You might also like
- Ejaculatory Dysfunction in Patient With Schizophrenia On SertindoleDocument4 pagesEjaculatory Dysfunction in Patient With Schizophrenia On SertindoleIda MaryaniNo ratings yet
- Sexual Pharmacology in The 21st CenturyDocument9 pagesSexual Pharmacology in The 21st CenturyFawaaz KhurwolahNo ratings yet
- Off-Label Trazodone Prescription-Evidence, Benefits and RisksDocument9 pagesOff-Label Trazodone Prescription-Evidence, Benefits and RisksomarapesNo ratings yet
- Drugs For Urologic DisordersDocument10 pagesDrugs For Urologic DisordersMajd HusseinNo ratings yet
- Pharmacologic Management of Adult Depression: Stephen M. Adams, MD Karl E. Miller, MD and Robert G. Zylstra, Edd, LCSWDocument8 pagesPharmacologic Management of Adult Depression: Stephen M. Adams, MD Karl E. Miller, MD and Robert G. Zylstra, Edd, LCSWruth_villagraNo ratings yet
- Indian Herbs That Act As 5-Alpha Reductase InhibitorsDocument9 pagesIndian Herbs That Act As 5-Alpha Reductase InhibitorsMan ManNo ratings yet
- Bala 2017Document6 pagesBala 2017amit1109No ratings yet
- Combination Medical Therapy For Lower Urinary Tract Symptoms and Benign Prostatic HyperplasiaDocument9 pagesCombination Medical Therapy For Lower Urinary Tract Symptoms and Benign Prostatic HyperplasiaganangahimsaNo ratings yet
- Vortioxetine: A Review of Its Use in Major Depressive DisorderDocument20 pagesVortioxetine: A Review of Its Use in Major Depressive DisorderDaniela PeñaNo ratings yet
- EndoquestionssolvedDocument14 pagesEndoquestionssolvedPuteri Nursyamimi Mohd SabilanNo ratings yet
- A Review of Trazodone Use in Psychiatric and Medical ConditionsDocument10 pagesA Review of Trazodone Use in Psychiatric and Medical ConditionsdoutormarcosNo ratings yet
- Sexual Dysfunction in Selective Serotonin Reuptake Inhibitors (Ssris) and Potential Solutions: A Narrative Literature ReviewDocument6 pagesSexual Dysfunction in Selective Serotonin Reuptake Inhibitors (Ssris) and Potential Solutions: A Narrative Literature ReviewsyahdanNo ratings yet
- Current Status of 5 of Lower Urinary Tract Symptoms and BPH: - Reductase Inhibitors in The ManagementDocument8 pagesCurrent Status of 5 of Lower Urinary Tract Symptoms and BPH: - Reductase Inhibitors in The ManagementApriani BahoriNo ratings yet
- The Relationship Between Clinical Pharmacokinetics of Aripiprazole and CYP2D6 Genetic Polymorphism: Effects of CYP Enzyme Inhibition by Coadministration of Paroxetine or FluvoxamineDocument9 pagesThe Relationship Between Clinical Pharmacokinetics of Aripiprazole and CYP2D6 Genetic Polymorphism: Effects of CYP Enzyme Inhibition by Coadministration of Paroxetine or FluvoxamineIulia CiocotisanNo ratings yet
- Molecules 18 07323Document13 pagesMolecules 18 07323Luis AtencioNo ratings yet
- Neuroactive Steroid Levels Are Modified in Cerebrospinal Fluid and Plasma of Post-Finasteride Patients Showing Persistent Sexual Side Effects and Anxious/Depressive SymptomatologyDocument6 pagesNeuroactive Steroid Levels Are Modified in Cerebrospinal Fluid and Plasma of Post-Finasteride Patients Showing Persistent Sexual Side Effects and Anxious/Depressive SymptomatologyVDNo ratings yet
- Adverse Effects of ParoxetineDocument4 pagesAdverse Effects of ParoxetineIssa umulimaNo ratings yet
