You might also like
- 4 Physiology of Neonatal SkinDocument7 pages4 Physiology of Neonatal SkinAna Li SingNo ratings yet
- Cousins 2014Document10 pagesCousins 2014maria-roosNo ratings yet
- Blan Pain 2009Document12 pagesBlan Pain 2009inforNo ratings yet
- 2021 - Neonatal Dermatology The Normal, The Common and The SeriousDocument14 pages2021 - Neonatal Dermatology The Normal, The Common and The SeriousnancyerlenNo ratings yet
- Basic Physiology of The SkinDocument4 pagesBasic Physiology of The SkinRegina SinagaNo ratings yet
- Schwartz Cpap 16 Skin and Subcutaneous TissueDocument16 pagesSchwartz Cpap 16 Skin and Subcutaneous TissueRem AlfelorNo ratings yet
- "Vision Without Action Is A Daydream. Action Without Vision Is A Nightmare." Japanese ProverbDocument22 pages"Vision Without Action Is A Daydream. Action Without Vision Is A Nightmare." Japanese Proverb123456100% (1)
- RenovhyalDocument8 pagesRenovhyalMaritaNetoNo ratings yet
- 11 Vesiculopustular, Bullous and Erosive Diseases of The NeonateDocument20 pages11 Vesiculopustular, Bullous and Erosive Diseases of The Neonatecgs08No ratings yet
- 08.16.16 Skin Histo Pathol (Nanney) HandoutDocument14 pages08.16.16 Skin Histo Pathol (Nanney) HandoutDan WuiytNo ratings yet
- M13 - Dermatology - Chapter 1Document10 pagesM13 - Dermatology - Chapter 1Idham BaharudinNo ratings yet
- Experimental Dermatology - 2008 - Proksch - The Skin An Indispensable BarrierDocument10 pagesExperimental Dermatology - 2008 - Proksch - The Skin An Indispensable BarrierDanna Valentina MartinezNo ratings yet
- M13 v2 Dermatology & STI - LO3Document8 pagesM13 v2 Dermatology & STI - LO3medipro clinicNo ratings yet
- Skin 2Document1 pageSkin 2BonesNo ratings yet
- Fitzpatrick - S Dermatology in General Medicine 8thDocument42 pagesFitzpatrick - S Dermatology in General Medicine 8thorchitarosadila haryonoNo ratings yet
- Protective Mechanism of The Body (Mucous Membrane)Document3 pagesProtective Mechanism of The Body (Mucous Membrane)Kirk CobainNo ratings yet
- Chapter 5 - Growth & Differentiation of The EpidermisDocument6 pagesChapter 5 - Growth & Differentiation of The EpidermisMary RiveroNo ratings yet
- Physiology of Neonatal Skin: A. Mudrikah H Dirgahayu 2017-84-027 Pembimbing: Dr. Hanny Tanasal, Sp. KKDocument20 pagesPhysiology of Neonatal Skin: A. Mudrikah H Dirgahayu 2017-84-027 Pembimbing: Dr. Hanny Tanasal, Sp. KKMudrikahHaniyahNo ratings yet
- Capitulo 1 MckeeDocument37 pagesCapitulo 1 MckeeEdu LopezNo ratings yet
- 2017 - Tecnología CosméticaDocument54 pages2017 - Tecnología CosméticaCésar Rosado Avila ToñoNo ratings yet
- Integumentary SystemDocument24 pagesIntegumentary SystemWadabiNo ratings yet
- Skin Barrier Defects in AtopicDocument20 pagesSkin Barrier Defects in AtopicDaniel SatyoNo ratings yet
- Development Team: Pharmaceutical Sciences Cosmetics Skin Care ProductsDocument26 pagesDevelopment Team: Pharmaceutical Sciences Cosmetics Skin Care Productschi nguyenNo ratings yet
- 2 - Nihms571891Document9 pages2 - Nihms571891mimatechcontabilidadNo ratings yet
- LorenzDocument8 pagesLorenzShreyaNo ratings yet
- Schwartz's Principles of Surgery: CH16: Page 1Document13 pagesSchwartz's Principles of Surgery: CH16: Page 1Kathryn ReunillaNo ratings yet
- Keratinocytes - Innate Immune Cells in Atopic DermatitisDocument15 pagesKeratinocytes - Innate Immune Cells in Atopic DermatitisMing XianNo ratings yet
- Emm 19992Document15 pagesEmm 19992cibif40663No ratings yet
- Chapter 15:: Epidermal and Dermal Adhesion:: Leena Bruckner-Tuderman &Document7 pagesChapter 15:: Epidermal and Dermal Adhesion:: Leena Bruckner-Tuderman &nazhifah apotekerNo ratings yet
- Anatomy and Physiology: Key FeaturesDocument4 pagesAnatomy and Physiology: Key Featuresorchitarosadila haryonoNo ratings yet
