You might also like
- Fast Facts: Optimización del tratamiento de las fluctuaciones motoras en la enfermedad de Parkinson: Adaptando el tratamiento al pacienteFrom EverandFast Facts: Optimización del tratamiento de las fluctuaciones motoras en la enfermedad de Parkinson: Adaptando el tratamiento al pacienteNo ratings yet
- Antiepileptic DrugsDocument43 pagesAntiepileptic DrugsdrpraneethpremkumarNo ratings yet
- Antiepileptic Drugs (Aed) : R. Anita. IndriyantiDocument36 pagesAntiepileptic Drugs (Aed) : R. Anita. Indriyantiandisti2323No ratings yet
- MDW 2017 Day 2 Track 2 Session 9 Bradley Reducing PolypharmacyDocument9 pagesMDW 2017 Day 2 Track 2 Session 9 Bradley Reducing PolypharmacyAmparo VillamilNo ratings yet
- Pertimbangan Pemilihan Obat Anti Epilepsi DR Nelly Edit 23 JanDocument53 pagesPertimbangan Pemilihan Obat Anti Epilepsi DR Nelly Edit 23 Janvenus002No ratings yet
- Aging and Drug HandlingDocument4 pagesAging and Drug HandlingJadys Merill DiezNo ratings yet
- Drugs in PregnancyDocument72 pagesDrugs in PregnancyNu Joe100% (1)
- Geriatric Pharmacology: Lisa Rosenberg, MD Touro University Nevada April 6, 2011Document45 pagesGeriatric Pharmacology: Lisa Rosenberg, MD Touro University Nevada April 6, 2011Recky Patala100% (1)
- Antimicrobial Regimen Selection (Quick AnswersL Pharmacy Book)Document16 pagesAntimicrobial Regimen Selection (Quick AnswersL Pharmacy Book)Yasmin ElsobkyNo ratings yet
- Geriatrics Prescribing GuidelinessDocument27 pagesGeriatrics Prescribing GuidelinessSayli Gore100% (1)
- 2011 Updates in Therapeutics: P P: The Pharmacotherapy Preparatory Review and Recertification CourseDocument11 pages2011 Updates in Therapeutics: P P: The Pharmacotherapy Preparatory Review and Recertification CourseDrx ahmed MaherNo ratings yet
- Farmakologi GeriatriDocument40 pagesFarmakologi Geriatrishatna nadila bellaNo ratings yet
- Drug Study #1Document7 pagesDrug Study #1Sarah Kaye BañoNo ratings yet
- Unit 8 Drugs Acting On The Endocrine SystemDocument26 pagesUnit 8 Drugs Acting On The Endocrine SystemTherese Margarette SantiagoNo ratings yet
- DRUG and IVF StudyDocument4 pagesDRUG and IVF StudyJohanna Camelle Insong MonteronNo ratings yet
- Farmakologi Dari Obat EpilepsiDocument82 pagesFarmakologi Dari Obat EpilepsiDion SaputraNo ratings yet
- Farmakologi Geriatri: Oleh: P. Santoso, S.Si.,M.Biomed, AptDocument40 pagesFarmakologi Geriatri: Oleh: P. Santoso, S.Si.,M.Biomed, AptEva Dharma WahyuniNo ratings yet
- Antiepileptic DrugsDocument63 pagesAntiepileptic Drugsvpd100% (1)
- Fall 2023 Classification of MedicationsDocument6 pagesFall 2023 Classification of Medicationsramyharoon2004No ratings yet
- Drug Treatment of EpilepsyDocument81 pagesDrug Treatment of EpilepsyAnifowose SamsonNo ratings yet
- Mood Stabilisers: PsychopharmacologyDocument50 pagesMood Stabilisers: Psychopharmacologymeno321No ratings yet
- Kasus 2 - Kelompok 1 - PC-1Document21 pagesKasus 2 - Kelompok 1 - PC-1NURZAINURANo ratings yet
- Presented By: Raghav Dogra M.Pharm (Analysis) 2016-2017Document38 pagesPresented By: Raghav Dogra M.Pharm (Analysis) 2016-2017gggNo ratings yet
- LECT-5B - Patient Case and MISCDocument31 pagesLECT-5B - Patient Case and MISCnonaNo ratings yet
- 24 Antiseizure DrugsDocument71 pages24 Antiseizure DrugsThea MallariNo ratings yet
- Pharmacology Dr. Scott PDFDocument90 pagesPharmacology Dr. Scott PDFSingey LhendupNo ratings yet
