You might also like
- Ralph Baric Statement To The Fact CheckerDocument2 pagesRalph Baric Statement To The Fact CheckerGlennKesslerWP100% (2)
- Plumb's+9th+Edition+Errata+-+PDH+Errata+Landing+Page 4.28.20 PDFDocument3 pagesPlumb's+9th+Edition+Errata+-+PDH+Errata+Landing+Page 4.28.20 PDFMuhammad Zubair BhuttaNo ratings yet
- Dispensing Lab Midterms ReviewerDocument7 pagesDispensing Lab Midterms ReviewerCHARLES RONALD GENATONo ratings yet
- SourceB Ophthalmology Product Catalog 2018 APPROVEDDocument8 pagesSourceB Ophthalmology Product Catalog 2018 APPROVEDMohammad A. BawtagNo ratings yet
- CONSENT FORM Kap Dengue LatestDocument6 pagesCONSENT FORM Kap Dengue Latestfairus_fz821575No ratings yet
- QR ANTIBIOTIC GUIDELINE A3 Size - 210628 - 082213 - 210628 - 082342 - 210628 - 082357-1Document1 pageQR ANTIBIOTIC GUIDELINE A3 Size - 210628 - 082213 - 210628 - 082342 - 210628 - 082357-1Munirah YusoffNo ratings yet
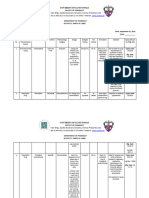
- Rekomendasi Antibiotik Rute Pemberian (Po / Drip/ Bolus) Dosis/ Interval Pemberian Lama Pemberian (Hari) Sumber Referensi KeteranganDocument4 pagesRekomendasi Antibiotik Rute Pemberian (Po / Drip/ Bolus) Dosis/ Interval Pemberian Lama Pemberian (Hari) Sumber Referensi Keterangananon_12953532No ratings yet
- Management of Acne Guidelines Jan 2015Document4 pagesManagement of Acne Guidelines Jan 2015NafiahEmaSuryaniNo ratings yet
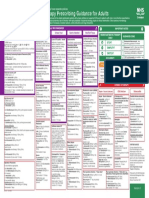
- Empirical Antimicrobial Therapy Prescribing Guidance For AdultsDocument1 pageEmpirical Antimicrobial Therapy Prescribing Guidance For AdultsPsychology TodayNo ratings yet
- Drug Name Classification/ Mechanism of Action Indications Contraindications Side Effects/ Adverse Effects Nursing Responsibilities Generic NameDocument1 pageDrug Name Classification/ Mechanism of Action Indications Contraindications Side Effects/ Adverse Effects Nursing Responsibilities Generic NameRheza AltimoNo ratings yet
- 6 Drug StudyDocument12 pages6 Drug StudyBabylayne PangcatanNo ratings yet
- Medical 3Document2 pagesMedical 3Hanane IssèmNo ratings yet
- ONA Foundation DAILY Outpatient CENSUS (November 2018) Chief Complaint Diagnosis Management DAY 2 - November 6, 2018Document4 pagesONA Foundation DAILY Outpatient CENSUS (November 2018) Chief Complaint Diagnosis Management DAY 2 - November 6, 2018Ray Christoffer GomezNo ratings yet
- Gabavent M 300mg500mcg Tablet View Uses, Side Effects, Price and Substitutes 1mgDocument1 pageGabavent M 300mg500mcg Tablet View Uses, Side Effects, Price and Substitutes 1mgSRINIVAS CHNo ratings yet
- Drug study-FOURTH TWO MEDICAL WARDDocument2 pagesDrug study-FOURTH TWO MEDICAL WARDErryl Justine AdvinculaNo ratings yet
- University of Cebu-Banilad College of NursingDocument4 pagesUniversity of Cebu-Banilad College of NursingMauriceNo ratings yet
- Pediatric Guidelines: Head and Neck Infections - MastoiditisDocument3 pagesPediatric Guidelines: Head and Neck Infections - MastoiditisJr SparkNo ratings yet
- Omeprazol - Drug StudyDocument2 pagesOmeprazol - Drug StudyMae Visperas100% (1)
- Annex To The European Commission Guideline On Excipients in The Labelling and Package Leaflet of Medicinal Products For Human Use' (2019)Document21 pagesAnnex To The European Commission Guideline On Excipients in The Labelling and Package Leaflet of Medicinal Products For Human Use' (2019)janoscribdNo ratings yet
- RCH - Peds Emergency Reference Card - Jan 2013Document2 pagesRCH - Peds Emergency Reference Card - Jan 2013Bob YongNo ratings yet
- Alfuzosin + Dutasteride Alfusin-D Medication Patient InformationDocument21 pagesAlfuzosin + Dutasteride Alfusin-D Medication Patient Informationgarciamaratin54No ratings yet
- DRUG STUDY MetronidazoleDocument4 pagesDRUG STUDY MetronidazoleJake Yvan DizonNo ratings yet
- Opioid Rotation Conversion Learning PackageDocument18 pagesOpioid Rotation Conversion Learning Packagepaul casillasNo ratings yet
