You might also like
- Diagnosis and Treatment of Vestibular DisordersFrom EverandDiagnosis and Treatment of Vestibular DisordersSeilesh BabuNo ratings yet
- Is Modern Perioperative Care Too Complicated For Surgeons?: ReferencesDocument2 pagesIs Modern Perioperative Care Too Complicated For Surgeons?: ReferencesHasriana BudimanNo ratings yet
- 2013 Knee Prolotherapy RCTDocument9 pages2013 Knee Prolotherapy RCTReyn JohnsonNo ratings yet
- Acta Anaesthesiologica Taiwanica: Editorial ViewDocument2 pagesActa Anaesthesiologica Taiwanica: Editorial ViewShuaib AhmedNo ratings yet
- 1 s2.0 S0003999319303892 MainDocument8 pages1 s2.0 S0003999319303892 MainRizkyrafiqoh afdinNo ratings yet
- Fascitis Plantar PRPDocument4 pagesFascitis Plantar PRPBelen QWNo ratings yet
- Anestesi Umum Dan Regional Untuk Operasi Fraktur Hip: Ameta-Analisis Uji Coba Secara AcakDocument13 pagesAnestesi Umum Dan Regional Untuk Operasi Fraktur Hip: Ameta-Analisis Uji Coba Secara AcakmardianaNo ratings yet
- The Study To Assess The Effect of Prehabilitation On Postoperative Outcome of The Patients On Total Knee Arthroplasty at Selected HospitalDocument4 pagesThe Study To Assess The Effect of Prehabilitation On Postoperative Outcome of The Patients On Total Knee Arthroplasty at Selected HospitalEditor IJTSRDNo ratings yet
- Vertebroplastia Evidencia 1 USADocument11 pagesVertebroplastia Evidencia 1 USAandres donnetNo ratings yet
- Randomized Clinical Trial Investigating The Stress Response From Two Different Methods of Analgesia After Laparoscopic Colorectal SurgeryDocument7 pagesRandomized Clinical Trial Investigating The Stress Response From Two Different Methods of Analgesia After Laparoscopic Colorectal Surgeryvalerio.messinaNo ratings yet
- Tangtiphaiboontana 2021Document8 pagesTangtiphaiboontana 2021翁嘉聰No ratings yet
- Glasgow Prognostic Score Class 2 Predicts Prolonged Intensive Care Unit Stay in Patients Undergoing PneumonectomyDocument7 pagesGlasgow Prognostic Score Class 2 Predicts Prolonged Intensive Care Unit Stay in Patients Undergoing PneumonectomyDavide RadiceNo ratings yet
- Rooij Et Al-2016-Arthritis Care & ResearchDocument12 pagesRooij Et Al-2016-Arthritis Care & ResearchJennifer JaneNo ratings yet
- Vertebrplasty 2016Document10 pagesVertebrplasty 2016karenNo ratings yet
- Parade New AnakDocument10 pagesParade New AnakMukhizalNo ratings yet
- StudyDocument23 pagesStudyJose Paul RaderNo ratings yet
- Rehabilitation Versus Surgical Reconstruction For Non-Acute Anterior Cruciate Ligament InjuryDocument11 pagesRehabilitation Versus Surgical Reconstruction For Non-Acute Anterior Cruciate Ligament InjuryJesusNavarrete97No ratings yet
- What's New in Spine Surgery: Specialty UpdateDocument11 pagesWhat's New in Spine Surgery: Specialty UpdatePoliceNo ratings yet
- Anaesthesia - 2017 - ChrimesDocument6 pagesAnaesthesia - 2017 - Chrimesannasoares02No ratings yet
- Osteoarthritis of The HipDocument2 pagesOsteoarthritis of The HipDewi WulansariNo ratings yet
- 4.RCT Oliveira2015Document10 pages4.RCT Oliveira2015elproedrosNo ratings yet
- 189-198 FukatoVol8No3 PDFDocument10 pages189-198 FukatoVol8No3 PDFIndah YulantariNo ratings yet
- Knee Osteoarthritis: Steriods Verus Platelets Rich Plasma EffectivenessDocument5 pagesKnee Osteoarthritis: Steriods Verus Platelets Rich Plasma EffectivenessInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Altman 2004Document8 pagesAltman 2004MeltemNo ratings yet
- 2021 Dextrose Prolotherapy in Knee Osteoarthritis A Systematic Review and Meta-AnalysisDocument10 pages2021 Dextrose Prolotherapy in Knee Osteoarthritis A Systematic Review and Meta-AnalysiswanhsiorthopedicsNo ratings yet
