You might also like
- Surviving and Thriving: How to Ensure Your First Year at Work Doesn't End in DisasterFrom EverandSurviving and Thriving: How to Ensure Your First Year at Work Doesn't End in DisasterNo ratings yet
- Surviving and Thriving: How to Ensure Your First Year at Work Doesn’t End in DisasterFrom EverandSurviving and Thriving: How to Ensure Your First Year at Work Doesn’t End in DisasterNo ratings yet
- Incident Report FormDocument2 pagesIncident Report FormAnku Kingsley Etornam100% (1)
- Free HR Incident Investigation FormDocument2 pagesFree HR Incident Investigation FormRichard R M ThodéNo ratings yet
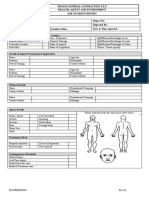
- Construction Accident Report FormDocument2 pagesConstruction Accident Report FormGirma AssefaNo ratings yet
- Lamp Sesi 8.2 Investigasi SCATDocument2 pagesLamp Sesi 8.2 Investigasi SCATaab kanayaNo ratings yet
- Incident Reporting Form PDFDocument2 pagesIncident Reporting Form PDFdeeptiNo ratings yet
- CDKNat OHS 015F 1 Register of Injuries FormDocument3 pagesCDKNat OHS 015F 1 Register of Injuries Formlol photoboothNo ratings yet
- 03 SHE SOP ACCIDENT INCIDENT REPORTING AND INVESTIGATION Rev02Document12 pages03 SHE SOP ACCIDENT INCIDENT REPORTING AND INVESTIGATION Rev02HADWAN YUSOFNo ratings yet
- Appendix 2 - Aldar Incident Investigation Report FormDocument7 pagesAppendix 2 - Aldar Incident Investigation Report FormXtreme-DesignsNo ratings yet
- April 04Document3 pagesApril 04roland magoNo ratings yet
- Incident Report FormDocument2 pagesIncident Report FormMuhammad Ibad AlamNo ratings yet
- Incident Reporting and Investigation 2Document3 pagesIncident Reporting and Investigation 2sreejukumar27No ratings yet
- Incident Report Muhammad SohailDocument4 pagesIncident Report Muhammad Sohailarfa vainceNo ratings yet
- Hse Department Accident/Incident Report Form /borang Laporan KemalanganDocument2 pagesHse Department Accident/Incident Report Form /borang Laporan Kemalanganlemuel bacsaNo ratings yet
- Accident Reporting, Investigation & Analysis (CIF&B)Document47 pagesAccident Reporting, Investigation & Analysis (CIF&B)saraswatvoNo ratings yet
- Wair ADocument2 pagesWair AJan Lenon Guira0% (1)
- Incident Report Form: RPSG-IMS-F-24 Accident and Investigation Form 5ADocument2 pagesIncident Report Form: RPSG-IMS-F-24 Accident and Investigation Form 5ARocky Bis100% (1)
- Workplace Injury/ Illness Report FormDocument2 pagesWorkplace Injury/ Illness Report FormDimpho MasetediNo ratings yet
- Near Miss and Accident FormDocument6 pagesNear Miss and Accident Formfaradayzzz100% (1)
- Incident Report Form: RPSG-IMS-F-24 Accident and Investigation Form 5ADocument2 pagesIncident Report Form: RPSG-IMS-F-24 Accident and Investigation Form 5ARocky BisNo ratings yet
- Employee Vehicle AccidentDocument2 pagesEmployee Vehicle AccidentlintangNo ratings yet
- Incident Report Form: RPSG-IMS-F-24 Accident and Investigation Form 5ADocument2 pagesIncident Report Form: RPSG-IMS-F-24 Accident and Investigation Form 5ARocky BisNo ratings yet
- SHES - Prelim Inci NotificationDocument3 pagesSHES - Prelim Inci NotificationKoi ChiNo ratings yet
- Injury Illness ReportDocument2 pagesInjury Illness ReportRay StatamNo ratings yet
- Department of Engineering Risk Assessment Form - This Is An Active Document and Must Be MaintainedDocument4 pagesDepartment of Engineering Risk Assessment Form - This Is An Active Document and Must Be MaintainedRadhaKrishnan RNo ratings yet
- Ed 155Document4 pagesEd 155api-299330082No ratings yet
- OHS Accident Investigation Report FormDocument2 pagesOHS Accident Investigation Report FormcoolariesatulNo ratings yet
