You might also like
- NCM 107A Pedia Week 5-7 Growth and DevelopmentDocument30 pagesNCM 107A Pedia Week 5-7 Growth and DevelopmentInsatiable CleeNo ratings yet
- Children's psicology and disturbility in evolutive age: What they are and how they workFrom EverandChildren's psicology and disturbility in evolutive age: What they are and how they workNo ratings yet
- Principles of Growth and Development of Children-B.Ed NotesDocument3 pagesPrinciples of Growth and Development of Children-B.Ed NotesLtfr RhmnNo ratings yet
- Chapter 011Document13 pagesChapter 011dtheart2821100% (2)
- PROF ED 2-Module 1Document7 pagesPROF ED 2-Module 1Ma KenNo ratings yet
- Changes in The Brain. This Period of Development Begins DuringDocument7 pagesChanges in The Brain. This Period of Development Begins DuringmelanieNo ratings yet
- Human Development N LearningDocument15 pagesHuman Development N LearningAsad NomanNo ratings yet
- Stages of Human DevelopmentDocument9 pagesStages of Human DevelopmentMardy SarcaugaNo ratings yet
- Ed.1 Module MidtermDocument90 pagesEd.1 Module MidtermNABUA MARY CRYSTALLINE S.100% (1)
- Module 1Document11 pagesModule 1ZONETTE PAREDONo ratings yet
- JRMSU Child Development Course SyllabusDocument8 pagesJRMSU Child Development Course SyllabusKewkew AzilearNo ratings yet
- ED101 MODULE 2 Lesson 1 & 2Document9 pagesED101 MODULE 2 Lesson 1 & 2Clifford Villarubia LaboraNo ratings yet
- Check My Twitter Account @nursetopia or IG @nursetopia1 For More Nursing Test Banks, Sample Exam, Reviewers, and NotesDocument32 pagesCheck My Twitter Account @nursetopia or IG @nursetopia1 For More Nursing Test Banks, Sample Exam, Reviewers, and NotesNurse UtopiaNo ratings yet
- Unit-5 060607Document4 pagesUnit-5 060607John Mark AlagonNo ratings yet
- Chapter 5 Typical and A Typical Development Among ChildrenDocument44 pagesChapter 5 Typical and A Typical Development Among ChildrenJohn carlo TugayNo ratings yet
- 991566643090unit-7 - Child and Human DevelopmentDocument15 pages991566643090unit-7 - Child and Human DevelopmentGaganpreet Kaur Fashion DesigningNo ratings yet
- C5 Typical and Atypical DevelopmentDocument5 pagesC5 Typical and Atypical DevelopmentMary Ann Bandola100% (3)
- New Ed101 Module 2 2Document24 pagesNew Ed101 Module 2 2aizaNo ratings yet
- Megatrends: The Future of Filipino: Human DevelopmentDocument17 pagesMegatrends: The Future of Filipino: Human DevelopmentJessy Grace Costo - TizonNo ratings yet
- Unit 1Document13 pagesUnit 1rajNo ratings yet
- Growth and Development, Paediatric NursingDocument26 pagesGrowth and Development, Paediatric NursingJimcyNo ratings yet
- Development of The Learners at Various StagesDocument1 pageDevelopment of The Learners at Various StagesGenkakuNo ratings yet
- Prof Ed. 1-Child and Adolescent Development: Learning Module 1 Human Development: Meaning, Concepts and ApproachesDocument7 pagesProf Ed. 1-Child and Adolescent Development: Learning Module 1 Human Development: Meaning, Concepts and ApproachesLEA ROSE VALENo ratings yet
- Local Media123349414965696629Document25 pagesLocal Media123349414965696629Ebale RoelNo ratings yet
- FTC 101 Module 1Document5 pagesFTC 101 Module 1Jamie Layson Dela CruzNo ratings yet
- Educ. 1-ADocument13 pagesEduc. 1-AMizzael Dayahan Abuel85% (41)
- Module in ED 101-Child and Adolescent Learners and Learning PrinciplesDocument54 pagesModule in ED 101-Child and Adolescent Learners and Learning PrinciplesCassy Casey100% (3)
- Psy 311 Notes 2021Document147 pagesPsy 311 Notes 2021austinoyugi08No ratings yet
- Dwnload Full Health Physical Assessment in Nursing 2nd Edition Damico Test Bank PDFDocument35 pagesDwnload Full Health Physical Assessment in Nursing 2nd Edition Damico Test Bank PDFcaunakirillx100% (9)
- Human Growth & Devpt.Document29 pagesHuman Growth & Devpt.kiromokelvinNo ratings yet
