You might also like
- Undrugged: Sleep: From Insomnia to Un-Somnia -- Why Sleeping Pills Don’T Improve Sleep and the Drug-Free Solutions That WillFrom EverandUndrugged: Sleep: From Insomnia to Un-Somnia -- Why Sleeping Pills Don’T Improve Sleep and the Drug-Free Solutions That WillRating: 5 out of 5 stars5/5 (2)
- Myasthenia Gravis, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandMyasthenia Gravis, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
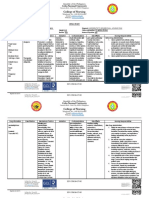
- College of Nursing: Cebu Normal UniversityDocument11 pagesCollege of Nursing: Cebu Normal Universityvivi's eyebrowsNo ratings yet
- 3 E. Drug StudyDocument4 pages3 E. Drug StudySarrah MaramagNo ratings yet
- Discuss Mechanism of Action As To How It Can Resolve Identified Condition, Signs and Symptoms, or Nursing ConditionsDocument5 pagesDiscuss Mechanism of Action As To How It Can Resolve Identified Condition, Signs and Symptoms, or Nursing ConditionsMenard VelascoNo ratings yet
- PediaDocument8 pagesPediaChloe CabingatanNo ratings yet
- Pregabalin LYricaDocument2 pagesPregabalin LYricaKristine Young100% (3)
- CNS: Headache, InsomniaDocument5 pagesCNS: Headache, InsomniaDave FagaritaNo ratings yet
- Drug Study FormatDocument7 pagesDrug Study FormatHAIDER JULAILINo ratings yet
- Tramadol DS PDFDocument6 pagesTramadol DS PDFSawada TsunayoshiNo ratings yet
- Re Me RonDocument2 pagesRe Me RonKatie McPeekNo ratings yet
- PrednisoneDocument1 pagePrednisoneCassieNo ratings yet
- Drug Study: Name of Drug Action Indication Adverse Effect Nursing ResponsibilityDocument4 pagesDrug Study: Name of Drug Action Indication Adverse Effect Nursing ResponsibilityBel CortezNo ratings yet
- Drug Study - LevetiracetamDocument3 pagesDrug Study - LevetiracetamCath Bril100% (4)
- Activity 4 F PsychiaLab DrugStudyDocument36 pagesActivity 4 F PsychiaLab DrugStudyVinz OñoNo ratings yet
- Dextroamphetamine ADHD Drug StudyDocument1 pageDextroamphetamine ADHD Drug StudyBeatrice ManingasNo ratings yet
- Behavioral Health Care PlanDocument13 pagesBehavioral Health Care Planapi-521003884No ratings yet
- PhenobarbitalDocument6 pagesPhenobarbitalGwyn RosalesNo ratings yet
- Meadows Paige Case StudyDocument16 pagesMeadows Paige Case Studyapi-607727110No ratings yet
- Drug LopressorDocument1 pageDrug LopressorSrkocherNo ratings yet
- Risperdone and Lithium CarbonateDocument4 pagesRisperdone and Lithium CarbonateFionah RetuyaNo ratings yet
- DrugStudy RazadyneDocument4 pagesDrugStudy RazadyneArone SebastianNo ratings yet
- CatapresDocument1 pageCatapresCen Janber CabrillosNo ratings yet
- DesyrelDocument1 pageDesyrelKatie McPeekNo ratings yet
- Sickle Cell - RahafDocument39 pagesSickle Cell - RahafgalalNo ratings yet
- 2011 Updates in Therapeutics: P P: The Pharmacotherapy Preparatory Review and Recertification CourseDocument11 pages2011 Updates in Therapeutics: P P: The Pharmacotherapy Preparatory Review and Recertification CourseDrx ahmed MaherNo ratings yet
- DrugStudy - CamaristaColeenMaeC (BSN III-G) (Prednisone)Document2 pagesDrugStudy - CamaristaColeenMaeC (BSN III-G) (Prednisone)Coleen Mae CamaristaNo ratings yet
- Pathophysiology: Depressed Mood Loss of Interest and Pleasure in ActivitiesDocument4 pagesPathophysiology: Depressed Mood Loss of Interest and Pleasure in ActivitiesBrittany VandermeulenNo ratings yet