- BenadrylDocument4 pagesBenadrylDiogo MaiaNo ratings yet
- Therapeutic Interchange ProgramDocument13 pagesTherapeutic Interchange ProgramSciNo ratings yet
- ParacetamolDocument3 pagesParacetamolgersalia.christiennikkiNo ratings yet
- Drug StudyDocument4 pagesDrug StudyColanag, Ian JohnNo ratings yet
- Recommendation For The Use of Antibiotics For The Treatment of InfectionDocument5 pagesRecommendation For The Use of Antibiotics For The Treatment of InfectionGem BorjaNo ratings yet
- Plumbs 9th Edition Errata PDH Errata Landing Page - 9.23.22Document3 pagesPlumbs 9th Edition Errata PDH Errata Landing Page - 9.23.22nino.bullonNo ratings yet
- 3.3 Medication Histories of Peptic Ulcer Disease: Table 3.3aDocument10 pages3.3 Medication Histories of Peptic Ulcer Disease: Table 3.3ab_rahman2k39603No ratings yet
- DSDSSDDocument10 pagesDSDSSDkrischaniNo ratings yet
- Dsip 2.4 BMX Mouthwash, Nitrofurantoin, OndansetronDocument17 pagesDsip 2.4 BMX Mouthwash, Nitrofurantoin, OndansetronGreatness AgwazeNo ratings yet
- MethimazoleDocument3 pagesMethimazoleRenNo ratings yet
- Section 5 Fastidious/Miscellaneous Gram Negative Bacilli/Cocci/CoccobacilliDocument36 pagesSection 5 Fastidious/Miscellaneous Gram Negative Bacilli/Cocci/CoccobacilliAhmed Goma'aNo ratings yet
- CP ReportDocument2 pagesCP Reportrebecca babiryeNo ratings yet
- CASE StudyDocument7 pagesCASE Studyخالد الغامديNo ratings yet
- Jurnal 2 EbcrDocument9 pagesJurnal 2 EbcrhermanfirdausNo ratings yet
- Car Bop LatinDocument2 pagesCar Bop LatinPerly PeterNo ratings yet
- Inserto Surestep VasoDocument11 pagesInserto Surestep Vasojorge.sebastian.velasquez0509No ratings yet
- SHC SurgProphylaxisGuidelinesDocument6 pagesSHC SurgProphylaxisGuidelinesDr shehwar100% (1)
- Pi Is 0168827817300156Document2 pagesPi Is 0168827817300156kookyin100% (1)
- Drug StudyDocument19 pagesDrug StudyKimberly Subade MandilagNo ratings yet
- Activity 3 Parts of LabelDocument5 pagesActivity 3 Parts of LabelLiz AbennaNo ratings yet
- 1 Comparative Pharmacokinetics of Oral Ibuprofen FormulationsDocument11 pages1 Comparative Pharmacokinetics of Oral Ibuprofen FormulationsNishad PrabhuNo ratings yet
- AdrenalineDocument11 pagesAdrenalineAli AkhtarNo ratings yet
- ONA Foundation DAILY Outpatient CENSUS (November 2018) Chief Complaint Diagnosis Management DAY 6 - November 21, 2018Document4 pagesONA Foundation DAILY Outpatient CENSUS (November 2018) Chief Complaint Diagnosis Management DAY 6 - November 21, 2018Ray Christoffer GomezNo ratings yet
- PSMMC IV GUIDE LINES - Copy6Document18 pagesPSMMC IV GUIDE LINES - Copy6NhcpsNo ratings yet
- DRUG StudyDocument43 pagesDRUG StudyNathalie Faith CotengNo ratings yet
- Laboratory, Diagnostics Procedures & ConsultationDocument5 pagesLaboratory, Diagnostics Procedures & Consultationeva cortezNo ratings yet
- Para Terminar de Llenar KPSDocument8 pagesPara Terminar de Llenar KPSAli Florez PedrazaNo ratings yet
- CheatDocument6 pagesCheatJona Rhose GadotNo ratings yet
- AmoxicillinDocument2 pagesAmoxicillinKasandra Dawn Moquia BerisoNo ratings yet
- Alb 440 - Xsys00001 - en - Ru - G1Document4 pagesAlb 440 - Xsys00001 - en - Ru - G1Matibar RahmanNo ratings yet
- Expert Advice For Today's Ob/Gyn: ObstetricsDocument66 pagesExpert Advice For Today's Ob/Gyn: Obstetricsjavierv44No ratings yet
- Tranexamic Acid Drug StudyDocument3 pagesTranexamic Acid Drug Studyswitchlers anneNo ratings yet
- Recommendations For Diagnosis and Treatment of Lyme BorreliosisDocument1 pageRecommendations For Diagnosis and Treatment of Lyme BorreliosisLauge BrimgiestNo ratings yet
- Antibiotics Lock TherapyDocument5 pagesAntibiotics Lock TherapyMei Fong Sohbana100% (1)
- NCP and Drug Study Form APDocument6 pagesNCP and Drug Study Form APRed EslaoNo ratings yet
- Ambulatory Care MedicineDocument26 pagesAmbulatory Care MedicineJustineValJadeLacabaNo ratings yet