- College of Education: San Jose Community CollegeDocument4 pagesCollege of Education: San Jose Community CollegeAnabel Jason Bobiles100% (3)
- Ed. 7 Module 5 AnswerDocument5 pagesEd. 7 Module 5 AnswerMea MagdayaoNo ratings yet
- Human DevelopmentpptxDocument20 pagesHuman DevelopmentpptxRembe Belleno100% (1)
- EED02 Notes1Document8 pagesEED02 Notes1Lem Merob100% (1)
- Why Good Physical Health is Necessary for Good LearnersDocument16 pagesWhy Good Physical Health is Necessary for Good LearnersHaroon Karim BalochNo ratings yet
- The Child and Adolescent Learners and The Learning PrinciplesDocument30 pagesThe Child and Adolescent Learners and The Learning PrinciplesmayetteNo ratings yet
- Human Development Module from Cebu Technological UniversityDocument14 pagesHuman Development Module from Cebu Technological UniversityJewel SkyNo ratings yet
- Goverment CollegeDocument7 pagesGoverment CollegeFatima KhanNo ratings yet
- Health Education's Progression To The Forefront of Health PromotionDocument18 pagesHealth Education's Progression To The Forefront of Health Promotionbernadette_olaveNo ratings yet
- l2 Child HealthDocument84 pagesl2 Child HealthNur AinaaNo ratings yet
- Human Development PrinciplesDocument5 pagesHuman Development PrinciplesRave LegoNo ratings yet
- Module 2 Educ 1011Document5 pagesModule 2 Educ 1011Aileen GalanzaNo ratings yet
- Child Dev Stages & ConceptsDocument34 pagesChild Dev Stages & ConceptsJustine Marquizo SanoriaNo ratings yet
- Typical and Atypical Development Among ChildrenDocument15 pagesTypical and Atypical Development Among ChildrenJohn guyll AtilanoNo ratings yet
- Module in ED101 Child and Adolescent Learners and Learning Principles PDFDocument61 pagesModule in ED101 Child and Adolescent Learners and Learning Principles PDFAnjela April93% (100)
- Chapter - Two: Human DevelopmentDocument43 pagesChapter - Two: Human DevelopmentBacha TarekegnNo ratings yet
- Chap5 Typical and Atypical DevelopmentDocument5 pagesChap5 Typical and Atypical DevelopmentCheyNo ratings yet
- Child Development - Basic Concepts & Principles: Learning OutcomesDocument31 pagesChild Development - Basic Concepts & Principles: Learning Outcomessmxlpxngx98100% (1)
- Human Development ModuleDocument2 pagesHuman Development Moduledonix100% (1)
- L1-L3 CALLP ModuleDocument7 pagesL1-L3 CALLP ModuleMelanie ClenuarNo ratings yet
- Report 4 - Fem3101Document39 pagesReport 4 - Fem3101Mutiara SyafiqahNo ratings yet
- Qtr-1-Module 2 Developing The Whole PersonDocument14 pagesQtr-1-Module 2 Developing The Whole PersonRaiza Cabrera100% (1)
- CAD Activities 1-3Document20 pagesCAD Activities 1-3Crissalyn Sanico Estrella100% (1)
- GROWTH AND DEVELOPMENTDocument8 pagesGROWTH AND DEVELOPMENTJade GordoncilloNo ratings yet
- m2 & d1 Theories and DevelopmentDocument16 pagesm2 & d1 Theories and DevelopmentDaniel John HaighNo ratings yet
- Human Development: Meaning, Concepts and ApproachesDocument8 pagesHuman Development: Meaning, Concepts and ApproachesAsida Maronsing DelionNo ratings yet
- EU LP Module. UNIT 1Document49 pagesEU LP Module. UNIT 1assessor rizalNo ratings yet
- Per Dev Module 5Document17 pagesPer Dev Module 5q2750336No ratings yet
- Arco - Unit 1Document9 pagesArco - Unit 1Jovel ConsularNo ratings yet
- The Best Foods For Erectile DysfunctionDocument13 pagesThe Best Foods For Erectile DysfunctionSophia ChloeNo ratings yet
- Science 8 Summative Exam Q4Document4 pagesScience 8 Summative Exam Q4Kelvin Jason ArellanoNo ratings yet
- Malabsorption Syndrome: Causes, Symptoms and TreatmentDocument5 pagesMalabsorption Syndrome: Causes, Symptoms and TreatmentPriyaNo ratings yet
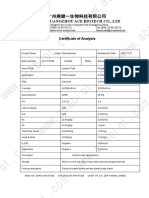
- COA of Konjac GlucomannanDocument1 pageCOA of Konjac GlucomannanPan EmmaNo ratings yet
