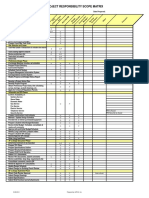
You might also like
- MatrixDocument3 pagesMatrixfarhanyazdaniNo ratings yet
- Physiology Summary Chapter 20Document9 pagesPhysiology Summary Chapter 20gail01850% (2)
- Case Analysis Presentation CvaDocument82 pagesCase Analysis Presentation CvaVhince Norben PiscoNo ratings yet
- Vascular Ultrasound Protocol Guide PDFDocument28 pagesVascular Ultrasound Protocol Guide PDFchica_as100% (2)
- D61762GC31 Les06-Data TypesDocument22 pagesD61762GC31 Les06-Data TypesUPPKH ProvKalselNo ratings yet
- Healthcare - Nursing Care Plan - Decreased Cardiac OutputDocument4 pagesHealthcare - Nursing Care Plan - Decreased Cardiac OutputBenjamin CañalitaNo ratings yet
- Congestive Cardiac FailureDocument38 pagesCongestive Cardiac FailureSalman KhanNo ratings yet
- 7,8-Antihypertensive Drugs PDFDocument10 pages7,8-Antihypertensive Drugs PDFSaktai DiyamiNo ratings yet
- Ingredient Vulnerability Assessment BRCDocument3 pagesIngredient Vulnerability Assessment BRCSherylNo ratings yet
- Transculturalism and Transcultural Liter PDFDocument211 pagesTransculturalism and Transcultural Liter PDFLucas Accastello ChNo ratings yet
- Atherosclerosis, Dyslipidaemia and Diabetes SlidesDocument75 pagesAtherosclerosis, Dyslipidaemia and Diabetes SlidesdanradulescuNo ratings yet
- Antidislipidemic DrugsDocument25 pagesAntidislipidemic DrugsAlda Gitu RahmaNo ratings yet
- E 03 H 3 JobsDocument4 pagesE 03 H 3 JobsSarah Azizah WiratamaNo ratings yet
- ZCA SMDaet CutReport All 14062023to20062023Document2 pagesZCA SMDaet CutReport All 14062023to20062023Patricia LacoNo ratings yet
- Figure 10. Junior Highschool Students Question 10 AnswersDocument1 pageFigure 10. Junior Highschool Students Question 10 Answerslovely graceNo ratings yet
- Walmart GRRDocument174 pagesWalmart GRRPatricia DillonNo ratings yet
- Mortality (Global)Document3 pagesMortality (Global)Daniel Angelo ArangoNo ratings yet
- Bad PDFCreatorDocument3 pagesBad PDFCreatorapi-3766300100% (2)
- Online Marketing Overview: Jon SummerfieldDocument14 pagesOnline Marketing Overview: Jon SummerfieldRmsgNo ratings yet
- WMC 2016 Prospectus June 2016 PDFDocument87 pagesWMC 2016 Prospectus June 2016 PDFAnonymous 0gfzLMYYfXNo ratings yet
- UndanganDocument1 pageUndanganrudianNo ratings yet
- Mother Goose Family GuideDocument4 pagesMother Goose Family GuideKamil KANTARCIOĞLUNo ratings yet
- ZCA QuixKioskSMSorsogon CutReport All 13062023to20062023Document2 pagesZCA QuixKioskSMSorsogon CutReport All 13062023to20062023Patricia LacoNo ratings yet
- Grafix DFPM LightdiffuserDocument4 pagesGrafix DFPM LightdiffuserfiskitNo ratings yet
- Third Quarter Update ReviewDocument26 pagesThird Quarter Update Reviewelong3102No ratings yet
- Using DDL Statements to Create and Manage Tables: license to use this Student GuideฺDocument40 pagesUsing DDL Statements to Create and Manage Tables: license to use this Student GuideฺSiranjeevi GnanamNo ratings yet
- Kaartrailion Shuttles Maart04Document1 pageKaartrailion Shuttles Maart04Meedenken en Doen BVNo ratings yet
- Monitoring ToolsDocument14 pagesMonitoring ToolsStephanie CastillonNo ratings yet
- SGD Evaluation Feedback Q2 2019Document4 pagesSGD Evaluation Feedback Q2 2019Lugawan ni Bro OfficeNo ratings yet
- GJMH All Rotomoulded Product CatalogueDocument8 pagesGJMH All Rotomoulded Product CatalogueAbhishek JaiswalNo ratings yet
