You might also like
- Difficult Acute Cholecystitis: Treatment and Technical IssuesFrom EverandDifficult Acute Cholecystitis: Treatment and Technical IssuesNo ratings yet
- Trauma de UretraDocument7 pagesTrauma de UretraJhoel QuellcaNo ratings yet
- The Ileoanal Pouch: A Practical Guide for Surgery, Management and TroubleshootingFrom EverandThe Ileoanal Pouch: A Practical Guide for Surgery, Management and TroubleshootingJanindra WarusavitarneNo ratings yet
- 3santucci 408 414Document7 pages3santucci 408 414Muh Ayyub PrimadiNo ratings yet
- Clinical Maxillary Sinus Elevation SurgeryFrom EverandClinical Maxillary Sinus Elevation SurgeryDaniel W. K. KaoNo ratings yet
- 231 - From Images in Urology Diagnosis and Management (Uday Patel M.B.CH.B., M.R.C.P. Etc.) (Z-Library)Document6 pages231 - From Images in Urology Diagnosis and Management (Uday Patel M.B.CH.B., M.R.C.P. Etc.) (Z-Library)Francisco BotelhoNo ratings yet
- Spilled Gallstones - Review of The Literature PDFDocument3 pagesSpilled Gallstones - Review of The Literature PDFZeeshaan Ahmed KhanNo ratings yet
- Bladder and Urethral Injury - ClinicalKeyDocument20 pagesBladder and Urethral Injury - ClinicalKeyKimberly Andrea Gramajo OrozcoNo ratings yet
- Giant Bladder Diverticulum Due To Previous Bullet Injury: Findings of Gadolinium-Enhanced Magnetic Resonance ImagingDocument4 pagesGiant Bladder Diverticulum Due To Previous Bullet Injury: Findings of Gadolinium-Enhanced Magnetic Resonance ImagingIrma Suriani DarwisNo ratings yet
- ROBIN. Small Bowel ObstructionDocument25 pagesROBIN. Small Bowel ObstructionRobin permadi100% (1)
- Bladder Injury PDFDocument7 pagesBladder Injury PDFaaaNo ratings yet
- Small-Bowel and Mesenteric Injuries in Blunt Trauma of The AbdomenDocument8 pagesSmall-Bowel and Mesenteric Injuries in Blunt Trauma of The AbdomenGina Kristina NanginNo ratings yet
- Webster Uretroplastia en 4 Etapas.Document13 pagesWebster Uretroplastia en 4 Etapas.LuisamdNo ratings yet
- Ureteric Calculi : Behaviour and WraithDocument7 pagesUreteric Calculi : Behaviour and Wraithvinay hrNo ratings yet
- 1 s2.0 S1089251608000486 MainDocument9 pages1 s2.0 S1089251608000486 MainHaya RihanNo ratings yet
- Ruptur Vesica Urinaria Case ReportDocument2 pagesRuptur Vesica Urinaria Case ReportAinun Jariah FahayNo ratings yet
- Cholecystogastric Fistula Penetrating Duodenum and Caused A Duodenal Obstruction A Case ReportDocument6 pagesCholecystogastric Fistula Penetrating Duodenum and Caused A Duodenal Obstruction A Case ReportHerald Scholarly Open AccessNo ratings yet
- Urinary System SurgeriesDocument34 pagesUrinary System SurgeriesShakil MahmodNo ratings yet
- Genitourinary Trauma: Kidney, Ureter, Bladder, Urethra, GenitaliaDocument42 pagesGenitourinary Trauma: Kidney, Ureter, Bladder, Urethra, GenitaliaOrin SujasmanNo ratings yet
- Ma 05011Document6 pagesMa 05011drelvNo ratings yet
- Caecocolic Intussusceptions in Horses: Clinical CommentaryDocument3 pagesCaecocolic Intussusceptions in Horses: Clinical CommentaryKiimBerly RcNo ratings yet
- RADIOLOGI JURNAL CampurDocument58 pagesRADIOLOGI JURNAL CampurderpNo ratings yet
- 079 - Bladder Trauma - (RSNA 2010)Document35 pages079 - Bladder Trauma - (RSNA 2010)Aswad AffandiNo ratings yet
- Radiological Investigation of The Biliary Tract: 1-Plain RadiographDocument11 pagesRadiological Investigation of The Biliary Tract: 1-Plain Radiographhussain AltaherNo ratings yet
- Case 1: Urological Trauma - Part 1Document2 pagesCase 1: Urological Trauma - Part 1HardiTariqHammaNo ratings yet
- El Khoury2018Document3 pagesEl Khoury2018peroksidaseNo ratings yet
- Medip,+ISJ 4325+CDocument3 pagesMedip,+ISJ 4325+CbrightozhrNo ratings yet
