You might also like
- MCQ Pract Pharma 1Document9 pagesMCQ Pract Pharma 1Syamil AzharNo ratings yet
- How To Switch Insulin Products - Pharm LetterDocument6 pagesHow To Switch Insulin Products - Pharm LetterAraceli LeonNo ratings yet
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesFrom EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesRating: 4 out of 5 stars4/5 (2)
- Practical Insulin: A Handbook for Prescribing ProvidersFrom EverandPractical Insulin: A Handbook for Prescribing ProvidersRating: 5 out of 5 stars5/5 (2)
- Biopuncture and Antihomotoxic TreatmentDocument65 pagesBiopuncture and Antihomotoxic TreatmentRaúl CornejoNo ratings yet
- Standards of Care 2021 Figure 9.2Document2 pagesStandards of Care 2021 Figure 9.2Ariel GutierrezNo ratings yet
- Insulin algorithm for type 1 diabetes in children and adultsDocument1 pageInsulin algorithm for type 1 diabetes in children and adultspraful.mehtaNo ratings yet
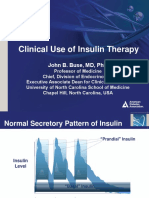
- Slide Clinical Use of Insulin Therapy (ADA)Document36 pagesSlide Clinical Use of Insulin Therapy (ADA)Dian SobaNo ratings yet
- Insulin Adjustment TREND 2023Document16 pagesInsulin Adjustment TREND 2023Rana Ahsan JavedNo ratings yet
- INSULINDocument6 pagesINSULINmilaNo ratings yet
- Type 1 Diabetes Treatment AlgorithmDocument1 pageType 1 Diabetes Treatment AlgorithmChristopher BeckerNo ratings yet
- Diabetes Cheat SheetDocument2 pagesDiabetes Cheat Sheetmanuel iglesiasNo ratings yet
- Diabetes SobrebasalizaciónDocument7 pagesDiabetes SobrebasalizaciónComisión Académica FCM - UNAHNo ratings yet
- CHAPTER 7 - Inpatient Management of Diabetes and HyperglycemiaDocument6 pagesCHAPTER 7 - Inpatient Management of Diabetes and HyperglycemiaenesNo ratings yet
- GUIDELINES FOR INPATIENT DIABETES MANAGEMENT هااامDocument1 pageGUIDELINES FOR INPATIENT DIABETES MANAGEMENT هااامAbu HuzaifaNo ratings yet
- Insulin Algorithm For Type 2 Diabetes in Children and AdultsDocument6 pagesInsulin Algorithm For Type 2 Diabetes in Children and AdultsOlesiaNo ratings yet
- Insulin Therapy: A Personal Approach: Mayer B. DavidsonDocument13 pagesInsulin Therapy: A Personal Approach: Mayer B. DavidsonRetri AtikaNo ratings yet
- Adjusting Your Insulin DoseDocument3 pagesAdjusting Your Insulin DoseLib AsNo ratings yet
- Blood Glucose Control Pathway in Type 2 Diabetes Apr 2013Document2 pagesBlood Glucose Control Pathway in Type 2 Diabetes Apr 2013J WongNo ratings yet
- Switching Between InsulinDocument2 pagesSwitching Between InsulinThoufiNo ratings yet
- Insulina Humana Menos Cara JAMADocument2 pagesInsulina Humana Menos Cara JAMApaulina farfanNo ratings yet
- Dok 21Document2 pagesDok 21dr. Noni PrisciliaNo ratings yet
- Updated Diabetes Guidelines - DR NandaDocument19 pagesUpdated Diabetes Guidelines - DR NandaMonish Sudhakar100% (1)
- EInsulin RegiemDocument18 pagesEInsulin RegiemzahrabokerNo ratings yet
- DKA/HHS Diagnostic Criteria and Treatment PhasesDocument6 pagesDKA/HHS Diagnostic Criteria and Treatment PhasesmarshaNo ratings yet
- Optimizing The Use of NPH Insulin in Patients With Type 2 Diabetes MellitusDocument3 pagesOptimizing The Use of NPH Insulin in Patients With Type 2 Diabetes MellitusGulzaib KhokharNo ratings yet
- The Essential Role of Insulin in Diabetes ManagementDocument9 pagesThe Essential Role of Insulin in Diabetes ManagementAbdul SamadNo ratings yet
- Simplify Insulin Therapy With IDegAsp Co-Formulation - 2022 UpdtDocument21 pagesSimplify Insulin Therapy With IDegAsp Co-Formulation - 2022 UpdtTataNo ratings yet