- PSY Supplement mhGAP-IG v2Document10 pagesPSY Supplement mhGAP-IG v2Jay TamNo ratings yet
- NCM107 Lab Drug Study Manalo BSN 2BDocument4 pagesNCM107 Lab Drug Study Manalo BSN 2BBethrice MelegritoNo ratings yet
- Drug Study 7th Floor Ucmed RotationDocument6 pagesDrug Study 7th Floor Ucmed RotationVinz OñoNo ratings yet
- Drug StudyDocument3 pagesDrug StudyPang ProjectNo ratings yet
- Drug ZoloftDocument1 pageDrug ZoloftSrkocherNo ratings yet
- Drugs PediaDocument3 pagesDrugs PediaMark Ianne AngNo ratings yet
- Drug StudyDocument7 pagesDrug StudyLyka PerezNo ratings yet
- NCM106 - Pharmacology: History: Hypersensitivity To Phenobarbital, Porphyria, PregnancyDocument2 pagesNCM106 - Pharmacology: History: Hypersensitivity To Phenobarbital, Porphyria, PregnancyBrandy RectoNo ratings yet
- Jall Jsot Dap PresentationDocument13 pagesJall Jsot Dap Presentationapi-383172592No ratings yet
- Lab or Diagnostic Test Patient's Value Normal ValueDocument9 pagesLab or Diagnostic Test Patient's Value Normal ValueJormarie NogueNo ratings yet
- Babon - MS Ward ReqtsDocument13 pagesBabon - MS Ward Reqtschristelleannebabon196No ratings yet
- Schizophrenia (Paliperidone) 2Document1 pageSchizophrenia (Paliperidone) 2Bukola OgunnaikeNo ratings yet
- Re QuipDocument1 pageRe QuipKatie McPeekNo ratings yet
- Nursing Care Plan #1 Mental HealthDocument13 pagesNursing Care Plan #1 Mental HealthNursyNurseNo ratings yet
- Captopril Drug StudyDocument5 pagesCaptopril Drug StudyFaye Andrea Francisco100% (1)
- Med Ward DrugsDocument4 pagesMed Ward DrugsMark Ianne AngNo ratings yet
- Careplan 2Document10 pagesCareplan 2api-520843051No ratings yet
- برزنتيشن هديك١Document22 pagesبرزنتيشن هديك١Abdallah AlquranNo ratings yet
- DRUGDocument6 pagesDRUGjhoyorlyn22No ratings yet
- Pharmacologic ClassDocument4 pagesPharmacologic ClassBianca Nicole Gacad FernandezNo ratings yet
- CymbaltaDocument2 pagesCymbaltaAdrianne Bazo100% (1)
- Tramadol Drug-StudyDocument3 pagesTramadol Drug-StudyPang ProjectNo ratings yet
- Memantine AD Drug StudyDocument1 pageMemantine AD Drug StudyBeatrice ManingasNo ratings yet
- Clozapine Drug StudyDocument2 pagesClozapine Drug StudyAlex Silvano100% (2)
- Drug Study: Atropine: RecommendedDocument6 pagesDrug Study: Atropine: RecommendedShara Lailanie A. AzisNo ratings yet
- Drug Analysis 1Document8 pagesDrug Analysis 1Sophia MarieNo ratings yet
- Forcadilla Medsurg Drug StudyDocument12 pagesForcadilla Medsurg Drug StudyKeir Mrls ForcadillaNo ratings yet
- Pain in Elderly Group 3 1Document26 pagesPain in Elderly Group 3 1Maica Lectana100% (1)
- Drug CiproDocument1 pageDrug CiproSrkocherNo ratings yet
- A Simple Guide to Myasthenia Gravis (Updated), Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Myasthenia Gravis (Updated), Diagnosis, Treatment and Related ConditionsNo ratings yet
- Autonomic Nervous System & Homeopathy: Personalized Nutrition Concept Depicted in Homeopathy & AyurvedaFrom EverandAutonomic Nervous System & Homeopathy: Personalized Nutrition Concept Depicted in Homeopathy & AyurvedaNo ratings yet
- Why Use Natural Healing: A Comparison of the Science and Efficacy of Natural Healing with That of PharmaceuticalsFrom EverandWhy Use Natural Healing: A Comparison of the Science and Efficacy of Natural Healing with That of PharmaceuticalsNo ratings yet
- Interpretation of Abgs: Sophie TatishviliDocument14 pagesInterpretation of Abgs: Sophie Tatishvilimashe1No ratings yet