- Kamus ManusiaDocument822 pagesKamus ManusiaAhmad Abdullah100% (1)
- Integumentary System: Stratum BasaleDocument21 pagesIntegumentary System: Stratum BasalerinaNo ratings yet
- Structure & Funtion NailsDocument5 pagesStructure & Funtion NailsrikaNo ratings yet
- Sistema Inmune y PielDocument53 pagesSistema Inmune y PielKevin MendozaNo ratings yet
- 10 1097@won 0000000000000029Document3 pages10 1097@won 0000000000000029Maria Paula Castiblanco SosaNo ratings yet
- Lai Cheong2013Document4 pagesLai Cheong2013Nirwana SeptianiNo ratings yet
- Anatomy and PhysiologyDocument14 pagesAnatomy and Physiologynanel25No ratings yet
- Anatomy and Physiology of SkinDocument12 pagesAnatomy and Physiology of Skinjose abadNo ratings yet
- Journal Written Report - Scar Prevention With Prolonged Use of Tissue AdhesiveDocument13 pagesJournal Written Report - Scar Prevention With Prolonged Use of Tissue AdhesiveNeill CelesteNo ratings yet
- RetinoidDocument22 pagesRetinoidPresstisa AxeliaNo ratings yet
- LEC - ACTIVITY5 - INTEGUMENTARY - SYSTEM - Copy - Cruz - SilveroDocument5 pagesLEC - ACTIVITY5 - INTEGUMENTARY - SYSTEM - Copy - Cruz - SilveroGeia Marie SilveroNo ratings yet
- Dr. Kurniati - Eliminating Dead Skin Cell Face and Body 0kt 2022Document27 pagesDr. Kurniati - Eliminating Dead Skin Cell Face and Body 0kt 2022wiwinNo ratings yet
- What Are The Properties of Normal SkinDocument102 pagesWhat Are The Properties of Normal Skinlovely_dyaNo ratings yet
- Ultraviolet Light, Toxin.: PEDIATRICS Vol. 113 No. 4 April 2004Document8 pagesUltraviolet Light, Toxin.: PEDIATRICS Vol. 113 No. 4 April 2004abhijit_gothoskar6039No ratings yet
- Keloids and Hypertrophic Scars: Pathophysiology, Classification, and TreatmentDocument16 pagesKeloids and Hypertrophic Scars: Pathophysiology, Classification, and TreatmentStella SunurNo ratings yet
- Skin Structure and Function: Applied Dermatotoxicology. DOI: © 2014 Elsevier Inc. All Rights ReservedDocument10 pagesSkin Structure and Function: Applied Dermatotoxicology. DOI: © 2014 Elsevier Inc. All Rights ReservedArsene AngelaNo ratings yet
- Phtsiology Hystology of The Skin. Primary & Secondary Morphological ElementsDocument21 pagesPhtsiology Hystology of The Skin. Primary & Secondary Morphological Elementsgrreddy8364320No ratings yet
- Chapter 14:: Skin Barrier:: Akiharu Kubo & Masayuki AmagaiDocument21 pagesChapter 14:: Skin Barrier:: Akiharu Kubo & Masayuki Amagaililis nur faridaNo ratings yet
- Giải phẫu ứng dụngDocument54 pagesGiải phẫu ứng dụngDũng Hoàng Nghĩa TríNo ratings yet
- Campus Collusio N: Review Questions For Test PreparationDocument3 pagesCampus Collusio N: Review Questions For Test PreparationGenna LedesmaNo ratings yet
- Types of Cells in The EpidermisDocument13 pagesTypes of Cells in The EpidermisSairelle Sordilla Obang83% (6)
- The Effect of Purple Mangosteen Peel Extract On Photoaging: A Literature ReviewDocument5 pagesThe Effect of Purple Mangosteen Peel Extract On Photoaging: A Literature ReviewNabila NatasyaNo ratings yet
- Stem Cell Dynamics, Migration and Plasticity During Wound HealingDocument20 pagesStem Cell Dynamics, Migration and Plasticity During Wound Healingro111111No ratings yet
- Skin Basic Structure and FunctionDocument11 pagesSkin Basic Structure and FunctionPanggih Sekar Palupi IINo ratings yet
- Structure and Function of The SkinDocument8 pagesStructure and Function of The SkinricardoarturoquezadacayambeNo ratings yet
- Anatomy, Skin (Integument), Epidermis - StatPearls - NCBI BookshelfDocument8 pagesAnatomy, Skin (Integument), Epidermis - StatPearls - NCBI Bookshelfpka25No ratings yet
- Skin SubstitutesDocument3 pagesSkin Substitutessilvio da costa guerreiroNo ratings yet
