You might also like
- Streptococcus Pneumoniae Haemophilus Influenzae: Click HereDocument3 pagesStreptococcus Pneumoniae Haemophilus Influenzae: Click HereSiti Hidayatul FitriNo ratings yet
- Any Up-Dates Are To Be Completed in Different Color Ink. The Student Is Expected To Document All Meds The Client Is Currently ReceivingDocument1 pageAny Up-Dates Are To Be Completed in Different Color Ink. The Student Is Expected To Document All Meds The Client Is Currently Receivinggeorgeloto12No ratings yet
- Medication PicuDocument2 pagesMedication PicuSweety KurnNo ratings yet
- Medical TherapyDocument6 pagesMedical Therapyvinay reddyNo ratings yet
- AmikinDocument2 pagesAmikinLIEZEL GRACE VELAYONo ratings yet
- HSB Pneumonia Antibiotic AlgorithmDocument4 pagesHSB Pneumonia Antibiotic AlgorithmDr.Senthil KumarNo ratings yet
- Salazar Medsurg Drug StudyDocument2 pagesSalazar Medsurg Drug StudyAlyssa Marie PepitoNo ratings yet
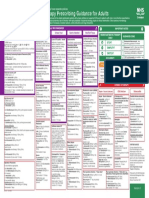
- Empirical Antimicrobial Therapy Prescribing Guidance For AdultsDocument1 pageEmpirical Antimicrobial Therapy Prescribing Guidance For AdultsPsychology TodayNo ratings yet
- Medications DSDocument2 pagesMedications DSSweety KurnNo ratings yet
- Chapter 2 - Antimicrobial Therapy For Head and Neck InfectionDocument13 pagesChapter 2 - Antimicrobial Therapy For Head and Neck InfectionMario CastanedaNo ratings yet
- Drug study-FOURTH TWO MEDICAL WARDDocument2 pagesDrug study-FOURTH TWO MEDICAL WARDErryl Justine AdvinculaNo ratings yet
- IMG EmpAposterDocument1 pageIMG EmpAposterChiu LeoNo ratings yet
- Amoxicillin (Amoxycillin) : PresentationDocument4 pagesAmoxicillin (Amoxycillin) : PresentationRavikiran SuryanarayanamurthyNo ratings yet
- COVID Clinical Management 14012022Document1 pageCOVID Clinical Management 14012022Naina DesaiNo ratings yet
- COVID Management 17th January 2022 DR Suvrankar Datta AIIMSDocument1 pageCOVID Management 17th January 2022 DR Suvrankar Datta AIIMSWhiteNo ratings yet
- Drug Study SalbutamolDocument2 pagesDrug Study Salbutamolliza sian100% (2)
- Drug Study of TBDocument7 pagesDrug Study of TBMarc AntonioNo ratings yet
- Salazar Medsurg Drug StudyDocument26 pagesSalazar Medsurg Drug StudyAlyssa Marie PepitoNo ratings yet
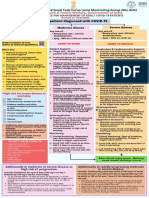
- Adult Patient Diagnosed With COVID-19: Ministry of Health & Family Welfare, Government of IndiaDocument1 pageAdult Patient Diagnosed With COVID-19: Ministry of Health & Family Welfare, Government of Indiapramodbankhele3845No ratings yet
- Midwifery Pharmacology-19Document1 pageMidwifery Pharmacology-19georgeloto12No ratings yet
- Drug Study AzithromycinDocument2 pagesDrug Study AzithromycinYamete KudasaiNo ratings yet
- Drug Study23Document2 pagesDrug Study23Joh Acedo BantingNo ratings yet
- Zinacef: Brand Name: Generic Name: Drug ClassificationDocument2 pagesZinacef: Brand Name: Generic Name: Drug ClassificationChristine Pialan SalimbagatNo ratings yet