- Menahga School District's 2023-2024 Certified Staff Seniority ListDocument7 pagesMenahga School District's 2023-2024 Certified Staff Seniority ListShannon GeisenNo ratings yet
- DatasetDocument341 pagesDatasetSanath Fernando100% (1)
- Mymulti Fare MapDocument1 pageMymulti Fare MapanandnagsNo ratings yet
- Gspaper 1 Book 3Document57 pagesGspaper 1 Book 3minatoackerman69No ratings yet
- No. Votes For Senator: TA L Senator'S NameDocument3 pagesNo. Votes For Senator: TA L Senator'S Namekathlyn obayanNo ratings yet
- 2022 11 16 RCC Enhanced Brochure FINAL V6Document21 pages2022 11 16 RCC Enhanced Brochure FINAL V6Darren ChenNo ratings yet
- Hutts: A Seed Is Sleepy, and A Butterfly Is PatientDocument40 pagesHutts: A Seed Is Sleepy, and A Butterfly Is PatientHaseeb ToorNo ratings yet
- EmptyDocument5 pagesEmptySullivan F'gNo ratings yet
- MONOGRAPH First Children's Embassy in The World MEGJASHI 1992-2022, 30 YearsDocument300 pagesMONOGRAPH First Children's Embassy in The World MEGJASHI 1992-2022, 30 YearsFIRST CHILDREN'S EMBASSY IN THE WORLD MEGJASHI MACEDONIANo ratings yet
- Problem Statements 2023: StoriesDocument136 pagesProblem Statements 2023: StoriesSuryaprakash MishraNo ratings yet
- A Kind of MagicDocument2 pagesA Kind of MagichappyNo ratings yet
- Bukti 1.29.5Document8 pagesBukti 1.29.5didiNo ratings yet
- Det-Tronics Flame DetectionDocument2 pagesDet-Tronics Flame DetectionGabriel MendezNo ratings yet
- Tabel GrafikDocument2 pagesTabel Grafikfatmaasri112No ratings yet
- Tema4 PositivePsychologyDocument16 pagesTema4 PositivePsychologyCristinaNo ratings yet
- Walt Disney Studios Top Grossing MoviesDocument7 pagesWalt Disney Studios Top Grossing MoviesBerenice Montiel HernandezNo ratings yet
- VICTRON ENERGY Solar System Sizing - DAYS With PV - EnglishDocument1 pageVICTRON ENERGY Solar System Sizing - DAYS With PV - EnglishJanfer EstradaNo ratings yet
- 6392 1 Assam Internal Security 193830Document21 pages6392 1 Assam Internal Security 193830Alka RanaNo ratings yet
- 002 002abx Gne 261223Document4 pages002 002abx Gne 261223toavuhNo ratings yet
- 001bx Sin 261223Document2 pages001bx Sin 261223toavuhNo ratings yet
- Shree Amar Kalyan Secondary School, Maijogmai, Ilam: T NV Iro NM en Ed Uc Ati OnDocument1 pageShree Amar Kalyan Secondary School, Maijogmai, Ilam: T NV Iro NM en Ed Uc Ati OnDB BhandariNo ratings yet
- 30th Sept Protest - PosterDocument1 page30th Sept Protest - PosteredenmorecdpNo ratings yet
- Achievement ChartDocument14 pagesAchievement ChartGlenzchie TaguibaoNo ratings yet
- Top OH-12th Export of Goods To Korea in 2016Document2 pagesTop OH-12th Export of Goods To Korea in 2016Korea Economic Institute of America (KEI)No ratings yet
- Profile en PDFDocument19 pagesProfile en PDFNouman EnterprisesNo ratings yet
- Continuum 3 ZZDocument1 pageContinuum 3 ZZdimitre79No ratings yet
- Karlas Chao Unit1b Thesis Briefing Document Part 2Document29 pagesKarlas Chao Unit1b Thesis Briefing Document Part 2Karlas ChaoNo ratings yet
- Document To MSA PDFDocument239 pagesDocument To MSA PDFdipak5939No ratings yet
- Muscle Contraction, Fatigue & Exercise 22 PDFDocument77 pagesMuscle Contraction, Fatigue & Exercise 22 PDFFAHMI ASSIDIQINo ratings yet
- Mind Mapping ConsonantDocument1 pageMind Mapping ConsonantIka FatraNo ratings yet
