You might also like
- 911 Pigeon Disease & Treatment Protocols!From Everand911 Pigeon Disease & Treatment Protocols!Rating: 4 out of 5 stars4/5 (1)
- Rotavirus structural proteins & causes diarrheaDocument4 pagesRotavirus structural proteins & causes diarrheayusrinastitiNo ratings yet
- Diarrhea in Neonatal RuminantsDocument8 pagesDiarrhea in Neonatal Ruminantsbarbybackup2No ratings yet
- Transmissible Gastroenteritis1Document6 pagesTransmissible Gastroenteritis1pedroNo ratings yet
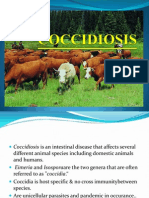
- CoccidiosisDocument6 pagesCoccidiosisAnaNo ratings yet
- CORONAVIRUS AVIAN INFECTIOUS BRONCHITIS VIRUSDocument10 pagesCORONAVIRUS AVIAN INFECTIOUS BRONCHITIS VIRUSMuhammad Arslan UsmanNo ratings yet
- Fowl PoxDocument3 pagesFowl PoxakhmadfuadiNo ratings yet
- Under Natural ConditionsDocument3 pagesUnder Natural ConditionsSantosh BhandariNo ratings yet
- Clostridial infections-LR3Document8 pagesClostridial infections-LR3yomifNo ratings yet
- Other Intestinal ProtozoansDocument26 pagesOther Intestinal ProtozoansCharlene SuliganNo ratings yet
- Reoviridae Birnaviridae: General and Systemic Virology (MICRO - 303)Document11 pagesReoviridae Birnaviridae: General and Systemic Virology (MICRO - 303)Muhammad Arslan UsmanNo ratings yet
- 7 DiarreaDocument19 pages7 DiarreajuanapetequiaNo ratings yet
- Rotavirus Case DiscussionDocument7 pagesRotavirus Case DiscussionNakajima AtsushiNo ratings yet
- Amebiasis and Giardiasis-FinalDocument25 pagesAmebiasis and Giardiasis-FinalDaniel AtiehNo ratings yet
- My Presentation On Johnes DiseaseDocument45 pagesMy Presentation On Johnes Diseaserohishaak100% (1)
- Intestinal Pathogens: Department of Clinical Microbiology Medical Faculty Universitas BrawijayaDocument56 pagesIntestinal Pathogens: Department of Clinical Microbiology Medical Faculty Universitas BrawijayaPipitNo ratings yet
- Viro Final 6Document10 pagesViro Final 6Muhammad Arslan UsmanNo ratings yet
- Enterobacteriaceae: Dr. BetsyDocument36 pagesEnterobacteriaceae: Dr. BetsySoham BanikNo ratings yet
- Ascaris LumbricoidesDocument33 pagesAscaris LumbricoidesRosi Gustina100% (5)
- Salmonella, The Host and Disease: A Brief ReviewDocument8 pagesSalmonella, The Host and Disease: A Brief ReviewPedro Albán MNo ratings yet
- Ascaris Lumbricoides NotesDocument4 pagesAscaris Lumbricoides NotesrositasholekhaNo ratings yet
- Ciliate and FlagellatesDocument95 pagesCiliate and FlagellatesJohn AdvinculaNo ratings yet
- Infectious DiseaseDocument33 pagesInfectious DiseaseebraheemelmandouhNo ratings yet
- Ascaris LumbricoidesDocument15 pagesAscaris LumbricoidesJyoti DasNo ratings yet
- Cdnursing PPT 2021Document37 pagesCdnursing PPT 2021yuuki konnoNo ratings yet
- Feline Panleukopenia Balram YadavDocument16 pagesFeline Panleukopenia Balram Yadavsanchi ranaNo ratings yet
- Contagious Ecthyma: Orf, Contagious Pustular Dermatitis, Sore Mouth, Scabby MouthDocument27 pagesContagious Ecthyma: Orf, Contagious Pustular Dermatitis, Sore Mouth, Scabby MouthMohammedNo ratings yet
- Salmonellosis 1Document15 pagesSalmonellosis 1BforbatNo ratings yet
- Bacterial Pneumonia Causative Agents Transmission RoutesDocument7 pagesBacterial Pneumonia Causative Agents Transmission RoutesRusselle BuyaNo ratings yet
- Feline Panleukopenia: Directed By: DR - Nadir Khosa DVM, Uvas, LahoreDocument11 pagesFeline Panleukopenia: Directed By: DR - Nadir Khosa DVM, Uvas, LahoreVetlife DvpNo ratings yet
- FInal Laboratory Activity Microbiology LABESORESDocument10 pagesFInal Laboratory Activity Microbiology LABESORESJAN ELMER L. LABESORESNo ratings yet
- Gram Positive BacilliDocument6 pagesGram Positive BacilliSteve ShirmpNo ratings yet
- Veterinary Medicine Individual AssignmentDocument6 pagesVeterinary Medicine Individual AssignmentObsaNo ratings yet
