You might also like
- Pharmacodynamics of Antimicrobial Agents: Time-Dependent vs. Concentration-Dependent KillingDocument4 pagesPharmacodynamics of Antimicrobial Agents: Time-Dependent vs. Concentration-Dependent KillingMaddy AlbuletNo ratings yet
- SubtitleDocument2 pagesSubtitleTawfiq BA ABBADNo ratings yet
- Antibiotic Selection GuideDocument43 pagesAntibiotic Selection GuideMuchlissatus Lisa MedicalbookNo ratings yet
- Pharmacokineticsand Pharmacodynamics: Optimalantimicrobial Therapyinthe IntensivecareunitDocument18 pagesPharmacokineticsand Pharmacodynamics: Optimalantimicrobial Therapyinthe IntensivecareunitSambit DashNo ratings yet
- Pathogens: The Minimum Inhibitory Concentration of Antibiotics: Methods, Interpretation, Clinical RelevanceDocument21 pagesPathogens: The Minimum Inhibitory Concentration of Antibiotics: Methods, Interpretation, Clinical RelevanceFirdaNo ratings yet
- Principles To ChemotherapyDocument32 pagesPrinciples To ChemotherapyWezzyNo ratings yet
- Clinical Pharmacy of AntibioticsDocument53 pagesClinical Pharmacy of AntibioticsEkanita DesianiNo ratings yet
- Bug and DrugDocument12 pagesBug and DrugJair Alexander Quintero PanucoNo ratings yet
- Tipuri de Efect PKDocument11 pagesTipuri de Efect PKLaiosAndreaNo ratings yet
- Bacteriology: Principles of Antimicrobial ActionDocument35 pagesBacteriology: Principles of Antimicrobial ActionggemalynNo ratings yet
- Antimicrobial Fundamental ConceptsDocument8 pagesAntimicrobial Fundamental ConceptsFarmaIndasurNo ratings yet
- Introduction To Antimicrobial DrugsDocument36 pagesIntroduction To Antimicrobial Drugstsegaab yosephNo ratings yet
- Bacterial Pathogenesis and ChemotherapyDocument3 pagesBacterial Pathogenesis and ChemotherapySubrata KunduNo ratings yet
- Farmacolgia para IntensivistasDocument14 pagesFarmacolgia para IntensivistasJesus RivasNo ratings yet
- Pharmacokinetics and Pharmacodynamics of Antibacterial Agents PDFDocument29 pagesPharmacokinetics and Pharmacodynamics of Antibacterial Agents PDFarmitadewiNo ratings yet
- 112antimicrobial Suscetibiliy Testing POSDocument4 pages112antimicrobial Suscetibiliy Testing POSkane.20602No ratings yet
- The Rational Use Of: AntibioticsDocument28 pagesThe Rational Use Of: AntibioticsdanielaNo ratings yet
- 01 Dr. Khin Hnin PwintDocument7 pages01 Dr. Khin Hnin PwintHein Myat HtutNo ratings yet
- AntibioticsDocument49 pagesAntibioticsShriefElghazalyNo ratings yet
- Minireview: Issues in Pharmacokinetics and Pharmacodynamics of Anti-Infective Agents: Kill Curves Versus MICDocument9 pagesMinireview: Issues in Pharmacokinetics and Pharmacodynamics of Anti-Infective Agents: Kill Curves Versus MICvn_ny84bio021666No ratings yet
- Revisiting Beta-Lactams - PK/PD Improves Dosing of Old AntibioticsDocument7 pagesRevisiting Beta-Lactams - PK/PD Improves Dosing of Old AntibioticsgabijurubitaNo ratings yet
- Antimicrobial Susceptibility Testing - Primer For CliniciansDocument20 pagesAntimicrobial Susceptibility Testing - Primer For Cliniciansdipzhit100% (1)
- Antimicrobial Pharmacokinetic and Pharmacodynamics (Andes) ChapterDocument22 pagesAntimicrobial Pharmacokinetic and Pharmacodynamics (Andes) Chapterkhangsiean89No ratings yet
- Antimicrobial Drugs: Introduction To Antimicrobial Drugs. (N.D.) - WWW - Cyto.purdue - EduDocument2 pagesAntimicrobial Drugs: Introduction To Antimicrobial Drugs. (N.D.) - WWW - Cyto.purdue - EduAdeniyi AdebanjiNo ratings yet
- PK PD Beta LactameDocument6 pagesPK PD Beta Lactamebaitur rohmahNo ratings yet
- Antimicrobial Therapy in Veterinary MedicineFrom EverandAntimicrobial Therapy in Veterinary MedicineSteeve GiguèreRating: 4 out of 5 stars4/5 (1)
- Lab Report Antimicrobial Susceptibility Testing MethodsDocument19 pagesLab Report Antimicrobial Susceptibility Testing MethodsAlyaa Athira100% (1)
- Reviews: Optimizing Antimicrobial Use: Challenges, Advances and OpportunitiesDocument12 pagesReviews: Optimizing Antimicrobial Use: Challenges, Advances and Opportunitiespoiu09092No ratings yet