- Drug Interactions in Dentistry: Iyad Abou Rabii DDS, Omfs, Mres, PHDDocument45 pagesDrug Interactions in Dentistry: Iyad Abou Rabii DDS, Omfs, Mres, PHDIyad Abou-Rabii100% (1)
- Drug StudyDocument4 pagesDrug StudyDean Angelo BarrientosNo ratings yet
- Eti Nurwening Sholikhah: Department of Pharmacology & Therapy Faculty of Medicine Universitas Gadjah MadaDocument43 pagesEti Nurwening Sholikhah: Department of Pharmacology & Therapy Faculty of Medicine Universitas Gadjah MadaadystiNo ratings yet
- Anti Epileptic DrugsDocument89 pagesAnti Epileptic DrugsInderjeet SohalNo ratings yet
- Drug StudyDocument6 pagesDrug StudyRosemarie CarpioNo ratings yet
- Antiseizure: Medical University of Sofia, Faculty of Medicine Department of Pharmacology and ToxicologyDocument29 pagesAntiseizure: Medical University of Sofia, Faculty of Medicine Department of Pharmacology and Toxicologybudirahmant0No ratings yet
- 2principles of Geriatric Pharmacotherapy - Lee - 10-19-10Document53 pages2principles of Geriatric Pharmacotherapy - Lee - 10-19-10Mbel'z Mbel'z Embil'zNo ratings yet
- GIT Renal Endo ReviewDocument43 pagesGIT Renal Endo Reviewshaira.maebbrnNo ratings yet
- Geriatric PharmacologyDocument33 pagesGeriatric PharmacologyArsal MushtaqNo ratings yet
- Antiepileptic Drugs-Good LectureDocument55 pagesAntiepileptic Drugs-Good LecturealijanmarwatNo ratings yet
- Therapeutic Drug Monitoring in The ElderlyDocument3 pagesTherapeutic Drug Monitoring in The ElderlyKristine BaringNo ratings yet
- DRUGSTUDYDocument6 pagesDRUGSTUDYMauriceNo ratings yet
- 4853 Medication Worksheet: Student NameDocument8 pages4853 Medication Worksheet: Student Nameapi-546817891No ratings yet
- Drug Study 1-Ward1Document4 pagesDrug Study 1-Ward1Annaoj Esor DarasNo ratings yet
- 2018 Obat Pada ManulaDocument62 pages2018 Obat Pada ManulaShafira Nur Amalia ZulvaNo ratings yet
- Diazepam, Lanoxin, Hemostan, NaprexDocument6 pagesDiazepam, Lanoxin, Hemostan, NaprexRene John Francisco100% (1)
- DementiaDocument57 pagesDementiaPriyash JainNo ratings yet
- Go SPIRONOLACTONE-PODocument4 pagesGo SPIRONOLACTONE-POSAMANTHA T. MODESTONo ratings yet
- Bumetanide MIMSDocument2 pagesBumetanide MIMSIndri WahyuniNo ratings yet
- LisinoprilDocument3 pagesLisinoprilLIEZEL GRACE VELAYONo ratings yet
- Mindanao State University - Iligan Institute of Technology Student: - SectionDocument2 pagesMindanao State University - Iligan Institute of Technology Student: - SectionJohn Pearl FernandezNo ratings yet
- Antidiabetic Drugs - AMBOSSDocument13 pagesAntidiabetic Drugs - AMBOSSOpio IsaacNo ratings yet
- 16 - Metabolism and Pharmacogenomics - 2023Document29 pages16 - Metabolism and Pharmacogenomics - 2023Rhythm BhardwajNo ratings yet
- For MaDocument9 pagesFor MaKathrina TumbagaNo ratings yet
- AntihistaminesDocument36 pagesAntihistaminesAli ElattarNo ratings yet
- Camuso OtcDocument15 pagesCamuso Otcapi-548307464No ratings yet
- AcetazolamideDocument1 pageAcetazolamideKyuSheenNo ratings yet
- Drug Name WPS OfficeDocument2 pagesDrug Name WPS OfficeCAMILLE GAIL HADJIRANINo ratings yet
- Antiseizures DrugsDocument27 pagesAntiseizures DrugsIrene Zae MwandotoNo ratings yet
- Captopril - Drug MonographDocument1 pageCaptopril - Drug MonographshahzadNo ratings yet
- Lisinopril Drug StudyDocument2 pagesLisinopril Drug StudyKristinelou Marie Reyna100% (1)
- Republic of The Philippines University Town, Northern SamarDocument2 pagesRepublic of The Philippines University Town, Northern SamarJosef Angelo PoldoNo ratings yet