- Prrs (Porcine Reproductive and Respiratory Syndrome) : GijaponDocument43 pagesPrrs (Porcine Reproductive and Respiratory Syndrome) : GijaponFrance GijaponNo ratings yet
- Systemic Infections From GiDocument10 pagesSystemic Infections From GiJake MillerNo ratings yet
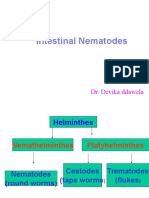
- Intestinal Nematodes: Dr. Devika DdawelaDocument127 pagesIntestinal Nematodes: Dr. Devika DdawelaPraveenKumarNo ratings yet
- Pathogenic SpirillaDocument7 pagesPathogenic SpirillaHamidreza RahmaniNo ratings yet
- CoccidiosisDocument45 pagesCoccidiosissherinshahs2010No ratings yet
- Coxsackie VirusDocument10 pagesCoxsackie Virusjyothsna yarraNo ratings yet
- Enteric FeverDocument7 pagesEnteric FeverkudzaimuregidubeNo ratings yet
- Swine Digestive Diseases GuideDocument28 pagesSwine Digestive Diseases GuidePETJSNVENo ratings yet
- Project IN Parasitology: Submitted To: Dr. Ed de Vera Submitted By: Francesca Angela Nervar BSN - 2Document36 pagesProject IN Parasitology: Submitted To: Dr. Ed de Vera Submitted By: Francesca Angela Nervar BSN - 2Catherine MetraNo ratings yet
- Dent 201 MB Shegillae Week 9.Document19 pagesDent 201 MB Shegillae Week 9.sima mhammedNo ratings yet
- Pyometrainsmallanimals: Ragnvi HagmanDocument23 pagesPyometrainsmallanimals: Ragnvi HagmansalomonNo ratings yet
- Diarréia em Potros - 2007Document3 pagesDiarréia em Potros - 2007thiago.veterinariaNo ratings yet
- Ascaris Lumbricoides: I. MorphologyDocument6 pagesAscaris Lumbricoides: I. MorphologyJoseline SorianoNo ratings yet
- Feline Panleukopenia Virus Infection and Other Viral EnteritidesDocument8 pagesFeline Panleukopenia Virus Infection and Other Viral EnteritidesjohanNo ratings yet
- Foot and Mouth DiseasesDocument9 pagesFoot and Mouth Diseaseseutamène ramziNo ratings yet
- Ascaris lumbricoides Literature ReviewDocument10 pagesAscaris lumbricoides Literature ReviewDina Fitri FauziahNo ratings yet
- Rota Virus: Presented byDocument13 pagesRota Virus: Presented byLalnuntluanga RalteNo ratings yet
- Topic: "Picoronoviruses. Coxsackie. ECHO. Laboratory Diagnostics"Document26 pagesTopic: "Picoronoviruses. Coxsackie. ECHO. Laboratory Diagnostics"deekshit dcNo ratings yet
- Infectious Bursal Disease Virus (IBDV) Etiology, Transmission, Clinical SignsDocument3 pagesInfectious Bursal Disease Virus (IBDV) Etiology, Transmission, Clinical SignsDr. Prakash PanthiNo ratings yet
- Project IN Parasitology: Submitted To: Dr. Ed de Vera Submitted By: Francesca Angela Nervar BSN - 2Document38 pagesProject IN Parasitology: Submitted To: Dr. Ed de Vera Submitted By: Francesca Angela Nervar BSN - 2Catherine MetraNo ratings yet
- 2 - Lower Respiratory InfectionsDocument106 pages2 - Lower Respiratory InfectionsAda JoraimiNo ratings yet
- 105 Brucellosis: Etiology/Pathophysiology EpidemiologyDocument3 pages105 Brucellosis: Etiology/Pathophysiology EpidemiologyDamián ContrerasNo ratings yet
- Nematode Infections 2019 Student PDFDocument272 pagesNematode Infections 2019 Student PDFCharlene SuliganNo ratings yet
- VIRUS INOCULATION IN EMBRYONIC CHICKEN’S EGGDocument8 pagesVIRUS INOCULATION IN EMBRYONIC CHICKEN’S EGGPuri RahmaNo ratings yet
- Canine Parvovirus: Dulce A. AgsanoDocument19 pagesCanine Parvovirus: Dulce A. AgsanoDulce AgsanoNo ratings yet
- Roundworm Infection Causes and TreatmentDocument20 pagesRoundworm Infection Causes and TreatmentDeladem EmmanuelNo ratings yet
- Infectious Diseases: CowpoxDocument3 pagesInfectious Diseases: CowpoxMohammedNo ratings yet
- Carruthers - The Case For Massively Modular Models of MindDocument21 pagesCarruthers - The Case For Massively Modular Models of MindMira LandesmanNo ratings yet
- L Dilemma of Designer Babies Paul Knoepfler WorksheetDocument3 pagesL Dilemma of Designer Babies Paul Knoepfler WorksheetRene MacapanasNo ratings yet
- Factors Analysis of Cultural Heritages Preservation With Tamsui CaseDocument22 pagesFactors Analysis of Cultural Heritages Preservation With Tamsui Case謝天梧No ratings yet