- Employee Incident Report FormDocument2 pagesEmployee Incident Report FormDS SystemsNo ratings yet
- HSE-F-NEOM-008 - Final Incident-Accident ReportDocument4 pagesHSE-F-NEOM-008 - Final Incident-Accident ReportAhmed MohamedNo ratings yet
- Injury Incident Report FormDocument3 pagesInjury Incident Report FormDave Joseph Conde100% (1)
- Bobcat Fire Incident ReportDocument5 pagesBobcat Fire Incident ReportRana Muhammad NaeemNo ratings yet
- ISBN Register of Injuries Template Return To Work Toolkit 2011 07Document3 pagesISBN Register of Injuries Template Return To Work Toolkit 2011 07Rakesh KaushikNo ratings yet
- EHS-FORM-001 v.2.0 Accident and Incident Reporting FormDocument2 pagesEHS-FORM-001 v.2.0 Accident and Incident Reporting FormRaja Selvakumar100% (1)
- HSE Incident Report RevDocument2 pagesHSE Incident Report RevBee100% (1)
- Accident-Incident Investigation Form v1-3Document3 pagesAccident-Incident Investigation Form v1-3Jenevie DecenillaNo ratings yet
- DR. Ahdab Elmorshedy: Accident / Incident Initial Investigation ReportDocument4 pagesDR. Ahdab Elmorshedy: Accident / Incident Initial Investigation ReportKamal NabilNo ratings yet
- Near Miss Incident Accident Report and Investigation FormDocument3 pagesNear Miss Incident Accident Report and Investigation Formhutomo_90No ratings yet
- Dole BQF WairDocument5 pagesDole BQF Wairbeng acosta100% (1)
- Form Accident ReportDocument4 pagesForm Accident ReportKarthik SNo ratings yet
- Incident ReportDocument3 pagesIncident Reportyakeshk5No ratings yet
- Incident Report Muhammad Zahid Steel FixerDocument4 pagesIncident Report Muhammad Zahid Steel Fixerarfa vainceNo ratings yet
- EAW.07 Ass.2 v1.0Document5 pagesEAW.07 Ass.2 v1.0Madhu BhaiNo ratings yet
- Incident FormDocument5 pagesIncident FormMurtadda Mohammed100% (1)
- Register of InjuriesDocument3 pagesRegister of InjuriesMani VannanNo ratings yet
- HT12 CRDocument2 pagesHT12 CRgadcoNo ratings yet
- Incident & Accident ReportDocument7 pagesIncident & Accident ReportleganzaNo ratings yet
- Incident Report Muhammad IrfanDocument4 pagesIncident Report Muhammad Irfanarfa vainceNo ratings yet
- Incident Report Form: RPSG-IMS-F-24 Accident and Investigation Form 5ADocument2 pagesIncident Report Form: RPSG-IMS-F-24 Accident and Investigation Form 5ARocky Bis100% (1)
- Supervisor's Incident/Accident Analysis: Oregon Military DepartmentDocument5 pagesSupervisor's Incident/Accident Analysis: Oregon Military DepartmentAnonymous m39OcDL2XnNo ratings yet
- Accident Incident Report FormDocument3 pagesAccident Incident Report FormTuan NguyenNo ratings yet
- Certificate of FitnessDocument2 pagesCertificate of FitnessKarthik SNo ratings yet
- Incident Report FromDocument3 pagesIncident Report Fromannerie.krugerNo ratings yet
- Indah Nur Jayanti - 21070121120009 - Investigasi KecelakaanDocument6 pagesIndah Nur Jayanti - 21070121120009 - Investigasi KecelakaanIndah Nur JNo ratings yet
- Environmental Health Risk AssessmentDocument7 pagesEnvironmental Health Risk Assessmentdu dungNo ratings yet
- Incident Report FormDocument2 pagesIncident Report Formketegbe paterne ulrichNo ratings yet
- Injury Report-2022Document2 pagesInjury Report-2022vNo ratings yet
- AFC-HSE-F04 - Detailed Accident Investigation ReportDocument3 pagesAFC-HSE-F04 - Detailed Accident Investigation ReportIbrahim MohamedNo ratings yet
- Accident and Incident ReportDocument6 pagesAccident and Incident ReportCharles DoriaNo ratings yet
- SW - Ci - Const - Fillable CsirDocument10 pagesSW - Ci - Const - Fillable CsirJaycee Bareng PagadorNo ratings yet