- Selective Serotonin-Reuptake InhibitorsDocument10 pagesSelective Serotonin-Reuptake InhibitorsAndyka Prima PratamaNo ratings yet
- 15 5a-Reductase Inhibitors in Benign Prostatic Hyperplasia and Prostate Cancer Risk ReductionDocument14 pages15 5a-Reductase Inhibitors in Benign Prostatic Hyperplasia and Prostate Cancer Risk ReductionDr-Mandeep SinghNo ratings yet
- Orthomolecular Botanical Treatments - For SchizophreniaDocument18 pagesOrthomolecular Botanical Treatments - For SchizophreniaLeanne MontgomeryNo ratings yet
- NCLEX: Drugs for Urologic Disorders: DRUGS USED TO TREAT ERECTILE DYSFUNCTION AND BPHDocument8 pagesNCLEX: Drugs for Urologic Disorders: DRUGS USED TO TREAT ERECTILE DYSFUNCTION AND BPHjthsNo ratings yet
- Prolonged Post-Treatment Genital Anesthesia and Sexual Dysfunction Following Discontinuation of Citalopram and The Atypical Antidepressant NefazodoneDocument3 pagesProlonged Post-Treatment Genital Anesthesia and Sexual Dysfunction Following Discontinuation of Citalopram and The Atypical Antidepressant NefazodoneJulio JuarezNo ratings yet
- Khazaie2015 (Revisi)Document6 pagesKhazaie2015 (Revisi)ihsansabridrNo ratings yet
- Sem 4 Lectura 2 Inhibidores de Recaptación de SerotoninaDocument18 pagesSem 4 Lectura 2 Inhibidores de Recaptación de SerotoninaJesús MoraNo ratings yet
- UpToDate Second-Generation Antipsychotic Medications: Pharmacology, Administration, and Side EffectsDocument59 pagesUpToDate Second-Generation Antipsychotic Medications: Pharmacology, Administration, and Side EffectsalbdapplimNo ratings yet
- Alopecia Androgenética.. Uma Atualização Das Opções de Tratamento (Traduzir Artigo)Document16 pagesAlopecia Androgenética.. Uma Atualização Das Opções de Tratamento (Traduzir Artigo)Alexia Vieira de SouzaNo ratings yet
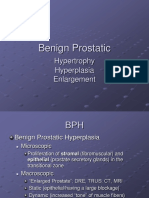
- Benign Prostatic: Hypertrophy Hyperplasia EnlargementDocument40 pagesBenign Prostatic: Hypertrophy Hyperplasia EnlargementAyu PurbaNo ratings yet
- Antidepressant Side Effects 2006Document9 pagesAntidepressant Side Effects 2006Renny AnggrainiNo ratings yet
- Trazodone Cognitive Vitality For ResearchersDocument6 pagesTrazodone Cognitive Vitality For ResearchersCerbari AnatolNo ratings yet
- Pharmacotherapy For Generalized Anxiety Disorder PDFDocument16 pagesPharmacotherapy For Generalized Anxiety Disorder PDFdreaming100% (1)
- BPH Smith English-6-15Document10 pagesBPH Smith English-6-15novi camiumNo ratings yet
- AntiandrogensDocument22 pagesAntiandrogenstheintrovNo ratings yet
- Erectile Dysfunction: QuestionsDocument24 pagesErectile Dysfunction: QuestionsSayed NourNo ratings yet
- Cvja 18 213Document3 pagesCvja 18 213arpitlyall27No ratings yet
- Venlafaxine (: DepressionDocument7 pagesVenlafaxine (: DepressionMilos MitrovicNo ratings yet
- Update On Management of The Oral and Maxillofac - 2022 - Oral and MaxillofacialDocument8 pagesUpdate On Management of The Oral and Maxillofac - 2022 - Oral and MaxillofacialFadi Al HajjiNo ratings yet
- 07 Atmaca 2020Document8 pages07 Atmaca 2020Vivian FrancoNo ratings yet
- A Comparative Review On Avanafil Vs Tadalafil Vs Sildenafil TabletDocument5 pagesA Comparative Review On Avanafil Vs Tadalafil Vs Sildenafil TabletZeyad A AbdullahNo ratings yet
- BPH JurnalDocument35 pagesBPH Jurnalrevina_revi0% (1)