- N-LEC5 - Chemotherapeutic Agents (General Considerations)Document33 pagesN-LEC5 - Chemotherapeutic Agents (General Considerations)geng gengNo ratings yet
- Anti - Infective TherapyDocument32 pagesAnti - Infective TherapyChaii De GuzmanNo ratings yet
- Principles of Antibiotic Formulary Selection For P&T Committees 1Document3 pagesPrinciples of Antibiotic Formulary Selection For P&T Committees 1madengNo ratings yet
- Antibiotic Susceptibility Testing: A Review On Current PracticesDocument8 pagesAntibiotic Susceptibility Testing: A Review On Current PracticesAndriano Arie WibowoNo ratings yet
- Day 2 General Microbiology 12-1-2021Document150 pagesDay 2 General Microbiology 12-1-2021ShriefElghazalyNo ratings yet
- Pea 2009Document13 pagesPea 2009Anh Khoa Đỗ ĐắcNo ratings yet
- Bayer 3rd Proc'99 - BOOTHE2Document8 pagesBayer 3rd Proc'99 - BOOTHE2sergioNo ratings yet
- Link Between MIC and Antimicrobial TherapyDocument8 pagesLink Between MIC and Antimicrobial TherapySahar WaqarNo ratings yet
- Pharmacology of Drug Resistance: 1 2 Resistance Defi Ned by Breakpoint: Good Clinical Response For "Sensitive"Document2 pagesPharmacology of Drug Resistance: 1 2 Resistance Defi Ned by Breakpoint: Good Clinical Response For "Sensitive"niarsari apNo ratings yet
- Barrera Hematoencefaolica y Farmacocinetica Atb SNC 2020Document37 pagesBarrera Hematoencefaolica y Farmacocinetica Atb SNC 2020Ru MNo ratings yet
- Azanza 2020 PharmacodynamicDocument3 pagesAzanza 2020 PharmacodynamicCarlos Espinoza CobeñasNo ratings yet
- PROA Net 2019 MOD 3 Texto Explicativo SpanishDocument7 pagesPROA Net 2019 MOD 3 Texto Explicativo SpanishLili VargasNo ratings yet
- Agus AntibioticDocument78 pagesAgus AntibioticagusNo ratings yet
- Journal Pcbi 1001043Document8 pagesJournal Pcbi 1001043kushalshaNo ratings yet
- Antobiotics I NotesDocument11 pagesAntobiotics I NotesBayan AlsaadiNo ratings yet
- MBR 2019 - Pharmacology HandoutsDocument125 pagesMBR 2019 - Pharmacology HandoutsRgm UyNo ratings yet
- Drug CombinationsDocument15 pagesDrug CombinationsntnquynhproNo ratings yet
- Antibiotic Pharmacokinetic MonitoringDocument5 pagesAntibiotic Pharmacokinetic MonitoringlucialNo ratings yet
- PK PDDocument6 pagesPK PDbaitur rohmahNo ratings yet
- Antimicrobial Chemotherapy, DPA 200-2Document26 pagesAntimicrobial Chemotherapy, DPA 200-2Yeboah Kukudabi AsiamahNo ratings yet
- 10.1515 - CCLM 2022 1072Document7 pages10.1515 - CCLM 2022 1072ENFERMERIA EMERGENCIANo ratings yet
- Darmansjah AntibioticDocument6 pagesDarmansjah AntibioticArrumNo ratings yet
- Antibiotics in Periodental TreatmentDocument29 pagesAntibiotics in Periodental TreatmentJana AliNo ratings yet
- Bactericida X BacteriostaticoDocument7 pagesBactericida X BacteriostaticoMunir BazziNo ratings yet
- Lecture 1Document17 pagesLecture 1mheni4979No ratings yet
- Fvets 09 8604726Document10 pagesFvets 09 8604726drnguyenbvtkNo ratings yet
- Antibiotics: Rodel L. Saludares Mario S. Abendanio Hazel M. Dela Cruz Lea Diane Dela Cruz Jicka TagubaDocument51 pagesAntibiotics: Rodel L. Saludares Mario S. Abendanio Hazel M. Dela Cruz Lea Diane Dela Cruz Jicka TagubaVer Garcera TalosigNo ratings yet
- Universitas Sumatera Utara: School of MedicineDocument60 pagesUniversitas Sumatera Utara: School of MedicineedelinNo ratings yet
- Applying Pharmacokinetic/Pharmacodynamic Principles in Critically Ill Patients: Optimizing Ef Ficacy and Reducing Resistance DevelopmentDocument18 pagesApplying Pharmacokinetic/Pharmacodynamic Principles in Critically Ill Patients: Optimizing Ef Ficacy and Reducing Resistance DevelopmentValentina Lcpc CajaleonNo ratings yet
- Microbiological AssaysDocument34 pagesMicrobiological Assayspradeepbawane60% (5)
- When Antibiotic Treatment FailsDocument3 pagesWhen Antibiotic Treatment FailsThai Che100% (1)