- Paflbnrs Exo: of On Labeling and Rnrorrvra - UonDocument1 pagePaflbnrs Exo: of On Labeling and Rnrorrvra - Uonanoushia alviNo ratings yet
- MA 01.12 DRAFT Guideline On Non Rutine MADocument14 pagesMA 01.12 DRAFT Guideline On Non Rutine MAanoushia alviNo ratings yet
- Presentation FinalDocument27 pagesPresentation Finalanoushia alviNo ratings yet
- Water ConservationDocument18 pagesWater Conservationanoushia alviNo ratings yet
- USP 1664.1 LeachablesDocument6 pagesUSP 1664.1 Leachablesanoushia alviNo ratings yet
- Receiving of Raw & Pacheging Material SOPDocument6 pagesReceiving of Raw & Pacheging Material SOPanoushia alviNo ratings yet
- Raw Material Identification PerformaDocument2 pagesRaw Material Identification Performaanoushia alviNo ratings yet
- Qa Audit Points: Syrup Manufacturing AreaDocument11 pagesQa Audit Points: Syrup Manufacturing Areaanoushia alviNo ratings yet
- 13 SOP Cleaning For Dispensing AreaDocument3 pages13 SOP Cleaning For Dispensing Areaanoushia alviNo ratings yet
- Log Book of CleaningDocument2 pagesLog Book of Cleaninganoushia alviNo ratings yet
- Packaging Material Material Identification PerformaDocument2 pagesPackaging Material Material Identification Performaanoushia alviNo ratings yet
- Receiving of Packaging Material SOPDocument4 pagesReceiving of Packaging Material SOPanoushia alviNo ratings yet
- SOP of Handling of Packaging MaterialDocument3 pagesSOP of Handling of Packaging Materialanoushia alviNo ratings yet
- Factories Act 1934 CHAPTER IIIDocument1 pageFactories Act 1934 CHAPTER IIIanoushia alviNo ratings yet
- Requirments For EHS Spill KitsDocument1 pageRequirments For EHS Spill Kitsanoushia alviNo ratings yet
- SOP of IndentingDocument2 pagesSOP of Indentinganoushia alvi0% (1)
- Legal Register FormatDocument1 pageLegal Register Formatanoushia alviNo ratings yet
- Fire Extinguisher Inspection RecordDocument1 pageFire Extinguisher Inspection Recordanoushia alviNo ratings yet
- Emergency and Action Plans-FormatsDocument12 pagesEmergency and Action Plans-Formatsanoushia alviNo ratings yet
- Quality LEGAL AND OTHER REQUIREMENTS REGISTERDocument8 pagesQuality LEGAL AND OTHER REQUIREMENTS REGISTERanoushia alviNo ratings yet
- Register - EHS Legal RequirementsDocument4 pagesRegister - EHS Legal Requirementsanoushia alviNo ratings yet
- Winthrox Laboratories Pvt. LTDDocument2 pagesWinthrox Laboratories Pvt. LTDanoushia alviNo ratings yet
- EHS Manual - FinalDocument53 pagesEHS Manual - Finalanoushia alviNo ratings yet
- Covid-19 SopDocument3 pagesCovid-19 Sopanoushia alviNo ratings yet
- Policy: Title: Environment, Health & SafetyDocument1 pagePolicy: Title: Environment, Health & Safetyanoushia alviNo ratings yet
- Ehs Policy SopDocument3 pagesEhs Policy Sopanoushia alviNo ratings yet
- TOOL BOX MEETING AGENDA FormatDocument1 pageTOOL BOX MEETING AGENDA Formatanoushia alviNo ratings yet
- Tool Box Meeting SOP AISHADocument2 pagesTool Box Meeting SOP AISHAanoushia alviNo ratings yet
- Communication SOPDocument10 pagesCommunication SOPanoushia alvi100% (1)
- Conservation of WaterDocument2 pagesConservation of Wateranoushia alviNo ratings yet
- Jon Rappoport's Blog: Corona: Creating The Illusion of A Pandemic Through Diagnostic TestsDocument24 pagesJon Rappoport's Blog: Corona: Creating The Illusion of A Pandemic Through Diagnostic TestsDonnaveo ShermanNo ratings yet
- The First Principle: Let Likes Cure Likes: Medica (Drug Picture) Is The Most Similar To That of The Patient'sDocument2 pagesThe First Principle: Let Likes Cure Likes: Medica (Drug Picture) Is The Most Similar To That of The Patient'sKumar M V ScNo ratings yet