- 5-HT-Related Drugs and Human Experimental AnxietyDocument4 pages5-HT-Related Drugs and Human Experimental AnxietyIvan VillatoroNo ratings yet
- David J. Greenblatt D. (ZOLPIDEM) 2Document9 pagesDavid J. Greenblatt D. (ZOLPIDEM) 2Antonio SanchezNo ratings yet
- Pharmacotherapy For Generalized Anxiety Disorder in Adults - UpToDate V eDocument14 pagesPharmacotherapy For Generalized Anxiety Disorder in Adults - UpToDate V eMonique GloverNo ratings yet
- Role of SSRIs in Psychiatric DisordersDocument38 pagesRole of SSRIs in Psychiatric Disordersfaisalnadeem100% (1)
- Pharmacotherapy For Generalized Anxiety Disorder in Adults - UpToDateDocument16 pagesPharmacotherapy For Generalized Anxiety Disorder in Adults - UpToDateLeonardoMartínezNo ratings yet
- Transsexual Transgendered Guide To Obtaining and Using Transsexual Hormones, Hormone Replacement Therapy HRTDocument52 pagesTranssexual Transgendered Guide To Obtaining and Using Transsexual Hormones, Hormone Replacement Therapy HRTTrinity Rose Transsexual77% (13)
- Fluoxetine Vs Tozadone RCTDocument7 pagesFluoxetine Vs Tozadone RCTAhsan KhanNo ratings yet
- Benign Prostatic HyperplasiaDocument18 pagesBenign Prostatic HyperplasiaGunawan SadewoNo ratings yet
- Farmakoterapi Inkontinensia Urin, Enuresis, BPHDocument43 pagesFarmakoterapi Inkontinensia Urin, Enuresis, BPHAnastasya LunasikifaNo ratings yet
- Opioid-Induced Androgen Deficiency (OPIAD)Document12 pagesOpioid-Induced Androgen Deficiency (OPIAD)EnzoNo ratings yet
- Acute Dystonia Case Report with ParoxetineDocument2 pagesAcute Dystonia Case Report with ParoxetineRenny SulelinoNo ratings yet
- Goldenberg M (Sildenafil)Document16 pagesGoldenberg M (Sildenafil)Antonio SanchezNo ratings yet
- PCOL2605 ADR and I ReportDocument8 pagesPCOL2605 ADR and I ReportsxphiastarNo ratings yet
- 5-ARIs Role in Treating BPHDocument5 pages5-ARIs Role in Treating BPHkanaNo ratings yet
- Clinical Endocrinology - 2020 - Angus - A Systematic Review of Antiandrogens and Feminization in Transgender WomenDocument10 pagesClinical Endocrinology - 2020 - Angus - A Systematic Review of Antiandrogens and Feminization in Transgender WomenGiuseppe NuciferoNo ratings yet
- Tretman Aseksualnosti Kod AntidepresivaDocument5 pagesTretman Aseksualnosti Kod AntidepresivaNebojsa JanjicNo ratings yet
- A Double-Blind, Randomized, Pilot Dose-Finding Study of Maca Root (L. Meyenii) For The Management of SSRI-Induced Sexual DysfunctionDocument10 pagesA Double-Blind, Randomized, Pilot Dose-Finding Study of Maca Root (L. Meyenii) For The Management of SSRI-Induced Sexual DysfunctionLudi12345No ratings yet
- Benign Prostatic Hypertrophy: An Update On Drug TherapyDocument2 pagesBenign Prostatic Hypertrophy: An Update On Drug TherapyAjieRnie IDNo ratings yet
- The Psychopharmacology of ParoxetineDocument7 pagesThe Psychopharmacology of ParoxetineolivukovicNo ratings yet
- Effect of Antidepressant Medications On Semen Parameters and Male FertilityDocument8 pagesEffect of Antidepressant Medications On Semen Parameters and Male FertilitySueNo ratings yet
- Cell Signalling Biology - Ion Channels (2012)Document72 pagesCell Signalling Biology - Ion Channels (2012)Apróné Török IbolyaNo ratings yet
- ReadingDocument7 pagesReadingTUTOR IELTS0% (1)