- Orthopaedic Infection in Adults UHL GuidelineDocument10 pagesOrthopaedic Infection in Adults UHL GuidelineFadlu ManafNo ratings yet
- FluticasoneDocument4 pagesFluticasonevanNo ratings yet
- Drug Study AmpicillinDocument3 pagesDrug Study AmpicillinChristine NocomuraNo ratings yet
- Cabasis Drug StudyDocument3 pagesCabasis Drug StudyNick James CabasisNo ratings yet
- Adiel Joy P. Calsa Drug Study March 9, 2022Document5 pagesAdiel Joy P. Calsa Drug Study March 9, 2022Adiel CalsaNo ratings yet
- SHC Heme Onc Antimicrobial ProphylaxisDocument4 pagesSHC Heme Onc Antimicrobial ProphylaxisTala MahmoudNo ratings yet
- Recommendation For The Use of Antibiotics For The Treatment of InfectionDocument5 pagesRecommendation For The Use of Antibiotics For The Treatment of InfectionGem BorjaNo ratings yet
- Empirical Prescribing Chart GlasgowDocument1 pageEmpirical Prescribing Chart GlasgowHariharan Narendran75% (4)
- Any Up-Dates Are To Be Completed in Different Color Ink. The Student Is Expected To Document All Meds The Client Is Currently ReceivingDocument1 pageAny Up-Dates Are To Be Completed in Different Color Ink. The Student Is Expected To Document All Meds The Client Is Currently Receivinggeorgeloto12No ratings yet
- ImmunizationDocument20 pagesImmunizationsarguss14100% (2)
- 5 Cefuroxime Drug StudyDocument4 pages5 Cefuroxime Drug Studyshadow gonzalezNo ratings yet
- Drug Study-PharmaDocument12 pagesDrug Study-PharmaMichael TokongNo ratings yet
- Acute Otitis Media (Aom) (Children) : Symptoms and DiagnosisDocument2 pagesAcute Otitis Media (Aom) (Children) : Symptoms and DiagnosisRoxana SurliuNo ratings yet
- Antibiotic Choices For Treatment of MRSADocument16 pagesAntibiotic Choices For Treatment of MRSAfarmasi_hm100% (2)
- UAW Respiratory Antimicrobial Pharm Guide MedstuDocument19 pagesUAW Respiratory Antimicrobial Pharm Guide MedstuNabeel ShahzadNo ratings yet
- Medicine RotatationbookletDocument20 pagesMedicine RotatationbookletJanelle JosephsNo ratings yet
- Antibiotic Hospital ManDocument1 pageAntibiotic Hospital Manarshiya.manasekiNo ratings yet
- Prophylaxis Action: Tetanus: Injection: 5 To 10 LF Units ofDocument10 pagesProphylaxis Action: Tetanus: Injection: 5 To 10 LF Units ofElle RosalesNo ratings yet
- Antimycobacterial Drugs: Camille E. Beauduy, Pharmd, & Lisa G. Winston, MDDocument17 pagesAntimycobacterial Drugs: Camille E. Beauduy, Pharmd, & Lisa G. Winston, MDRegine Coeli Menta LansanganNo ratings yet
- Drug Study: Sympathomime Tic, Beta2-Selective Adrenergic Agonist, Bronchodilator, AntiasthmaticDocument3 pagesDrug Study: Sympathomime Tic, Beta2-Selective Adrenergic Agonist, Bronchodilator, AntiasthmaticJichutreasure100% (1)
- 6 Metronidazole Drug StudyDocument4 pages6 Metronidazole Drug Studyshadow gonzalezNo ratings yet
- Drud Study For DutyDocument9 pagesDrud Study For DutyAnonymous AlphaNo ratings yet
- COVID19 Management Algorithm 22042021 v1Document1 pageCOVID19 Management Algorithm 22042021 v1shivani shindeNo ratings yet
