Assessment-1Emmanuel kusimo100% (1)
- GLOC Health Claim Form Fillable Form NewDocument2 pagesGLOC Health Claim Form Fillable Form NewRyanRamroopNo ratings yet
- Providence WC Clinic Referral FormDocument3 pagesProvidence WC Clinic Referral FormlisamaurerNo ratings yet
- 3 Accident Investigation FormDocument5 pages3 Accident Investigation Formsusa1716100% (1)
- NHCA Health Club Incident RPT FormDocument2 pagesNHCA Health Club Incident RPT Formcrossfitvelocity982No ratings yet
- Employees Accedent ReportDocument1 pageEmployees Accedent ReportKomal TiwariNo ratings yet
- Employee Report of Injury (NEW)Document1 pageEmployee Report of Injury (NEW)Kerry CollinsNo ratings yet
- Sample Accident ReportDocument5 pagesSample Accident ReportadmzaemNo ratings yet
- Health Surveillance QuestionaireDocument5 pagesHealth Surveillance QuestionaireTrinidad InspectionNo ratings yet
- Accident Investigation Form PDFDocument5 pagesAccident Investigation Form PDFAfiq BahaNo ratings yet
- Accident & Incident Investigation FormDocument5 pagesAccident & Incident Investigation FormTony CampbellNo ratings yet
- FILL and UPLOAD Week 4 - Accident Investigation FormDocument5 pagesFILL and UPLOAD Week 4 - Accident Investigation FormAnonymous HizOWFNo ratings yet
- Indah Nur Jayanti - 21070121120009 - Investigasi KecelakaanDocument6 pagesIndah Nur Jayanti - 21070121120009 - Investigasi KecelakaanIndah Nur JNo ratings yet
- Vba 21 0960m 13 Are CervicalDocument11 pagesVba 21 0960m 13 Are CervicalCombat CraigNo ratings yet
- 2023 - Registration FormDocument3 pages2023 - Registration FormhusnanabiyyuNo ratings yet
- Injury Illness ReportDocument2 pagesInjury Illness ReportRay StatamNo ratings yet
- VBA 21 0960M 9 ARE Knee and Lower LegDocument10 pagesVBA 21 0960M 9 ARE Knee and Lower LegCombat CraigNo ratings yet
- 1 - BSBWHS521 Appendix E - Register of Injuries TemplateDocument3 pages1 - BSBWHS521 Appendix E - Register of Injuries TemplateKamal SainiNo ratings yet
- Client Intake Form: Date Patient Last: First Initial Address City Zip Date of Birth Phone CellDocument6 pagesClient Intake Form: Date Patient Last: First Initial Address City Zip Date of Birth Phone Celljayson_tamayo2No ratings yet
- Accidents Before & AfterDocument1 pageAccidents Before & AftergolusinghdataNo ratings yet
- SAFETY Accident - Investigation - Form (1) (AutoRecovered)Document6 pagesSAFETY Accident - Investigation - Form (1) (AutoRecovered)ramilnavarra62No ratings yet
- WIC Claim FormDocument3 pagesWIC Claim FormHihiNo ratings yet
- USGICL - Accidental Insurance - Common Claim FormDocument4 pagesUSGICL - Accidental Insurance - Common Claim FormKôtî MśdiañNo ratings yet
- Supervisor's Accident Investigation FormDocument4 pagesSupervisor's Accident Investigation FormJoy DePazNo ratings yet
- Sample Medical Incident Report: Section 1Document2 pagesSample Medical Incident Report: Section 1DS SystemsNo ratings yet
- Incident Accident Investigation Report - EriadiDocument2 pagesIncident Accident Investigation Report - EriadiPeter Sare WolloNo ratings yet