- Blood Collection, Equipment, Additives, and Order of DrawDocument29 pagesBlood Collection, Equipment, Additives, and Order of DrawLyonTrioréNo ratings yet
- Konstantinov 2000Document5 pagesKonstantinov 2000cth103No ratings yet
- Rotation 4 - DarundayDocument16 pagesRotation 4 - DarundayEzra Miguel DarundayNo ratings yet
- CHSE Science Revised Syllabus 20-21 PDFDocument106 pagesCHSE Science Revised Syllabus 20-21 PDFsandeep prASAD PATRONo ratings yet
- Radtke-Schuller2016 Article BrainAtlasOfTheMongolianGerbilDocument272 pagesRadtke-Schuller2016 Article BrainAtlasOfTheMongolianGerbilCharlotte NordenNo ratings yet
- Induction BioDocument161 pagesInduction BioFaheem UllahNo ratings yet
- 7.5A Bromothymol Blue LabDocument6 pages7.5A Bromothymol Blue LabKeely TrauberNo ratings yet
- Updated Action Potential & Nerve StimulationDocument4 pagesUpdated Action Potential & Nerve Stimulationamir elhadiNo ratings yet
- Anne E. Urai: EmploymentDocument5 pagesAnne E. Urai: EmploymentAnne UraiNo ratings yet
- Mark Scheme (Results) Summer 2012: International GCSE Human Biology (4HB0) Paper 01Document14 pagesMark Scheme (Results) Summer 2012: International GCSE Human Biology (4HB0) Paper 01MalihaNo ratings yet
- Jan BI1 - 2001Document13 pagesJan BI1 - 2001skarun1No ratings yet
- Pharma Module 1 PDFDocument22 pagesPharma Module 1 PDFSheryhan Tahir BayleNo ratings yet
- Hemoglobin and Myoglobin 2Document78 pagesHemoglobin and Myoglobin 2Soffa ShmuelNo ratings yet
- Efectele Speciilor Reactive de Oxigen Asupra Sistemului de Reproducere FemininDocument8 pagesEfectele Speciilor Reactive de Oxigen Asupra Sistemului de Reproducere FemininLuminita HutanuNo ratings yet
- Gujarat - University PAPERS 2020-2022Document36 pagesGujarat - University PAPERS 2020-2022Shlok RathodNo ratings yet
- NEUROMUSCULAR TRANSMISSION: ANATOMY AND PHYSIOLOGYDocument45 pagesNEUROMUSCULAR TRANSMISSION: ANATOMY AND PHYSIOLOGYparuNo ratings yet
- Respiratory System Semi FinalDocument60 pagesRespiratory System Semi FinalMichelle AnteneroNo ratings yet
- Synaptic Neurotransmission and Parts of The Brain NOTESDocument6 pagesSynaptic Neurotransmission and Parts of The Brain NOTESDaniNo ratings yet
- Understanding the Upper ExtremitiesDocument30 pagesUnderstanding the Upper ExtremitiesLaura Lee CliffordNo ratings yet
- Metamorphosis in InsectsDocument13 pagesMetamorphosis in InsectsAnupam GhoshNo ratings yet
- 30 Investigations IA IdeasDocument7 pages30 Investigations IA IdeasYasmine Ouled Kaddour El HallaouiNo ratings yet
- Breathing and Exchange of Gases Part4Document12 pagesBreathing and Exchange of Gases Part4GAURANSH AlaghNo ratings yet
- Eukaryotic and Prokaryotic Cells Practice Exam Questions HigherDocument3 pagesEukaryotic and Prokaryotic Cells Practice Exam Questions HigherboneyNo ratings yet
- Angelo BanaresDocument11 pagesAngelo BanaresNathan Russel PangilinanNo ratings yet
- INSOMNIA ScriptDocument2 pagesINSOMNIA ScriptZeribinNo ratings yet
- ThalamusDocument21 pagesThalamusTem GemechuNo ratings yet
- Ncert Solutions Class 9 Science Chapter 5Document6 pagesNcert Solutions Class 9 Science Chapter 5ppusapatiNo ratings yet
- Worksheet Plant Growth 1 - ANSWERSDocument4 pagesWorksheet Plant Growth 1 - ANSWERSDwight DsilvaNo ratings yet