- DUG AntifungalDocument26 pagesDUG AntifungalAudrey JauwNo ratings yet
- FluticasoneDocument3 pagesFluticasoneAmberNo ratings yet
- Drug Study (Covid Case)Document5 pagesDrug Study (Covid Case)YessaminNo ratings yet
- RCH - Peds Emergency Reference Card - Jan 2013Document2 pagesRCH - Peds Emergency Reference Card - Jan 2013Bob YongNo ratings yet
- PHARMAfdDocument7 pagesPHARMAfdJobelle AcenaNo ratings yet
- PDF Surgical Prophylaxis Poster Dec 2021Document1 pagePDF Surgical Prophylaxis Poster Dec 2021Midhun KishorNo ratings yet
- TASH Empirical Antibiotic Treatment Guidelines - 2018 Hospital and Ventilator Associated Pneumonia (HAP and VAP)Document2 pagesTASH Empirical Antibiotic Treatment Guidelines - 2018 Hospital and Ventilator Associated Pneumonia (HAP and VAP)ጉራማይሌ TubeNo ratings yet
- PHARMA LE1 Asthma & Cough Cram SheetDocument1 pagePHARMA LE1 Asthma & Cough Cram SheetMarjorie MonesNo ratings yet
- NDS BubanDocument3 pagesNDS BubanJennica BubanNo ratings yet
- Antibiotic (Bacteriostatic) DrugsDocument15 pagesAntibiotic (Bacteriostatic) DrugsVictor LeeNo ratings yet
- Drug Study - OmeprazoleDocument5 pagesDrug Study - OmeprazoleRonel ResurricionNo ratings yet
- Parasitic WormsDocument4 pagesParasitic WormsEricNo ratings yet
- Adult Infectious Disease Bulletpoints HandbookFrom EverandAdult Infectious Disease Bulletpoints HandbookRating: 4.5 out of 5 stars4.5/5 (9)
- Mouthwash From Ethanol Leaf Extract Of: Jurnal Ilmiah Farmako BahariDocument11 pagesMouthwash From Ethanol Leaf Extract Of: Jurnal Ilmiah Farmako BahariJr SparkNo ratings yet
- BEYOND THE GOD SPOT Transcendence and The Brain: Way February 2014Document8 pagesBEYOND THE GOD SPOT Transcendence and The Brain: Way February 2014Jr SparkNo ratings yet
- Religions: God Spots in The Brain: Nine Categories of Unasked, Unanswered QuestionsDocument14 pagesReligions: God Spots in The Brain: Nine Categories of Unasked, Unanswered QuestionsJr SparkNo ratings yet
- Uji Daya Hambat Larutan Daun Sukun (Artocarpus Altilis) TERHADAP PERTUMBUHAN BAKTERIDocument10 pagesUji Daya Hambat Larutan Daun Sukun (Artocarpus Altilis) TERHADAP PERTUMBUHAN BAKTERIJr SparkNo ratings yet
- ID Hubungan Kinerja Otak Dengan SpiritualitDocument8 pagesID Hubungan Kinerja Otak Dengan SpiritualitJr SparkNo ratings yet
- GCS Assessment Aid English PDFDocument1 pageGCS Assessment Aid English PDFSila OntitaNo ratings yet
- March 2013 Neurotheology of The SoulDocument6 pagesMarch 2013 Neurotheology of The SoulHugo Andres Rubiano CharryNo ratings yet
- Fingelkurts Is Our Brain Hardwired To Produce or Perseive GodDocument54 pagesFingelkurts Is Our Brain Hardwired To Produce or Perseive GodJr SparkNo ratings yet
- The Brain and The Soul: Joseph LeeDocument14 pagesThe Brain and The Soul: Joseph LeeJr SparkNo ratings yet
- 61 - 5409 - e (C) - PF1 (M) - F (P) - PF1 (P) - Pfa (NC) - Olf - PF1 (Puh) - 1Document5 pages61 - 5409 - e (C) - PF1 (M) - F (P) - PF1 (P) - Pfa (NC) - Olf - PF1 (Puh) - 1Jr SparkNo ratings yet