- Physiotherapy For Plantar Fasciitis - A UK Wide Survey of Current PracticeDocument29 pagesPhysiotherapy For Plantar Fasciitis - A UK Wide Survey of Current PracticeCambriaChicoNo ratings yet
- 1 s2.0 S1836955319300918 Main PDFDocument7 pages1 s2.0 S1836955319300918 Main PDFJuliano BritoNo ratings yet
- Watermark 7Document14 pagesWatermark 7PKM BANGSRI INo ratings yet
- Microwave Ablation of Osteoid OsteomasDocument2 pagesMicrowave Ablation of Osteoid OsteomasAmritNo ratings yet
- Research Paper On EpiduralDocument7 pagesResearch Paper On Epiduralezkugohkf100% (1)
- Regional AnalgesiaDocument5 pagesRegional AnalgesiajdjhdNo ratings yet
- moura2021Document10 pagesmoura2021Phoenix WhiteNo ratings yet
- Impact of Exercise On The Functional Capacity and Pain of Patients With Knee Osteoarthritis: A Randomized Clinical TrialDocument7 pagesImpact of Exercise On The Functional Capacity and Pain of Patients With Knee Osteoarthritis: A Randomized Clinical TrialSunithaNo ratings yet
- 1 s2.0 S000709122030444X MainDocument2 pages1 s2.0 S000709122030444X MainFabiola AcostaNo ratings yet
- Manejo No Quirugico de La Artrosis de Rodilla CaderaDocument12 pagesManejo No Quirugico de La Artrosis de Rodilla CaderaCesar C SNo ratings yet
- Improving Management of Neonatal Infections: CommentDocument3 pagesImproving Management of Neonatal Infections: CommentShofi Dhia AiniNo ratings yet
- Lewis 2016Document1 pageLewis 2016Adjhy Aji AchmadNo ratings yet
- GR Up: SM Orthopedics & Muscular SystemDocument6 pagesGR Up: SM Orthopedics & Muscular SystemValerie BpNo ratings yet
- 8Document1 page8Daniel GuevaraNo ratings yet
- Laparoscopic Vs Open Distal Pancreatectomy: A Single-Institution Comparative StudyDocument6 pagesLaparoscopic Vs Open Distal Pancreatectomy: A Single-Institution Comparative StudyHana YunikoNo ratings yet
- 1 s2.0 S0039606020302725 MainDocument1 page1 s2.0 S0039606020302725 MainRafael Calleja LozanoNo ratings yet
- Comparison of Three Sitting Positions For Combined Spinal - Epidural Anesthesia: A Multicenter Randomized Controlled TrialDocument8 pagesComparison of Three Sitting Positions For Combined Spinal - Epidural Anesthesia: A Multicenter Randomized Controlled TrialFadhilNo ratings yet
- Can Endoscopic Atrophy Predict Histological Atrophy? Historical Study in United Kingdom and JapanDocument12 pagesCan Endoscopic Atrophy Predict Histological Atrophy? Historical Study in United Kingdom and JapanJosseph EscobarNo ratings yet
- The Journal of ArthroplastyDocument6 pagesThe Journal of ArthroplastyKarla milNo ratings yet
- Journal of Orthopaedics: Case ReportDocument7 pagesJournal of Orthopaedics: Case ReportDita AldiniNo ratings yet
- --Low-Level Laser Therapy at 635 nm for Treatment of Chronic Plantar Fasciitis. A Placebo-Controlled, Randomized StudyDocument5 pages--Low-Level Laser Therapy at 635 nm for Treatment of Chronic Plantar Fasciitis. A Placebo-Controlled, Randomized StudymarioNo ratings yet
- Early Mobilization: Why, What For and How?: ReviewDocument8 pagesEarly Mobilization: Why, What For and How?: ReviewViviane SalazarNo ratings yet
- Wilson Smith2017Document28 pagesWilson Smith2017FaisalNo ratings yet
- Pi Is 0140673616321663Document2 pagesPi Is 0140673616321663bagasNo ratings yet
- Endoscopic Findings of The Gastric Mucosa During Long Term Use of Proton Pump Inhibitor A Multicenter StudyDocument6 pagesEndoscopic Findings of The Gastric Mucosa During Long Term Use of Proton Pump Inhibitor A Multicenter StudySamuel0651No ratings yet