- Neonatal Seizures - VillaroyaDocument9 pagesNeonatal Seizures - VillaroyaChristy CarmelNo ratings yet
- Edu Adhd PaperDocument8 pagesEdu Adhd Paperapi-534406008No ratings yet
- NURSING CARE PLAN - SeizureDocument2 pagesNURSING CARE PLAN - Seizurederic91% (54)
- Standards For Bipolar Excellence - STABLE - Toolkit PDFDocument67 pagesStandards For Bipolar Excellence - STABLE - Toolkit PDFSophie257100% (1)
- Schizophrenia ReportDocument28 pagesSchizophrenia ReportsksanisidrogensanNo ratings yet
- Real-Life Clinical Experience With Cariprazine - A Systematic Review of Case StudiesDocument17 pagesReal-Life Clinical Experience With Cariprazine - A Systematic Review of Case Studiesbelloilportogallo99No ratings yet
- Research - Drug Rehabilitation CenterDocument6 pagesResearch - Drug Rehabilitation CenterDan Czar T. JuanNo ratings yet
- Antepartum - AbortionDocument5 pagesAntepartum - AbortionBench AvilaNo ratings yet
- Mid Term-Essay On Drug AddictionDocument12 pagesMid Term-Essay On Drug AddictionShubho Dev nathNo ratings yet
- Day 6 - Module # 6 - Primary & Secondary Survey, Helmet Removal, Cervial Collar, Spine ImmobilizaDocument28 pagesDay 6 - Module # 6 - Primary & Secondary Survey, Helmet Removal, Cervial Collar, Spine ImmobilizaBloody DoctorNo ratings yet
- Vertebrobasilar SyndromeDocument14 pagesVertebrobasilar SyndromeHitesh RohitNo ratings yet
- Mcmi III Essentials InterpretationDocument56 pagesMcmi III Essentials InterpretationZeine Daoudi100% (6)
- Case 4 - Neuro RoyalDocument20 pagesCase 4 - Neuro RoyalkvintumbelNo ratings yet
- Physiocure Consent FormDocument1 pagePhysiocure Consent FormHarram SajjadNo ratings yet
- Facultad de Psicología: Universidad Anáhuac México Campus NorteDocument4 pagesFacultad de Psicología: Universidad Anáhuac México Campus NorteJaneth GmNo ratings yet
- Mood DisordersDocument10 pagesMood DisordersHarvey T. Dato-onNo ratings yet
- Goldberg's Bipolar Screening ScaleDocument2 pagesGoldberg's Bipolar Screening ScaleVisesh100% (2)
- Approach To Dementia Author Schulich School of Medicine and Dentistry Western UniversityDocument18 pagesApproach To Dementia Author Schulich School of Medicine and Dentistry Western UniversitySHERIF ZAHERNo ratings yet
- JeremyDocument2 pagesJeremyManjuNo ratings yet
- PIM3 CalculatorDocument9 pagesPIM3 CalculatorFernando Elcyede LinoNo ratings yet
- Safety (Wounds)Document32 pagesSafety (Wounds)kay_genius252No ratings yet
- Miriti M.D Masters of Clinical Medicine Accidents and Emergency Peadiatrics Emergencies Ii Facilitators: DR Mburugu DR SimbaDocument32 pagesMiriti M.D Masters of Clinical Medicine Accidents and Emergency Peadiatrics Emergencies Ii Facilitators: DR Mburugu DR SimbaDennis MiritiNo ratings yet
- Pediatric FirstAid CPR AEDDocument12 pagesPediatric FirstAid CPR AEDVirtuepearlsNo ratings yet
- Alteraciones Neuropsicológicas en EpilepsiaDocument6 pagesAlteraciones Neuropsicológicas en EpilepsiaClaudiaAcuñaZapataNo ratings yet
- Insulin ShockDocument9 pagesInsulin ShockMarina CiburciuNo ratings yet
- Adhd Diva - 5Document20 pagesAdhd Diva - 5quaz486% (14)
- Research Paper.g10Document10 pagesResearch Paper.g10Fake EmailNo ratings yet
- Pediatric Sleep Disorders PDFDocument70 pagesPediatric Sleep Disorders PDFMalay P. Khamnuengkhuan100% (1)
- Shock Management, by Ayman RawehDocument15 pagesShock Management, by Ayman RawehaymxNo ratings yet