- PSCF9 05jeevesDocument17 pagesPSCF9 05jeevesJr SparkNo ratings yet
- Shifting Paradigm: From Intellectual Quotient, Emotional Quotient, and Spiritual Quotient Toward Ruhani Quotient in Ruhiology PerspectivesDocument24 pagesShifting Paradigm: From Intellectual Quotient, Emotional Quotient, and Spiritual Quotient Toward Ruhani Quotient in Ruhiology PerspectivesJr SparkNo ratings yet
- Afterword: Belief in Science? On The Neuroscience of ReligionDocument1 pageAfterword: Belief in Science? On The Neuroscience of ReligionJr SparkNo ratings yet
- Neurotheology:: Confirming The Existence of A Naturally Mystical MindDocument10 pagesNeurotheology:: Confirming The Existence of A Naturally Mystical MindJr SparkNo ratings yet
- Religions: Is An Integrative Model of Neurotheology Possible?Document11 pagesReligions: Is An Integrative Model of Neurotheology Possible?Jr SparkNo ratings yet
- 366-Article Text-923-1-10-20210507Document10 pages366-Article Text-923-1-10-20210507Jr SparkNo ratings yet
- March 2013 Neurotheology of The SoulDocument6 pagesMarch 2013 Neurotheology of The SoulHugo Andres Rubiano CharryNo ratings yet
- How Theology Looks at NeurotheologyDocument16 pagesHow Theology Looks at NeurotheologyJr SparkNo ratings yet
- Neuroscience of SpiritualityDocument7 pagesNeuroscience of SpiritualityAndrás SzabóNo ratings yet
- The God Spot 2013Document5 pagesThe God Spot 2013Jr SparkNo ratings yet
- The God Spot 2013Document5 pagesThe God Spot 2013Jr SparkNo ratings yet
- Spirituality Special Interest Group Publications Simon Dein Recent Advances in NeurotheologyDocument3 pagesSpirituality Special Interest Group Publications Simon Dein Recent Advances in NeurotheologyJr SparkNo ratings yet
- 5C 5CFiles5CAuthArts5C1018 PDFDocument6 pages5C 5CFiles5CAuthArts5C1018 PDFJr SparkNo ratings yet
- Oculocardiac Re Ex: Know-How?: Jaichandran V VDocument7 pagesOculocardiac Re Ex: Know-How?: Jaichandran V VJr SparkNo ratings yet
- Prinsip - Prinsip Dasar Manajemen Anestesi Pada Operasi MataDocument38 pagesPrinsip - Prinsip Dasar Manajemen Anestesi Pada Operasi MataJr SparkNo ratings yet
- 10.1177 0300060520945158Document10 pages10.1177 0300060520945158Jr SparkNo ratings yet
- Leukemia Myeloproliferation, Myelodysplasia: Lita Septina Peyakit Dalam FK UMSUDocument47 pagesLeukemia Myeloproliferation, Myelodysplasia: Lita Septina Peyakit Dalam FK UMSUJr SparkNo ratings yet
- Acute Myeloid Leukemia Early Detection, Diagnosis, and TypesDocument22 pagesAcute Myeloid Leukemia Early Detection, Diagnosis, and TypesMellan Apriiaty SimbolonNo ratings yet
- Acute Myeloid Leukemia Early Detection, Diagnosis, and TypesDocument22 pagesAcute Myeloid Leukemia Early Detection, Diagnosis, and TypesMellan Apriiaty SimbolonNo ratings yet
- Mastoiditis: February 2016Document15 pagesMastoiditis: February 2016Bram wijayaNo ratings yet
- 11 16Document128 pages11 16WoodsNo ratings yet
- Staff Training Slideshow 4 - HygieneDocument21 pagesStaff Training Slideshow 4 - HygieneChef M.husainNo ratings yet