- Update Management DMDocument27 pagesUpdate Management DMnando8396No ratings yet
- MILV8N8Document4 pagesMILV8N8garywall.ukNo ratings yet
- Novolin and HumulinDocument3 pagesNovolin and HumulinChynnaNo ratings yet
- H. E. Hopkinson, R. M. Jacques, K. J. Gardner, S. A. Amiel and P. MansellDocument6 pagesH. E. Hopkinson, R. M. Jacques, K. J. Gardner, S. A. Amiel and P. MansellDidi SaputraNo ratings yet
- Insulin Protocols for Diabetic PatientsDocument16 pagesInsulin Protocols for Diabetic PatientsSitti Mardiya SariolNo ratings yet
- Insulin IssuesDocument6 pagesInsulin Issuesdoctorzo0% (1)
- Assessment Diagnosis Outcome Interventions Rationale EvaluationDocument6 pagesAssessment Diagnosis Outcome Interventions Rationale EvaluationHanna La MadridNo ratings yet
- Fit-Diploma 3-2-2024Document57 pagesFit-Diploma 3-2-2024light tweenNo ratings yet
- Less Hypoglycemia With Insulin Glargine in Intensive Insulin Therapy For Type 1 DiabetesDocument5 pagesLess Hypoglycemia With Insulin Glargine in Intensive Insulin Therapy For Type 1 DiabetesUduman IsmailNo ratings yet
- Insulin Initiation PPT - PPTX 2Document53 pagesInsulin Initiation PPT - PPTX 2Meno Ali100% (1)
- How Early Should Basal Insulin Be Used in Management of T2DM-intention BaruDocument36 pagesHow Early Should Basal Insulin Be Used in Management of T2DM-intention BaruRuri harmawantiNo ratings yet
- 2011 - Practical Guide Insulin TherapyDocument6 pages2011 - Practical Guide Insulin Therapytheva_thy100% (1)
- Alprazolam (Systemic)Document14 pagesAlprazolam (Systemic)RIRINo ratings yet
- Basal Bolus Insulin Titration AhsDocument2 pagesBasal Bolus Insulin Titration AhsAnn A.100% (1)
- Mod4 Insulin CurvesDocument5 pagesMod4 Insulin Curvesjaya28655746No ratings yet
- Rabbit Formulary: Inhalation AnestheticsDocument3 pagesRabbit Formulary: Inhalation AnestheticsMiriam CervantesNo ratings yet
- Practical Guidance On Intensification of Insulin Therapy With Biasp 30: A Consensus StatementDocument7 pagesPractical Guidance On Intensification of Insulin Therapy With Biasp 30: A Consensus StatementAlizaPinkyNo ratings yet
- Insulin As PartDocument3 pagesInsulin As PartRezaNo ratings yet
- Glycemic ControlDocument2 pagesGlycemic ControlHildaNo ratings yet
- 2022 Insulin Calculations Cheat Sheet ARDocument4 pages2022 Insulin Calculations Cheat Sheet ARGulsama BabarNo ratings yet
- Adult Intravenous Aminophylline ProtocolDocument3 pagesAdult Intravenous Aminophylline ProtocolNataliaNo ratings yet
- DM Lab 2 - FinalDocument33 pagesDM Lab 2 - FinalMahamed Wefkey OmranNo ratings yet
- Rapid-Acting Insulin (Onset: 15-30 MinsDocument5 pagesRapid-Acting Insulin (Onset: 15-30 MinsBea TanNo ratings yet
- COVID-19 Positive Patient - Dexamethasone GuidanceDocument2 pagesCOVID-19 Positive Patient - Dexamethasone GuidanceLe Hoang TuanNo ratings yet
- Algorithm For Blood Glucose Lowering Therapy in Adults With Type 2 Diabetes PDF 2185604173Document1 pageAlgorithm For Blood Glucose Lowering Therapy in Adults With Type 2 Diabetes PDF 2185604173AlessioNavarraNo ratings yet
- Nutrition Risk Assessment and ManagementDocument3 pagesNutrition Risk Assessment and ManagementSitty Aizah MangotaraNo ratings yet
- Avandia RosiglitazoneDocument1 pageAvandia RosiglitazoneCassieNo ratings yet
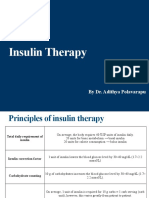
- Insulin Therapy: by Dr. Adithya PolavarapuDocument18 pagesInsulin Therapy: by Dr. Adithya Polavarapuadithya polavarapuNo ratings yet
- Diabetes Mellitus: Types, Symptoms, Diagnosis and TreatmentDocument58 pagesDiabetes Mellitus: Types, Symptoms, Diagnosis and TreatmentAgatha NightrayNo ratings yet