- 3C Development of Organisms PDFDocument74 pages3C Development of Organisms PDFBryan YeohNo ratings yet
- Dna Microarray Technology: Fatoki John OlabodeDocument9 pagesDna Microarray Technology: Fatoki John Olabodejohn tokiNo ratings yet
- 12 Production and Purification of Recombinant Glargine Insulin From Escherichia Coli BL-21 StrainDocument12 pages12 Production and Purification of Recombinant Glargine Insulin From Escherichia Coli BL-21 StrainAnand KumarNo ratings yet
- Productive Soil Ecosystem ClassificationDocument8 pagesProductive Soil Ecosystem ClassificationFransche BeukesNo ratings yet
- Concepts of The Cell Theory: Cell Structure and FunctionDocument31 pagesConcepts of The Cell Theory: Cell Structure and FunctionGracious Angel Bautista IgnacioNo ratings yet
- Class Xii Practical 2021-22Document21 pagesClass Xii Practical 2021-22vedant raikarNo ratings yet
- Leber Hereditary Optic Neuropathy Review of TreatmDocument8 pagesLeber Hereditary Optic Neuropathy Review of Treatmfebyan yohanesNo ratings yet
- GPB-101-Fundamentals of Genetics & CytogeneticsDocument162 pagesGPB-101-Fundamentals of Genetics & CytogeneticsKING ArthurNo ratings yet
- DRSMARTANDANUOLUWAI NITIATIVE BIO102QUESTIONSANDANSWERSDocument10 pagesDRSMARTANDANUOLUWAI NITIATIVE BIO102QUESTIONSANDANSWERSOluwabamire Oreoluwa100% (8)
- RadVacWhite Paper SARS CoV 2 Vaccine Ver 3 3 1Document69 pagesRadVacWhite Paper SARS CoV 2 Vaccine Ver 3 3 1Karoline MarxNo ratings yet
- Kaplan: Clinical Chemistry, 5 Edition: Clinical References - Methods of AnalysisDocument9 pagesKaplan: Clinical Chemistry, 5 Edition: Clinical References - Methods of AnalysisSaad KhanNo ratings yet
- Caramba: A First-In-Human Clinical Trial With SLAMF7 CAR-T Cells Prepared by Virus-Free Sleeping Beauty Gene Transfer To Treat Multiple MyelomaDocument12 pagesCaramba: A First-In-Human Clinical Trial With SLAMF7 CAR-T Cells Prepared by Virus-Free Sleeping Beauty Gene Transfer To Treat Multiple MyelomaCarlos Meza HernandezNo ratings yet
- Gene Silencing - Antisense RNA & SiRNADocument18 pagesGene Silencing - Antisense RNA & SiRNAvenkatsuriyaprakash100% (1)
- Accepted Manuscript: 10.1016/j.npep.2018.07.001Document34 pagesAccepted Manuscript: 10.1016/j.npep.2018.07.001mr dexterNo ratings yet
- ESMO Preceptorship On Breast Cancer Lisbon SepteDocument73 pagesESMO Preceptorship On Breast Cancer Lisbon SepteStancaMihaiAlexandruNo ratings yet
- Biotechnology8 q3 Mod2 Manipulation-of-Genetic-MaterialDocument16 pagesBiotechnology8 q3 Mod2 Manipulation-of-Genetic-Materialunc b40% (5)
- 610 Irregular VerbsDocument18 pages610 Irregular VerbsCureshNo ratings yet
- Scientific American Biology For A Changing World With Core Physiology 3rd Edition Shuster Test BankDocument34 pagesScientific American Biology For A Changing World With Core Physiology 3rd Edition Shuster Test Bankbrittanysummerstrkayoizcj100% (8)
- Fundamental Unit of Life Class 9 WsDocument2 pagesFundamental Unit of Life Class 9 WsKshiti HNo ratings yet
- Activity No. 3 The Cell As A School (Module-1)Document2 pagesActivity No. 3 The Cell As A School (Module-1)Andrea MacayaNo ratings yet
- Neonatal HypotoniaDocument8 pagesNeonatal Hypotoniazulfiqar aliNo ratings yet
- 2019 YEARLY LESSON PLAN FOR FORM 1 SCIENCEDocument18 pages2019 YEARLY LESSON PLAN FOR FORM 1 SCIENCESITI NURSYIFA BINTI ROZALI MoeNo ratings yet
- Protein Analysis WorkflowDocument37 pagesProtein Analysis WorkflowKurdianto MSiNo ratings yet
- DiphteriaDocument24 pagesDiphteriasalmaNo ratings yet
- Psma MidtermDocument206 pagesPsma MidtermPrincess Rose GamboaNo ratings yet
- Complete Botany 111Document44 pagesComplete Botany 111Sukriti BaniyaNo ratings yet
- Biology Paper 1 November 1999Document30 pagesBiology Paper 1 November 1999k391No ratings yet