- Kaya Kalp House Keeping StandardsDocument131 pagesKaya Kalp House Keeping StandardsAnuragMishraNo ratings yet
- Bovine Respiratory DiseaseDocument4 pagesBovine Respiratory DiseaseDamir BrankovicNo ratings yet
- Neurosesnsory EYESDocument92 pagesNeurosesnsory EYESMae MarcojosNo ratings yet
- LeaP-Health-G6-Week 1-Q3Document4 pagesLeaP-Health-G6-Week 1-Q3Dyanne de JesusNo ratings yet
- Drug Study Ampicillin, CelestamineDocument5 pagesDrug Study Ampicillin, CelestamineLLan Kristine Lazarito100% (1)
- Module 3 AsepsisDocument14 pagesModule 3 Asepsisjhoyjhoy779No ratings yet
- Rheumatology SheetDocument54 pagesRheumatology Sheetnachwaallam50% (2)
- Using Transition Words CorrectlyDocument4 pagesUsing Transition Words CorrectlyxhahaniNo ratings yet
- Needle Stick InjuryDocument5 pagesNeedle Stick Injurypsc anandNo ratings yet
- Binda BIO3219 Lab5Document12 pagesBinda BIO3219 Lab5Ronaldo BindaNo ratings yet
- Basics of Chest X-RayDocument44 pagesBasics of Chest X-RayMelissa Aina Mohd YusofNo ratings yet
- Satuan Acara Penyuluhan Penanganan Dan Pencegahan Penyakit PanuDocument8 pagesSatuan Acara Penyuluhan Penanganan Dan Pencegahan Penyakit PanuRamayanaNo ratings yet
- Gallstone DiseaseDocument14 pagesGallstone DiseasePrincess Meinny JeanNo ratings yet
- Responses To Exposed Variant Surface T-Cell-Independent and T-Cell-Dependent B-CellDocument7 pagesResponses To Exposed Variant Surface T-Cell-Independent and T-Cell-Dependent B-CellNicoli Arthur Balita BorromeoNo ratings yet
- C+F-Spirometra İnfection in Cats and DogsDocument5 pagesC+F-Spirometra İnfection in Cats and Dogstaner_soysurenNo ratings yet
- Rapid Revisin SurgeryDocument5 pagesRapid Revisin SurgeryMOHAMMED IQBALNo ratings yet
- Communicable Disease ReviewDocument7 pagesCommunicable Disease Reviewjudith dela cruzNo ratings yet
- Crops Diseases List (Updated)Document23 pagesCrops Diseases List (Updated)Amit KishoreNo ratings yet
- TheRawFoodDietandYourCompromisedTeeth PDFDocument117 pagesTheRawFoodDietandYourCompromisedTeeth PDFkiska888No ratings yet
- Immunization Schedule 27-07-2016Document2 pagesImmunization Schedule 27-07-2016SandraniNo ratings yet
- Mycology SOP 2nd Ed 2019Document144 pagesMycology SOP 2nd Ed 2019Deepak Muralidhara NadigNo ratings yet
- Approval Status of New Drug During 1971-1981Document44 pagesApproval Status of New Drug During 1971-1981NitinPrachiJainNo ratings yet
- Wood's Lamp - IjdvlDocument5 pagesWood's Lamp - IjdvlKunal PaulNo ratings yet
- Fish Diseases and ParasitesDocument11 pagesFish Diseases and ParasitesRizalene Agustin100% (2)
- Unit 1 The Microbial World and YouDocument29 pagesUnit 1 The Microbial World and YouGebriel Igdon TomarongNo ratings yet
- Waterborne Diseases 1Document26 pagesWaterborne Diseases 1Dalia Talaat WehediNo ratings yet
- Rabies Virus: RhabdovirusesDocument18 pagesRabies Virus: RhabdovirusesHaydas ChannelNo ratings yet
- WEEK 9 Antimicrobial ChemotherapyDocument25 pagesWEEK 9 Antimicrobial Chemotherapyotaibynaif100% (2)