- DInsulin Types 1Document22 pagesDInsulin Types 1zahrabokerNo ratings yet
- T2D PharmacologyDocument2 pagesT2D PharmacologyTan Thay HuiNo ratings yet
- Oral RevalidaDocument39 pagesOral Revalidajunathancortez123No ratings yet
- Insulin HandbookDocument67 pagesInsulin HandbookThits SarNo ratings yet
- Drug Name Mechanism of Action Indication Side Effects Nursing Reponsibilities Generic NameDocument4 pagesDrug Name Mechanism of Action Indication Side Effects Nursing Reponsibilities Generic NamehahahaNo ratings yet
- Nama ObatDocument13 pagesNama Obatsahmin sahminNo ratings yet
- Prof J. Kasule, FRCS, FRCOG Department of Obstetrics and Gynaecology University of ZimbabweDocument17 pagesProf J. Kasule, FRCS, FRCOG Department of Obstetrics and Gynaecology University of ZimbabwedanielNo ratings yet
- Evolution of Miasm Concept in Light of Germ TheoryDocument4 pagesEvolution of Miasm Concept in Light of Germ TheoryRamesh ShahNo ratings yet
- 4thQ Week1 PPT DigestiveDocument49 pages4thQ Week1 PPT DigestiveGeronimo SantiagoNo ratings yet
- Clinical Practice Handbook For Quality Abortion CareDocument66 pagesClinical Practice Handbook For Quality Abortion CareRaj ShahNo ratings yet
- Obstetrics AclsDocument6 pagesObstetrics AclsPedro BurgosNo ratings yet
- AlbuminDocument16 pagesAlbuminMaroofAliNo ratings yet
- DiethylcarbamazineDocument8 pagesDiethylcarbamazinePrakob GikokNo ratings yet
- Annotated Bibliography of Obstetrics & Gynaecology ResourcesDocument4 pagesAnnotated Bibliography of Obstetrics & Gynaecology ResourcesKaku ManishaNo ratings yet
- Wender Utah PDFDocument3 pagesWender Utah PDFFco CanaleNo ratings yet
- Approach To Patient With Endocrine DisordersDocument2 pagesApproach To Patient With Endocrine DisordersSeff CausapinNo ratings yet
- Amit BiomedSignalDocument14 pagesAmit BiomedSignalDr-Amit Kumar SinghNo ratings yet
- Bronchiolitis Obliterans PDFDocument7 pagesBronchiolitis Obliterans PDFSatnam KaurNo ratings yet
- JURNAL GonoreDocument20 pagesJURNAL GonoreRuni Arumndari100% (1)
- Dialogue Unit 8: Example of A DialogueDocument4 pagesDialogue Unit 8: Example of A DialogueIsfaNo ratings yet
- Respiratory Physiology in Pregnancy ReviewDocument13 pagesRespiratory Physiology in Pregnancy ReviewAlejandra RequesensNo ratings yet
- Caduet (Dr. Ismahun Maret 2009)Document41 pagesCaduet (Dr. Ismahun Maret 2009)Yulia SumarnaNo ratings yet
- Health and Disease Status of Thai Pangas, Bangladesh: Pangasius Hypophthalmus Cultured in Rural Ponds of MymensinghDocument3 pagesHealth and Disease Status of Thai Pangas, Bangladesh: Pangasius Hypophthalmus Cultured in Rural Ponds of MymensinghgooedliaNo ratings yet
- Homoeopathic Drug Pictures PDFDocument718 pagesHomoeopathic Drug Pictures PDFNimesh PatelNo ratings yet
- Medical AbbreviationsDocument6 pagesMedical AbbreviationsEina CarmonaNo ratings yet
- Achilles Tendinopathy What Runners Should Know FinitoDocument4 pagesAchilles Tendinopathy What Runners Should Know FinitoAdmirNo ratings yet
- Rosnimar NOK Campur Padat ENG AFDocument21 pagesRosnimar NOK Campur Padat ENG AFberriandi_arwanNo ratings yet
- Cough NCPDocument2 pagesCough NCPMYLENE GRACE ELARCOSANo ratings yet
- Studies: Coagulation The DigitalisDocument7 pagesStudies: Coagulation The Digitalisfebyan yohanesNo ratings yet
- Hypotension PulgoDocument8 pagesHypotension PulgoDumbo Dog lolNo ratings yet
- МартDocument55 pagesМартLuisAngelPonceTorresNo ratings yet
- Group 1Document41 pagesGroup 1SELEMAYE ZENEBENo ratings yet
- Renal PhysiologyDocument5 pagesRenal PhysiologyJayricDepalobosNo ratings yet