- Epidemology Pravctical Questions NR 1Document34 pagesEpidemology Pravctical Questions NR 1Adeeba AshrafNo ratings yet
- ANNEX E CONSENT FORM Edited 082922Document2 pagesANNEX E CONSENT FORM Edited 082922leslie buenNo ratings yet
- THE WORLD BANK OPERATIONAL MANUAL OD 4.30 Operational DirectiveDocument9 pagesTHE WORLD BANK OPERATIONAL MANUAL OD 4.30 Operational DirectiveIshara MadusankaNo ratings yet
- JOA-XII-October - December-2018-4f4ay9OBo6ShtirVV PDFDocument144 pagesJOA-XII-October - December-2018-4f4ay9OBo6ShtirVV PDFsillypoloNo ratings yet
- Civil Commitment CriteriaDocument17 pagesCivil Commitment CriteriaclydefindleyNo ratings yet
- Teaching Medicine and Medical Ethics Using PopularDocument180 pagesTeaching Medicine and Medical Ethics Using PopularRizky AmaliahNo ratings yet
- Arine Exp22 Word Ch04 Cumulative CattleDocument7 pagesArine Exp22 Word Ch04 Cumulative Cattlesramnarine1991No ratings yet
- Worksheet On Columbian Exchange - SmallpoxDocument3 pagesWorksheet On Columbian Exchange - SmallpoxfruittinglesNo ratings yet
- Lung Center v. Quezon CityDocument8 pagesLung Center v. Quezon CityMassabielleNo ratings yet
- A Brief History of The Origins of Behavioral MedicineDocument16 pagesA Brief History of The Origins of Behavioral MedicineAllie WatrenNo ratings yet
- Complete Guide To Urine TheraphyDocument9 pagesComplete Guide To Urine TheraphyNancy Miro100% (4)
- Negotiation With Difficult PeopleDocument20 pagesNegotiation With Difficult PeopleMikaela100% (1)
- Do Think Most People Realize How Common Mental Illness Is in The PopulationDocument3 pagesDo Think Most People Realize How Common Mental Illness Is in The PopulationHanna Marie TrocioNo ratings yet
- Ageing and Healthy Life Expectancy - JIAGDocument4 pagesAgeing and Healthy Life Expectancy - JIAGVince AugustineNo ratings yet
- Sources of Epidemiological Data BoazDocument4 pagesSources of Epidemiological Data Boazgeorgeloto1288% (8)
- Fish Hematology in AquacultureDocument28 pagesFish Hematology in AquacultureEdwin A. Aguilar M.100% (1)
- Full Name Nationality Status SEX Place of Birth Date of Birth Passport Number Languages Educational QualificationsDocument3 pagesFull Name Nationality Status SEX Place of Birth Date of Birth Passport Number Languages Educational QualificationsHoseinNo ratings yet
- Test Bank For Health Psychology 2 e 2nd Edition Deborah Fish RaginDocument36 pagesTest Bank For Health Psychology 2 e 2nd Edition Deborah Fish Raginrostratefootholdho0v100% (40)
- Benchmark Patient's Spiritual NeedsDocument6 pagesBenchmark Patient's Spiritual NeedsDamer WriterNo ratings yet
- Reseach On The Needs of Community Based Rehabilitation (CBR) For Disabled Persons in CambodiaDocument105 pagesReseach On The Needs of Community Based Rehabilitation (CBR) For Disabled Persons in Cambodiaadkittipong100% (1)
- Unit 1 Study Guide Revised 01-09.doc AnswersDocument9 pagesUnit 1 Study Guide Revised 01-09.doc AnswersvickisscribdNo ratings yet
- Jurnal KesehatanDocument17 pagesJurnal KesehatanDiani Rista SariNo ratings yet
- Constructing The Slave BodyDocument18 pagesConstructing The Slave BodyFelis Chaus100% (1)
- EVS-BOOK-UNIT-7 CombineDocument37 pagesEVS-BOOK-UNIT-7 CombineAnshu KumarNo ratings yet
- AdverDocument13 pagesAdverHelen Meriz SagunNo ratings yet
- Livingood, Blake - Livingood Daily Your 21-Day Guide To Experience Real HealthDocument260 pagesLivingood, Blake - Livingood Daily Your 21-Day Guide To Experience Real HealthciperezNo ratings yet
- Grahani Rog PDFDocument3 pagesGrahani Rog PDFAnkit SainiNo ratings yet
- IralaDocument32 pagesIralaapi-26175717100% (3)