- Ultrasoud Guidance For Lumbar PunctureDocument12 pagesUltrasoud Guidance For Lumbar PunctureDavid Avellaneda TalledoNo ratings yet
- RecoveryDocument139 pagesRecoveryIgnacio VázquezNo ratings yet
- Soni 2010Document4 pagesSoni 2010AlejandroVeraVargasNo ratings yet
- Deambulacion Vs Reposo en CPPDocument10 pagesDeambulacion Vs Reposo en CPPNoé Alejandro SánchezNo ratings yet
- Adductor Canal Block Versus Femoral Canal Block For Total Knee Arthroplasty - A Meta-Analysis 3Document7 pagesAdductor Canal Block Versus Femoral Canal Block For Total Knee Arthroplasty - A Meta-Analysis 3angelama1783riosNo ratings yet
- 2018 - OARSI GuidelinesDocument12 pages2018 - OARSI GuidelinesGuilherme AugustoNo ratings yet
- Thesis DeepakDocument72 pagesThesis DeepakDeepak SugumarNo ratings yet
- Treatment of Neck Pain With Myofascial Therapies: A Single Blind Randomized Controlled TrialDocument11 pagesTreatment of Neck Pain With Myofascial Therapies: A Single Blind Randomized Controlled TrialBTS LGONo ratings yet
- The Ability of Prehabilitation To Influence Postoperative Outcome After Intra-Abdominal Operation: A Systematic Review and Meta-AnalysisDocument13 pagesThe Ability of Prehabilitation To Influence Postoperative Outcome After Intra-Abdominal Operation: A Systematic Review and Meta-AnalysisHAriNo ratings yet
- Baru &Document6 pagesBaru &Bianca CaterinalisendraNo ratings yet
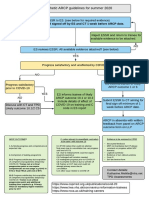
- Draft ARCP Guidelines Summer 2020Document1 pageDraft ARCP Guidelines Summer 2020tomlawson88No ratings yet
- Royal College X AnesthesiaDocument66 pagesRoyal College X AnesthesiaManuela CormioNo ratings yet
- Annex F - ICMDocument34 pagesAnnex F - ICMtomlawson88No ratings yet
- Annex E - AdvancedDocument68 pagesAnnex E - Advancedtomlawson88No ratings yet
- TRG CCT AnnexgDocument40 pagesTRG CCT AnnexgManuela CormioNo ratings yet
- 216 9411 Anaes (Consultant Anaesthetist) 4Document22 pages216 9411 Anaes (Consultant Anaesthetist) 4tomlawson88No ratings yet
- Catastrophes in Anaesthetic Practice - Dealing With The AftermathDocument32 pagesCatastrophes in Anaesthetic Practice - Dealing With The Aftermathtomlawson88No ratings yet
- Drug and Alcohol Abuse 2011 0Document40 pagesDrug and Alcohol Abuse 2011 0tomlawson88No ratings yet
- ADocument1 pageAtomlawson88No ratings yet
- Anaesthesia For Tension Free Vaginal TapeDocument1 pageAnaesthesia For Tension Free Vaginal Tapetomlawson88No ratings yet
- Liver, GI and MetabolismDocument54 pagesLiver, GI and Metabolismtomlawson88No ratings yet
- Liver, GI and MetabolismDocument54 pagesLiver, GI and Metabolismtomlawson88No ratings yet
- Topics Left To CoverDocument1 pageTopics Left To Covertomlawson88No ratings yet
- The Hitchens DecalogueDocument1 pageThe Hitchens Decaloguetomlawson88No ratings yet
- Training in Anaesthesia – the Essential CurriculumDocument2 pagesTraining in Anaesthesia – the Essential Curriculumtomlawson88No ratings yet
- Book ReviewDocument1 pageBook Reviewtomlawson88No ratings yet
- Level of Cords of Brachial Plexus Lateral, Medial and Posterior (Named According To Relation To Axillary Artery)Document6 pagesLevel of Cords of Brachial Plexus Lateral, Medial and Posterior (Named According To Relation To Axillary Artery)tomlawson88No ratings yet
- Stats For Primary FRCADocument7 pagesStats For Primary FRCAtomlawson88No ratings yet
- Review Question - GI PDFDocument10 pagesReview Question - GI PDFTee BeeNo ratings yet
- Digestive SystemDocument10 pagesDigestive SystemSweets Jar80% (5)