- Food Nutrition Consumer MarketsDocument2 pagesFood Nutrition Consumer MarketsGlenzchie TaguibaoNo ratings yet
- Vegemite Triple Decker Sandwich RecipeDocument1 pageVegemite Triple Decker Sandwich RecipeJoedy-Beth Dolom0% (1)
- SITHCCC005 Student Assessment Tasks - UPDATEDDocument21 pagesSITHCCC005 Student Assessment Tasks - UPDATEDSagar PanchalNo ratings yet
- Kelly Wright hw499 Unit 4 AssignmentDocument9 pagesKelly Wright hw499 Unit 4 Assignmentapi-526258935No ratings yet
- Nasogastric Feeding GuidelineDocument25 pagesNasogastric Feeding GuidelineElse FashiosNo ratings yet
- RBE-EXAM-LECTUREDocument38 pagesRBE-EXAM-LECTURELowellyn Grezen VillaflorNo ratings yet
- OnenotDocument7 pagesOnenotJenison AdonisNo ratings yet
- Past TenseDocument5 pagesPast TenseTrâm AnhNo ratings yet
- Food and Nutrition MarikaDocument21 pagesFood and Nutrition Marikammeemz360No ratings yet
- Outline Format Problem SolutionDocument2 pagesOutline Format Problem SolutionSofia Torres FlorezNo ratings yet
- Breaking Down Fitness Dogmas: A Healthy Diet Is Only 25% NutritionDocument3 pagesBreaking Down Fitness Dogmas: A Healthy Diet Is Only 25% NutritionrheyNo ratings yet
- Foods that Boost MoodDocument12 pagesFoods that Boost MoodAnrica Ferdianti100% (1)
- Speaking Vstep Part 1Document7 pagesSpeaking Vstep Part 1lan quynhNo ratings yet
- Processing and Marketing Goat ProductsDocument57 pagesProcessing and Marketing Goat ProductsCAPT. MOHD KHAIRUL ANAM ILIASNo ratings yet
- Food and Nutrition Research Institute (FNRI) Food Guide PyramidDocument28 pagesFood and Nutrition Research Institute (FNRI) Food Guide PyramidWincy SalazarNo ratings yet
- Ai DietitianDocument14 pagesAi DietitianMr.Ashok SNo ratings yet
- Cmca Unit 3 RuayaDocument12 pagesCmca Unit 3 RuayaMarc Glico ComonNo ratings yet
- Prepare Vegetable Dishes.3Document54 pagesPrepare Vegetable Dishes.3Antonette OcampoNo ratings yet
- 1st Final Draft LNAP 2022Document51 pages1st Final Draft LNAP 2022ruby ultrA100% (1)
- ĐỀ CƯƠNG ÔN TẬP HỌC KÌ I GLOBAL SUCCESSDocument6 pagesĐỀ CƯƠNG ÔN TẬP HỌC KÌ I GLOBAL SUCCESSCúcNo ratings yet
- Bone Growth and DevelopmentDocument3 pagesBone Growth and DevelopmentTroy Albert MirandaNo ratings yet
- Cutting Meal Plan 210 230 Pound ManDocument2 pagesCutting Meal Plan 210 230 Pound ManGeorge VNo ratings yet
- Biochemistry Nutrition and DieteticsDocument23 pagesBiochemistry Nutrition and DieteticsSaad Zafar AwanNo ratings yet
- Life Sciences p1 Memo Gr11 Nov 2020 Eng DDocument10 pagesLife Sciences p1 Memo Gr11 Nov 2020 Eng Dmokoenakoketso018No ratings yet
- PQCNC 2023 Nutrition in PregnancyDocument12 pagesPQCNC 2023 Nutrition in PregnancykcochranNo ratings yet
- Quarter 3 Lesson on Student Diet and ShoppingDocument4 pagesQuarter 3 Lesson on Student Diet and ShoppingPhạm Khắc TrungNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (14)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)
- Daniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisFrom EverandDaniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisRating: 3.5 out of 5 stars3.5/5 (130)
- Troubled: A Memoir of Foster Care, Family, and Social ClassFrom EverandTroubled: A Memoir of Foster Care, Family, and Social ClassRating: 4.5 out of 5 stars4.5/5 (24)
- Nonviolent Communication by Marshall B. Rosenberg - Book Summary: A Language of LifeFrom EverandNonviolent Communication by Marshall B. Rosenberg - Book Summary: A Language of LifeRating: 4.5 out of 5 stars4.5/5 (50)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- The Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeFrom EverandThe Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeNo ratings yet
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingFrom EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingRating: 4 out of 5 stars4/5 (1138)