- Core Curriculum WOCNSDocument1,212 pagesCore Curriculum WOCNSJerry MaguireNo ratings yet
- Birth InjuriesDocument4 pagesBirth InjuriesHarshal KhadeNo ratings yet
- Blistering DisordersDocument4 pagesBlistering DisordersHarshal KhadeNo ratings yet
- Care of Neonatal and Preterm SkinDocument5 pagesCare of Neonatal and Preterm SkinHarshal KhadeNo ratings yet
- Blistering DisordersDocument4 pagesBlistering DisordersHarshal KhadeNo ratings yet
- Birth InjuriesDocument4 pagesBirth InjuriesHarshal KhadeNo ratings yet
- Antenatal Ultrasound - Its Utility and LimitationsDocument9 pagesAntenatal Ultrasound - Its Utility and LimitationsHarshal KhadeNo ratings yet
- Class 12 Maths Project On Prime NumbersDocument13 pagesClass 12 Maths Project On Prime Numbersanon_3835245630% (1)
- Mini-Case 1 Ppe AnswerDocument11 pagesMini-Case 1 Ppe Answeryu choong100% (2)
- BS746 2014Document22 pagesBS746 2014marco SimonelliNo ratings yet
- Lecture5 PDE 2016Document22 pagesLecture5 PDE 2016isele1977No ratings yet
- YellowstoneDocument1 pageYellowstoneOana GalbenuNo ratings yet
- Class 12 - Maths - MatricesDocument87 pagesClass 12 - Maths - MatricesAishwarya MishraNo ratings yet
- SAT Biochar Ethylene Poster 10 - 10b PDFDocument1 pageSAT Biochar Ethylene Poster 10 - 10b PDFsherifalharamNo ratings yet
- 10th Aug. 2011 Structural Calculation (For Sub.) - 03Document29 pages10th Aug. 2011 Structural Calculation (For Sub.) - 03Nguyễn Tiến Việt100% (1)
- Hurricanes Grade5Document3 pagesHurricanes Grade5Anonymous m3yrUPNo ratings yet
- LPPDocument4 pagesLPPMargarida ReisNo ratings yet
- Manufacuring EngineeringDocument3 pagesManufacuring Engineeringapi-79207659No ratings yet
- Accsap 10 VHDDocument94 pagesAccsap 10 VHDMuhammad Javed Gaba100% (2)
- Comparison of 3 Tests To Detect Acaricide ResistanDocument4 pagesComparison of 3 Tests To Detect Acaricide ResistanMarvelous SungiraiNo ratings yet
- 9701 w09 QP 21Document12 pages9701 w09 QP 21Hubbak KhanNo ratings yet
- Chapter 04 Product and ServDocument43 pagesChapter 04 Product and ServAlireza AlborziNo ratings yet
- Prawn ProcessingDocument21 pagesPrawn ProcessingKrishnaNo ratings yet
- Properties of Matter ReviewDocument8 pagesProperties of Matter Reviewapi-290100812No ratings yet
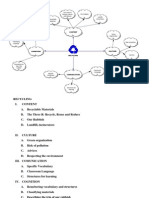
- Recycling Mind MapDocument2 pagesRecycling Mind Mapmsole124100% (1)
- Bhagwati School Strap Report AnalysisDocument60 pagesBhagwati School Strap Report AnalysisReverse Minded100% (1)
- Pref - 2 - Grammar 1.2 - Revisión Del IntentoDocument2 pagesPref - 2 - Grammar 1.2 - Revisión Del IntentoJuan M. Suarez ArevaloNo ratings yet
- Leadership Games and ActivitiesDocument38 pagesLeadership Games and ActivitiesWilliam Oliss100% (1)
- Action Analysis For Animators by Chris WebsterDocument409 pagesAction Analysis For Animators by Chris WebsterThomas Yandex100% (8)
- Texto CuritibaDocument1 pageTexto CuritibaMargarida GuimaraesNo ratings yet
- BECO UACE Chem2Document6 pagesBECO UACE Chem2EMMANUEL BIRUNGINo ratings yet
- LighthouseDocument4 pagesLighthousejaneborn5345No ratings yet
- Reactive Dyes For Digital Textile Printing InksDocument4 pagesReactive Dyes For Digital Textile Printing InksDHRUVNo ratings yet
- FAJASDocument891 pagesFAJASCecilia GilNo ratings yet
- Paranoia XP - Gamemaster Screen Booklet - Mandatory Fun Enforcement PackDocument24 pagesParanoia XP - Gamemaster Screen Booklet - Mandatory Fun Enforcement PackStBash100% (3)
- Statistics and Probability Module 3Document3 pagesStatistics and Probability Module 3Eftychia LeegleeNo ratings yet
- Kodak Easyshare Z712 Is Zoom Digital Camera: User'S GuideDocument75 pagesKodak Easyshare Z712 Is Zoom Digital Camera: User'S GuideIronko PepeNo ratings yet