- Surviving Sepsis Campaign 2021Document28 pagesSurviving Sepsis Campaign 2021Hanny Melati HarahapNo ratings yet
- Surgical Site Infection - Prevention - DynaMedDocument122 pagesSurgical Site Infection - Prevention - DynaMedYorvi hendersson Ilasaca gaonaNo ratings yet
- Lectura Critica de Un CC - MURADDocument4 pagesLectura Critica de Un CC - MURADYorvi hendersson Ilasaca gaonaNo ratings yet
- MX Resist Gram+Document8 pagesMX Resist Gram+Yorvi hendersson Ilasaca gaonaNo ratings yet
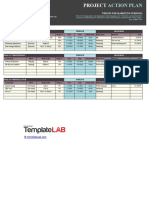
- Claudia Warren: Project ManagerDocument2 pagesClaudia Warren: Project ManagerYorvi hendersson Ilasaca gaonaNo ratings yet
- Med1 Mukkamala ShreyaDocument6 pagesMed1 Mukkamala ShreyaCharlotte YeoNo ratings yet
- Biomarkers-A General ReviewDocument17 pagesBiomarkers-A General ReviewKevin FossNo ratings yet
- Chitosan Nanoparticles PHD ThesisDocument6 pagesChitosan Nanoparticles PHD Thesisfjgmmmew100% (2)
- 559 FullDocument12 pages559 FullAmatystNo ratings yet
- Nephrotic SyndromeDocument10 pagesNephrotic SyndromeElaf SherzadNo ratings yet
- Botanical Pharmacognosy of AndrographisDocument4 pagesBotanical Pharmacognosy of AndrographisNongton DeBitNo ratings yet
- Pericardiocentesis: Why Is This Procedure Done?Document3 pagesPericardiocentesis: Why Is This Procedure Done?HannaNo ratings yet
- Index: General Notices (1) Apply To All Monographs and Other TextsDocument36 pagesIndex: General Notices (1) Apply To All Monographs and Other TextsGhenaNo ratings yet
- Software Quality Assurance AssingmentDocument7 pagesSoftware Quality Assurance AssingmentSheikh HashirNo ratings yet
- Aromatherapy As Complementary Medicine: Amira Ahmed Kamal El-Din El-AnssaryDocument13 pagesAromatherapy As Complementary Medicine: Amira Ahmed Kamal El-Din El-AnssarySava VijakNo ratings yet
- Specialty Pharmacy Business PlanDocument14 pagesSpecialty Pharmacy Business PlanNishchal PaudelNo ratings yet
- Endocrine SystemDocument27 pagesEndocrine SystemJhemDelfin100% (1)
- 1.5-DOH Reviewer & Examination-NurseDocument111 pages1.5-DOH Reviewer & Examination-NurseRoger CarpisoNo ratings yet
- Morley-Senkler Et Al-2022-Cochrane Database of Systematic ReviewsDocument12 pagesMorley-Senkler Et Al-2022-Cochrane Database of Systematic ReviewsVenessaEdeNo ratings yet
- Congestive Heart Failure (CHF) / Decompensation Cordis Functional Class (DCFCDocument25 pagesCongestive Heart Failure (CHF) / Decompensation Cordis Functional Class (DCFCYUSRIL ZUMADINSYAHNo ratings yet
- RCSI Supplement - MedicineDocument22 pagesRCSI Supplement - MedicineIoana GusatuNo ratings yet
- Sepsis OverviewDocument45 pagesSepsis Overviewzul kandiNo ratings yet
- Pedia Drug StudyDocument5 pagesPedia Drug StudyTyn TynNo ratings yet
- Anti Biotics: Acive Princble Indication Family NameDocument61 pagesAnti Biotics: Acive Princble Indication Family NameAhmed FekryNo ratings yet
- Opsonin Pharma ListDocument14 pagesOpsonin Pharma ListDelegate Tech100% (1)
- Publicação 2Document8 pagesPublicação 2BrunoNo ratings yet
- 5 25 17 Migraines PowerPointDocument40 pages5 25 17 Migraines PowerPointSaifi AlamNo ratings yet
- Cumulative NCLEX Test May 2023Document29 pagesCumulative NCLEX Test May 2023Julie Ann100% (2)
- Management of Warfarin-Associated Bleeding or Supratherapeutic INR - UpToDateDocument41 pagesManagement of Warfarin-Associated Bleeding or Supratherapeutic INR - UpToDatejames lxNo ratings yet
- Barcode ObatDocument6 pagesBarcode Obatmr. ARCxxxiNo ratings yet
- Article On C.rutidosperma PDFDocument3 pagesArticle On C.rutidosperma PDFBhagirath GogikarNo ratings yet
- Guideline Watch 2021Document24 pagesGuideline Watch 2021Pedro NicolatoNo ratings yet
- Pharmacology Respiratory DrugsDocument51 pagesPharmacology Respiratory DrugsAngel DamoNo ratings yet
- 6 135Document6 pages6 135Ashok LenkaNo ratings yet
- Drug Addiction and Prevention ReviewerDocument6 pagesDrug Addiction and Prevention ReviewerAira NicoleNo ratings yet