- Review Intravenous Urography and Imaging of The Urinary TractDocument27 pagesReview Intravenous Urography and Imaging of The Urinary TractBIntangsinagaNo ratings yet
- Ultrasonography of Bladder DisordersDocument23 pagesUltrasonography of Bladder DisordersmedicoscantareiraNo ratings yet
- Horton, K. M., Corl, F. M., & Fishman, E. K. (2000) - CT Evaluation of The Colon - Inflammatory Disease. RadioGraphics, 20 (2), 399-418Document20 pagesHorton, K. M., Corl, F. M., & Fishman, E. K. (2000) - CT Evaluation of The Colon - Inflammatory Disease. RadioGraphics, 20 (2), 399-418PauloCostaNo ratings yet
- Genitourinary Trauma: Sanjay Shewakramani,, Kevin C. ReedDocument18 pagesGenitourinary Trauma: Sanjay Shewakramani,, Kevin C. ReedKetan HijauNo ratings yet
- 10 TV Ca Cel TrasnsicionalesDocument19 pages10 TV Ca Cel TrasnsicionalesDonaldo ReleyNo ratings yet
- Ureteral Stent For Ureteral Stricture: James F. Borin and Elspeth M. McdougallDocument13 pagesUreteral Stent For Ureteral Stricture: James F. Borin and Elspeth M. McdougallOoNo ratings yet
- Bladder TraumaDocument43 pagesBladder TraumaSangeeta BSR100% (1)
- Bladder Injury: Types, Mechanisms, and Diagnostic Imaging: Jordan S. Gross, MD Scott Rotenberg, MD Mindy M. Horrow, MDDocument38 pagesBladder Injury: Types, Mechanisms, and Diagnostic Imaging: Jordan S. Gross, MD Scott Rotenberg, MD Mindy M. Horrow, MDTantyaNo ratings yet
- A Case of Urethrocutaneous Fistula A Forgotten Segment of A Broken UrethralDocument3 pagesA Case of Urethrocutaneous Fistula A Forgotten Segment of A Broken UrethralWardah Fauziah El SofwanNo ratings yet
- GUS CASE 5 - Fraktur PelvisDocument18 pagesGUS CASE 5 - Fraktur PelvisCassantha papjiNo ratings yet
- Materi Rupture BladderDocument4 pagesMateri Rupture Bladderendah desfindaNo ratings yet
- Abdominal X Ray Own NotesDocument12 pagesAbdominal X Ray Own NotesOrton UfmyNo ratings yet
- 9.renal InjuryDocument32 pages9.renal Injuryjitendra magarNo ratings yet
- Review ImagenesDocument23 pagesReview ImagenesJavierNo ratings yet
- Intestinalobstruction 150401053831 Conversion Gate01Document65 pagesIntestinalobstruction 150401053831 Conversion Gate01Nina NoviaNo ratings yet
- Trauma BuliDocument32 pagesTrauma BulimoonlightsoantaNo ratings yet
- Bladder TraumaDocument13 pagesBladder TraumaAnusikta PandaNo ratings yet
- Penis Injury After A FallDocument6 pagesPenis Injury After A FallIbrahim SabraNo ratings yet
- General Considerations: o o o o o o oDocument9 pagesGeneral Considerations: o o o o o o ovitaNo ratings yet
- Injuries To The Genito Urinary TractDocument83 pagesInjuries To The Genito Urinary TractHj. Andi SatinjariNo ratings yet
- Stump LeakageDocument3 pagesStump LeakageNuraqila Mohd murshidNo ratings yet
- Abdominal X Rays Made Easy - CalcificationDocument4 pagesAbdominal X Rays Made Easy - CalcificationMinh TanNo ratings yet
- Radiographic Imaging: Lane S. PalmerDocument24 pagesRadiographic Imaging: Lane S. PalmerFierda Ovita AzhariNo ratings yet
- Lecture 8 Surgical Umbilicus 2016Document6 pagesLecture 8 Surgical Umbilicus 2016Iyaloo ShiimiNo ratings yet
- Module 1 Acute Scrotum PDFDocument11 pagesModule 1 Acute Scrotum PDFbayutrihatmajaNo ratings yet
- Laparoscopic Cholecystectomy: 1. Abdominal Cavity ApproachDocument7 pagesLaparoscopic Cholecystectomy: 1. Abdominal Cavity ApproachTeja Laksana NukanaNo ratings yet
- Obstruction EDocument87 pagesObstruction ETimbur IgorNo ratings yet
- Kosma 2009Document4 pagesKosma 2009Falon PapalangiNo ratings yet
- Urinary SurgeryDocument10 pagesUrinary SurgeryClassic BobbyNo ratings yet
- Radiology Secrets - 2nd EdDocument12 pagesRadiology Secrets - 2nd EdD T50% (8)
- Duplication of Gallbladder: Case ReportDocument3 pagesDuplication of Gallbladder: Case ReportVenanda RianNo ratings yet