- Co Un T) : Shree Amar Kalyan Secondary School, Maijogmai 1 Nayabazar, IlamDocument4 pagesCo Un T) : Shree Amar Kalyan Secondary School, Maijogmai 1 Nayabazar, IlamDB BhandariNo ratings yet
- Bunn VPR Parts ManualDocument26 pagesBunn VPR Parts Manualsatx840No ratings yet
- The Crimson Cowboys: The Remarkable Odyssey of the 1931 Claflin-Emerson ExpeditionFrom EverandThe Crimson Cowboys: The Remarkable Odyssey of the 1931 Claflin-Emerson ExpeditionNo ratings yet
- Circulatory System 1641908954579 SCDocument4 pagesCirculatory System 1641908954579 SCJ15No ratings yet
- Heart Failure: Roro WigidDocument29 pagesHeart Failure: Roro WigidroroNo ratings yet
- Clinical Practice Guidelines On The Management of Visceral AneurysmsDocument37 pagesClinical Practice Guidelines On The Management of Visceral AneurysmsSarah KaderNo ratings yet
- Cardiovasular SystemDocument5 pagesCardiovasular SystemAsher Eby VargeeseNo ratings yet
- Instant Download Ebook PDF Ekg Plain and Simple 4th Edition by Karen Ellis PDF ScribdDocument41 pagesInstant Download Ebook PDF Ekg Plain and Simple 4th Edition by Karen Ellis PDF Scribdjason.smalley210100% (45)
- ECCO 2 Hemodynamics TestDocument3 pagesECCO 2 Hemodynamics TestpamoralesNo ratings yet
- Malignant Hypertension - Dr. Todung PDFDocument12 pagesMalignant Hypertension - Dr. Todung PDFMuhammad Khoirul SodiqNo ratings yet
- Roger Hainsworth (Auth.), Marek Malik (Eds.) - Clinical Guide To Cardiac Autonomic Tests-Springer Netherlands (1998)Document425 pagesRoger Hainsworth (Auth.), Marek Malik (Eds.) - Clinical Guide To Cardiac Autonomic Tests-Springer Netherlands (1998)Victor LauneNo ratings yet
- Antianginal DrugsDocument19 pagesAntianginal DrugsAnusha ZubairNo ratings yet
- Prediktor Kegagalan Intervensi Koroner Perkutan Pada Oklusi Total Di Pusat Jantung Nasional, IndonesiaDocument9 pagesPrediktor Kegagalan Intervensi Koroner Perkutan Pada Oklusi Total Di Pusat Jantung Nasional, IndonesiaNining AnjarwatiNo ratings yet
- MCQ CardiologyDocument2 pagesMCQ Cardiologyvishaljairam100% (1)
- Varicose VeinDocument32 pagesVaricose VeinBhavana NambiarNo ratings yet
- Radcliffe EducationDocument4 pagesRadcliffe EducationSherwin Buenavente SulitNo ratings yet
- CVS AdaptationDocument20 pagesCVS AdaptationAlya KamarrudenNo ratings yet
- Artificial HeartDocument17 pagesArtificial HeartRAKESHKANNAN100% (1)
- Cardiovascular System (Lecture 1)Document55 pagesCardiovascular System (Lecture 1)Ranime A. FatouhNo ratings yet
- Framingham Data Famous Cohort Study of 5209 Subjects From Framingham MADocument2 pagesFramingham Data Famous Cohort Study of 5209 Subjects From Framingham MAEdwin Johny Asnate SalazarNo ratings yet
- Slide JR UGD SaktaDocument39 pagesSlide JR UGD SaktaWayan GunawanNo ratings yet
- 4-Pulp Vessels FactoidDocument4 pages4-Pulp Vessels FactoidmoffittajNo ratings yet
- Cor Pulmonale IkaDocument19 pagesCor Pulmonale IkaIka Lukita SariNo ratings yet
- Budd-Chiari Syndrome: Spectrum of Imaging FindingsDocument9 pagesBudd-Chiari Syndrome: Spectrum of Imaging FindingsDanaAmaranducaiNo ratings yet
- Material Mini NetterDocument13 pagesMaterial Mini NetterVALENTINA ALBORNOZ BASTÍASNo ratings yet
- Compensatory Mechanism of Circulatory ShockDocument29 pagesCompensatory Mechanism of Circulatory ShockWan Razin Wan Hassan100% (1)
- Systolic MurmursDocument10 pagesSystolic MurmursRizqan Fahlevvi AkbarNo ratings yet