- Obat-Obatan Bumil Dan Busui Berdasarkan Kategori Fda, Adec, MPRDocument2 pagesObat-Obatan Bumil Dan Busui Berdasarkan Kategori Fda, Adec, MPRUGD VIDYANNo ratings yet
- PHARCHEM2 List AntimicrobialsDocument14 pagesPHARCHEM2 List AntimicrobialsLA BriguelaNo ratings yet
- MFP Volume17No2Document135 pagesMFP Volume17No2Shazwani KKTSNo ratings yet
- The Short Child Review Article DR Azriyanti 2021Document10 pagesThe Short Child Review Article DR Azriyanti 2021tee qarafiNo ratings yet
- v17n2 Oa Prevalence and Factors Associated With PsychologicalDocument10 pagesv17n2 Oa Prevalence and Factors Associated With PsychologicalShazwani KKTSNo ratings yet
- v15n3 Original Article 4Document8 pagesv15n3 Original Article 4Shazwani KKTSNo ratings yet
- Major Depressive DisorderDocument5 pagesMajor Depressive DisorderShazwani KKTSNo ratings yet
- Depression Primary Care Part2Document4 pagesDepression Primary Care Part2Shazwani KKTSNo ratings yet
- Antibiotic Susceptibility TestingDocument46 pagesAntibiotic Susceptibility Testingditta antNo ratings yet
- BMS Iddt 2020 41Document8 pagesBMS Iddt 2020 41Guneyden GuneydenNo ratings yet
- Mc. ConcayDocument5 pagesMc. Concaypuspita dwikartikasariNo ratings yet
- HIV Vaccine Basics May 2019Document21 pagesHIV Vaccine Basics May 2019Priyo SadewoNo ratings yet
- Types of Infectious DiseasesDocument11 pagesTypes of Infectious DiseasesmaricelNo ratings yet
- Culture MediaDocument5 pagesCulture MediaNuella AbrigoNo ratings yet
- Vaginal SecretionsDocument52 pagesVaginal SecretionsKim BuguinaNo ratings yet
- Neisseria, MoraxellaDocument33 pagesNeisseria, MoraxellaShuler0071No ratings yet
- Emailing DOC-20221210-WA0012.Document1 pageEmailing DOC-20221210-WA0012.JAHIR HASANNo ratings yet
- Bacterial Growth and Culture MediaDocument26 pagesBacterial Growth and Culture MediaMuhammad HuzaifaNo ratings yet
- Virology LectureDocument16 pagesVirology LectureJuan UmiwasNo ratings yet
- Difference of Broad Spectrum & Narrow Spectrum AntibioticsDocument36 pagesDifference of Broad Spectrum & Narrow Spectrum AntibioticsAFTAB H. ABBASINo ratings yet
- Yellow FeverDocument11 pagesYellow FeverPriyanka TalukdarNo ratings yet
- Viruses: RNA Virus Reverse Genetics and Vaccine DesignDocument20 pagesViruses: RNA Virus Reverse Genetics and Vaccine Designfragariavesca100% (1)
- TonsillitisDocument21 pagesTonsillitisWael ShamyNo ratings yet
- ShigellaDocument23 pagesShigellaAayush AdhikariNo ratings yet
- ProtozoanDocument3 pagesProtozoanPatrice Bianca SarmientoNo ratings yet
- A Hefty Volume: Immunology and Molecular Biology of Parasitic InfectionsDocument1 pageA Hefty Volume: Immunology and Molecular Biology of Parasitic InfectionsRichard TamreNo ratings yet
- Zika Virus FactsheetDocument2 pagesZika Virus Factsheetfriska_arianiNo ratings yet
- Answering Crucial Questions About Sars-CoV-2Document57 pagesAnswering Crucial Questions About Sars-CoV-2Sarah WestallNo ratings yet
- Dengue VirusDocument2 pagesDengue VirusImee Claire PacisNo ratings yet
- Characteristics of Monera: BacteriaDocument5 pagesCharacteristics of Monera: BacteriaAkshitaa PandeyNo ratings yet
- Uji Efektivitas Ekstrak Etanol Kulit Buah Naga Merah (Hylocereus Polyrhizus) Terhadap StaphylococcusDocument5 pagesUji Efektivitas Ekstrak Etanol Kulit Buah Naga Merah (Hylocereus Polyrhizus) Terhadap StaphylococcusUten MokiNo ratings yet
- BMS533 Lab Practical 1Document13 pagesBMS533 Lab Practical 1Nur NazirahNo ratings yet
- Microbiology NotesDocument14 pagesMicrobiology Notesapi-264004571No ratings yet
- Virus ShapesDocument2 pagesVirus Shapessarath chandNo ratings yet
- Benefits and Limitations of Maldi Tof Mass Spectrometry For The Identification of Microorganisms Journal of Infectiology 1 1142Document5 pagesBenefits and Limitations of Maldi Tof Mass Spectrometry For The Identification of Microorganisms Journal of Infectiology 1 1142ntnquynhproNo ratings yet
- LKJHHDocument5 pagesLKJHHVishnu SharmaNo ratings yet