- Describe The Radiological Anatomy of The Male Urinary Bladder. Describe in Detail The Techniques For Demonstrating The OrganDocument43 pagesDescribe The Radiological Anatomy of The Male Urinary Bladder. Describe in Detail The Techniques For Demonstrating The OrganMichael IdowuNo ratings yet
- Gallstone Ileus: An Unusual Cause of Intestinal ObstructionDocument7 pagesGallstone Ileus: An Unusual Cause of Intestinal ObstructionSiska Eni WijayantiNo ratings yet
- Abnormal PuerperiumDocument23 pagesAbnormal PuerperiumLynee OlvianaNo ratings yet
- Anaphylaxis: Learning ObjectivesDocument4 pagesAnaphylaxis: Learning Objectivesmohamed fahmyNo ratings yet
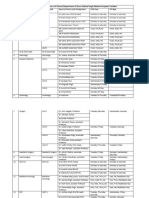
- OPD and OT Days of Doctors of Clinical Department of Guru Gobind Singh Medical HospitalDocument4 pagesOPD and OT Days of Doctors of Clinical Department of Guru Gobind Singh Medical HospitalBohar singh Brar BrarNo ratings yet
- Folleto Medicamentos de Alto Riesgo GeneralidadesDocument1 pageFolleto Medicamentos de Alto Riesgo GeneralidadesGabee MoralesNo ratings yet
- Australian Seniors Ride Digital Care WaveDocument11 pagesAustralian Seniors Ride Digital Care Waveivg8562No ratings yet
- Sample RFPDocument7 pagesSample RFPrahul kNo ratings yet
- Nonlinear PharmacokineticsDocument22 pagesNonlinear PharmacokineticsNadya Prafita100% (1)
- Defination of FireDocument21 pagesDefination of FireVikas YamagarNo ratings yet
- Sustained Release Drug Delivery System Potential: The Pharma InnovationDocument13 pagesSustained Release Drug Delivery System Potential: The Pharma InnovationprinceamitNo ratings yet
- Occupational Health and Safety ChecklistDocument6 pagesOccupational Health and Safety ChecklistpaurushgodharNo ratings yet
- YANG SHENG 2011 October B PDFDocument70 pagesYANG SHENG 2011 October B PDFSasa PuiuNo ratings yet
- HIV Peer Training Toolkit GuideDocument73 pagesHIV Peer Training Toolkit GuideGatot SandyNo ratings yet
- Module 3 - Integration of BADAC Plan To BPOPS - NBOODocument15 pagesModule 3 - Integration of BADAC Plan To BPOPS - NBOOSharamae DalogdogNo ratings yet
- The Practical Design & Implementation of Small-Sided Conditioned Games (SSCGS)Document1 pageThe Practical Design & Implementation of Small-Sided Conditioned Games (SSCGS)Husan ThapaNo ratings yet
- WWW - England.nhs - Uk: Business Continuity Management NHS WorkshopDocument52 pagesWWW - England.nhs - Uk: Business Continuity Management NHS WorkshopForbetNo ratings yet
- Local Anesthetics AgentsDocument56 pagesLocal Anesthetics AgentsIyad Abou-Rabii100% (1)
- 1 SMDocument14 pages1 SMRosalina Pertiwi GultomNo ratings yet
- v4n2 9pdfDocument10 pagesv4n2 9pdfissaninNo ratings yet
- Jerusalem SyndromeDocument5 pagesJerusalem Syndromele_papillon15No ratings yet
- Ozlex Tea ADocument3 pagesOzlex Tea AbiancaNo ratings yet
- DISABILITYDocument9 pagesDISABILITYSyeda AttqaNo ratings yet
- Important Numbers For SMLEDocument3 pagesImportant Numbers For SMLEAkpevwe EmefeNo ratings yet
- Republic of The PhilippinesDocument24 pagesRepublic of The PhilippinesMarie France Suarin100% (1)
- Cruz Marissa Resume CsusbDocument3 pagesCruz Marissa Resume Csusbapi-341233003No ratings yet
- Dry Acide Dessolution Unit FreesenuisDocument59 pagesDry Acide Dessolution Unit FreesenuisokboNo ratings yet
- By Dinesh GannerllaDocument74 pagesBy Dinesh GannerllagannerllaNo ratings yet
- Ultimate Frisbee DraftDocument3 pagesUltimate Frisbee Draftapi-526745820No ratings yet
- ACTI-Mag Brochure 2016Document4 pagesACTI-Mag Brochure 2016Atharva UlangwarNo ratings yet
- Child and Adolescent Developmental StagesDocument26 pagesChild and Adolescent Developmental StagesLaila PagdilaoNo ratings yet
- Peds - Research ArticleDocument2 pagesPeds - Research Articleapi-662219485No ratings yet