- EAW.07 Ass.2 v1.0Document5 pagesEAW.07 Ass.2 v1.0Madhu BhaiNo ratings yet
- Pre AdmissionDocument5 pagesPre AdmissionLaura Margaretha BatlayarNo ratings yet
- Wrist Conditions Disability Benefits QuestionnaireDocument8 pagesWrist Conditions Disability Benefits QuestionnaireCombat CraigNo ratings yet
- Employee's Report of Injury FormDocument4 pagesEmployee's Report of Injury FormAlifudin HanifNo ratings yet
- SafetyAccidentInvestigationQuestionsandNeededInfo tcm36-208795 PDFDocument2 pagesSafetyAccidentInvestigationQuestionsandNeededInfo tcm36-208795 PDFramkumardotg_5807772No ratings yet
- SafetyAccidentInvestigationQuestionsandNeededInfo tcm36-208795 PDFDocument2 pagesSafetyAccidentInvestigationQuestionsandNeededInfo tcm36-208795 PDFramkumardotg_5807772No ratings yet
- Accident-incident-Early Report FormDocument1 pageAccident-incident-Early Report FormAngeloNo ratings yet
- Medical Certificate 2Document2 pagesMedical Certificate 2Aditeya Shukla100% (1)
- Statement of Medical Examiner - Total Permanent Disability Section BDocument4 pagesStatement of Medical Examiner - Total Permanent Disability Section Brajecon543No ratings yet
- Ofa Statment Fitness PDF enDocument2 pagesOfa Statment Fitness PDF ensatheeskumar VikramasingarajNo ratings yet
- SAFE520bP - Injury ReportDocument1 pageSAFE520bP - Injury ReportMiracle DavidNo ratings yet
- Winthrox Laboratories (PVT) Ltd. Ehs DepartmentDocument4 pagesWinthrox Laboratories (PVT) Ltd. Ehs Departmentanoushia alviNo ratings yet
- English TranslatedDocument2 pagesEnglish TranslatedUMAR KHANNo ratings yet
- New Patient Questionnaire Physical Therapy: Chief ComplaintDocument4 pagesNew Patient Questionnaire Physical Therapy: Chief ComplaintAstonNo ratings yet
- Incident Report Form: RPSG-IMS-F-24 Accident and Investigation Form 5ADocument2 pagesIncident Report Form: RPSG-IMS-F-24 Accident and Investigation Form 5ARocky BisNo ratings yet
- Massage Intake and Agreement Form CoreDocument2 pagesMassage Intake and Agreement Form CoreCraig JohnsonNo ratings yet
- Incident Reporting Form PDFDocument2 pagesIncident Reporting Form PDFdeeptiNo ratings yet
- Pain Unit 5 PDFDocument1 pagePain Unit 5 PDFEka NursafitriNo ratings yet
- Family Ministry Incident ReportDocument2 pagesFamily Ministry Incident Report基督教門諾會光復教會No ratings yet
- MCPS Student Injury Report FormDocument2 pagesMCPS Student Injury Report FormConcussion_MCPS_MdNo ratings yet
- CT Consent FormDocument3 pagesCT Consent FormAnonymous WXqKjTXMNo ratings yet
- Attending Physicians Statement MCHBMMCDocument3 pagesAttending Physicians Statement MCHBMMCMohdShahrilAhmadNo ratings yet
- Consent For Eyebrow Drawing Using Microblading TechniqueDocument4 pagesConsent For Eyebrow Drawing Using Microblading TechniquekeziamachadoNo ratings yet
- Register of Injuries: Buoy CafeDocument3 pagesRegister of Injuries: Buoy CafeM. Hamza IftikharNo ratings yet
- VBA-21-0960C-11-ARE Seizure Disorders Epilepsy PDFDocument4 pagesVBA-21-0960C-11-ARE Seizure Disorders Epilepsy PDFCombat CraigNo ratings yet