- Digestion and Absorption: SolutionsDocument12 pagesDigestion and Absorption: SolutionsSeekerNo ratings yet
- EnzymesDocument5 pagesEnzymesLea IoaNo ratings yet
- Fight The Obesity EpidemicDocument102 pagesFight The Obesity EpidemicJorianditha RamadhanNo ratings yet
- Mind Body NutritionDocument76 pagesMind Body Nutritionenver100% (3)
- Digestio NDocument27 pagesDigestio NSauban AhmedNo ratings yet
- Test Bank Of Basic Nutrition and Diet Therapy 14th EditionDocument24 pagesTest Bank Of Basic Nutrition and Diet Therapy 14th EditionronneldeleyvaNo ratings yet
- 1.about Some GIT Hormones (True or False)Document71 pages1.about Some GIT Hormones (True or False)JOSEPH NDERITU100% (2)
- Bsczo 301Document386 pagesBsczo 301JjelNo ratings yet
- Biochemistry of Digestive System FKUH 2017Document207 pagesBiochemistry of Digestive System FKUH 2017ummuabNo ratings yet
- Neuroendocrine Control of Food IntakeDocument11 pagesNeuroendocrine Control of Food IntakeO KiNo ratings yet
- Transduksi Sinyal Hormon Kolesistokinin Sebagai TaDocument11 pagesTransduksi Sinyal Hormon Kolesistokinin Sebagai TaNadhya AgathaNo ratings yet
- List of Human HormonesDocument7 pagesList of Human HormonesKeerthana BathojuNo ratings yet
- Digestive System PowerpointDocument65 pagesDigestive System Powerpointapi-263357086No ratings yet
- Git MovementsDocument7 pagesGit MovementsTrinity PdplNo ratings yet
- Benelam 2009 Nutrition - BulletinDocument48 pagesBenelam 2009 Nutrition - BulletinCarlos Julio Fonseca SilvaNo ratings yet
- Gastrointestinal Hormones: A Mini-Review: European Journal Pharmaceutical and Medical Research April 2022Document6 pagesGastrointestinal Hormones: A Mini-Review: European Journal Pharmaceutical and Medical Research April 2022Yared gebremedhinNo ratings yet
- The ASPEN Adult Nutrition Support Core Curriculum, 3 RD EditionDocument1,246 pagesThe ASPEN Adult Nutrition Support Core Curriculum, 3 RD EditionTrinh85% (13)
- Digestion and absorption multiple choice questionsDocument46 pagesDigestion and absorption multiple choice questionsAmbika dawadiNo ratings yet
- Army Public School, Kirkee: Human Digestive Organ-StomachDocument16 pagesArmy Public School, Kirkee: Human Digestive Organ-StomachV Deepak KumarNo ratings yet
- Neet Digestion systemMCQDocument58 pagesNeet Digestion systemMCQiGadgetProNo ratings yet
- Regulation of Food IntakeDocument18 pagesRegulation of Food IntakeenriNo ratings yet
- Regulation of GIT by gastrointestinal hormonesDocument13 pagesRegulation of GIT by gastrointestinal hormonesRaja Rashid IqbalNo ratings yet
- Digestive SystemDocument9 pagesDigestive SystemJhomar B, Dela CruzNo ratings yet
- Intestinal and Colonic Physiology and Biochemistry (Part 2 - Secretion, Digestion, Absorption) (Slides With Notes)Document69 pagesIntestinal and Colonic Physiology and Biochemistry (Part 2 - Secretion, Digestion, Absorption) (Slides With Notes)kuchipuchi12No ratings yet
- Aiims Nov 2010 Review by Tanmay MehtaDocument56 pagesAiims Nov 2010 Review by Tanmay MehtaGIST (Gujarat Institute of Science & Technology)No ratings yet
- Regulation of Food IntakeDocument15 pagesRegulation of Food Intakezsf8m52ky4No ratings yet
- Biokimia - DR - Maehan Hardjo M.biomed PHDDocument159 pagesBiokimia - DR - Maehan Hardjo M.biomed PHDHerryNo ratings yet
- Chemical Coordination and Integration: SolutionsDocument10 pagesChemical Coordination and Integration: SolutionsIhtisham Ul HaqNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (41)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)