- Incident Report Form: RPSG-IMS-F-24 Accident and Investigation Form 5ADocument2 pagesIncident Report Form: RPSG-IMS-F-24 Accident and Investigation Form 5ARocky BisNo ratings yet
- Incident Report Form: RPSG-IMS-F-24 Accident and Investigation Form 5ADocument2 pagesIncident Report Form: RPSG-IMS-F-24 Accident and Investigation Form 5ARocky Bis100% (1)
- VBA-21-0960C-8-ARE Headaches Migraines PDFDocument3 pagesVBA-21-0960C-8-ARE Headaches Migraines PDFCombat CraigNo ratings yet
- Lamp Sesi 8.2 Investigasi SCATDocument2 pagesLamp Sesi 8.2 Investigasi SCATaab kanayaNo ratings yet
- InjuriesDocument5 pagesInjuriesKc GarciaNo ratings yet
- ASK - Health Declaration FormDocument2 pagesASK - Health Declaration FormAkmal HaziqNo ratings yet
- Level Up! Body By Dre's 30-Day Bodyweight Program: Better Mind, Body and Nutrition! 20 Minutes or Less!From EverandLevel Up! Body By Dre's 30-Day Bodyweight Program: Better Mind, Body and Nutrition! 20 Minutes or Less!No ratings yet
- OHSE-CL-22 Welfare Facilities ChecklistDocument1 pageOHSE-CL-22 Welfare Facilities ChecklistEmmanuel kusimoNo ratings yet
- OHSE-CL-12 Machinery ChecklistDocument2 pagesOHSE-CL-12 Machinery ChecklistEmmanuel kusimoNo ratings yet
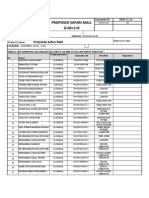
- Contracting M ET R OB U I L D IN G: Proposed Safari MallDocument2 pagesContracting M ET R OB U I L D IN G: Proposed Safari MallEmmanuel kusimoNo ratings yet
- OHSE-CL-18 Site General ChecklistDocument1 pageOHSE-CL-18 Site General ChecklistEmmanuel kusimoNo ratings yet
- Metro Building ContractingDocument4 pagesMetro Building ContractingEmmanuel kusimoNo ratings yet
- L 600 7577 Erecting Metal Chimneys in The WorkplaceDocument2 pagesL 600 7577 Erecting Metal Chimneys in The WorkplaceEmmanuel kusimoNo ratings yet
- New Bottom PlateDocument9 pagesNew Bottom PlateEmmanuel kusimo100% (1)
- 22toolbox Talk ReportDocument2 pages22toolbox Talk ReportEmmanuel kusimoNo ratings yet
- OHSE-CL-04 Environment ChecklistDocument1 pageOHSE-CL-04 Environment ChecklistEmmanuel kusimoNo ratings yet
- HSE-F-18 First Aid Box Checklist (AutoRecovered)Document1 pageHSE-F-18 First Aid Box Checklist (AutoRecovered)Emmanuel kusimoNo ratings yet
- Jtawab Toolbox Talk PaperDocument2 pagesJtawab Toolbox Talk PaperEmmanuel kusimoNo ratings yet
- SKM - C454e21022308000 1 1Document3 pagesSKM - C454e21022308000 1 1Emmanuel kusimoNo ratings yet
- OHSE-CL-09 Housekeeping ChecklistDocument1 pageOHSE-CL-09 Housekeeping ChecklistEmmanuel kusimoNo ratings yet
- Civil Toolbox Talk PaperDocument2 pagesCivil Toolbox Talk PaperEmmanuel kusimoNo ratings yet
- OHSE-CL-21 Welding and Gas Cutting ChecklistDocument3 pagesOHSE-CL-21 Welding and Gas Cutting ChecklistEmmanuel kusimoNo ratings yet
- ARIA TANKS - Mechanical VariationDocument1 pageARIA TANKS - Mechanical VariationEmmanuel kusimoNo ratings yet
- OHSE-CL-22 Welfare Facilities ChecklistDocument1 pageOHSE-CL-22 Welfare Facilities ChecklistEmmanuel kusimoNo ratings yet
- OHSE-CL-18 Site General ChecklistDocument1 pageOHSE-CL-18 Site General ChecklistEmmanuel kusimoNo ratings yet
- Method StatementDocument10 pagesMethod StatementEmmanuel kusimoNo ratings yet