- Antacid Drug AnalysisDocument2 pagesAntacid Drug AnalysisJosef Angelo PoldoNo ratings yet
- Onsult: Ementia Reatment PdateDocument5 pagesOnsult: Ementia Reatment PdateAxel Robinson HerreraNo ratings yet
- Mangalam Drugs ReportDocument1 pageMangalam Drugs ReportBKSNo ratings yet
- Brody Hall - Exercício Terapêutico Na Busca Da Função, 3 Ed, 2011 (Inglês)Document802 pagesBrody Hall - Exercício Terapêutico Na Busca Da Função, 3 Ed, 2011 (Inglês)SerenelaNo ratings yet
- FC Continuous Education Microcredentials July 2021 (3354)Document9 pagesFC Continuous Education Microcredentials July 2021 (3354)Luis Peralta GuzmanNo ratings yet
- Health Checklist: NG:) Lumunok)Document2 pagesHealth Checklist: NG:) Lumunok)Rose Duron GumaNo ratings yet
- The Effects of Exercise On The Nervous SystemDocument2 pagesThe Effects of Exercise On The Nervous SystemramadanNo ratings yet
- International Wound Journal Volume 7 Issue 4 2010 (Doi 10.1111/j.1742-481x.2010.00682.x) Christine A Chrisman - Care of Chronic Wounds in Palliative Care and End-Of-Life Patients PDFDocument22 pagesInternational Wound Journal Volume 7 Issue 4 2010 (Doi 10.1111/j.1742-481x.2010.00682.x) Christine A Chrisman - Care of Chronic Wounds in Palliative Care and End-Of-Life Patients PDFNovaNo ratings yet
- Icd X: Diagnose ICD Diagnosa ICDDocument33 pagesIcd X: Diagnose ICD Diagnosa ICDannisa statiraNo ratings yet
- Our Lady of Fatima University College of Nursing - Cabanatuan CityDocument3 pagesOur Lady of Fatima University College of Nursing - Cabanatuan CityDanica FrancoNo ratings yet
- Aspirin Paracetamol CaffeineDocument3 pagesAspirin Paracetamol CaffeineMariusNeicuNo ratings yet
- Neri, Angela - Act. 1,2,3Document5 pagesNeri, Angela - Act. 1,2,3Angela NeriNo ratings yet
- NUR194 ADocument15 pagesNUR194 AJemuel DalanaNo ratings yet
- DNRDocument1 pageDNRabiangdanNo ratings yet
- Hypertension HistoryDocument2 pagesHypertension HistorybassamNo ratings yet
- Law Exam NotesDocument11 pagesLaw Exam NotesEric Cheng100% (1)
- Mixed Lymphocyte Culture / Reaction (MLC / MLR)Document2 pagesMixed Lymphocyte Culture / Reaction (MLC / MLR)Muthi KhairunnisaNo ratings yet
- UntitledDocument14 pagesUntitledsyntacs skNo ratings yet
- Permintaan Lab 2023Document9 pagesPermintaan Lab 2023imanNo ratings yet
- Orbino, Frances Anne N. 4th Rot FdarDocument2 pagesOrbino, Frances Anne N. 4th Rot FdarFrances OrbinoNo ratings yet
- Methode EBOODocument37 pagesMethode EBOOjohanNo ratings yet
- The Bipolar Affective Disorder Dimension Scale (BADDS) - A Dimensional Scale For Rating Lifetime Psychopathology in Bipolar Spectrum DisordersDocument11 pagesThe Bipolar Affective Disorder Dimension Scale (BADDS) - A Dimensional Scale For Rating Lifetime Psychopathology in Bipolar Spectrum DisordersDM YazdaniNo ratings yet
- ID-IM-SQ-E ToolDocument9 pagesID-IM-SQ-E TooltriciacamilleNo ratings yet
- Hospital Design - AUHDocument108 pagesHospital Design - AUHDion LakonawaNo ratings yet
- 01SMARTeZ IFU 09.27.2017 Rev 4Document4 pages01SMARTeZ IFU 09.27.2017 Rev 4Rucha PavagadhiNo ratings yet
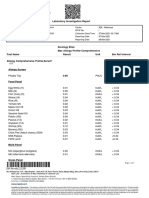
- Laboratory Investigation ReportDocument7 pagesLaboratory Investigation ReportAmarjeetNo ratings yet
- Fluid Therapy and Shock: An Integrative Literature Review: Joana Silva, Luís Gonçalves and Patrícia Pontífice SousaDocument6 pagesFluid Therapy and Shock: An Integrative Literature Review: Joana Silva, Luís Gonçalves and Patrícia Pontífice Sousateguh sulistiyantoNo ratings yet
- PsoriasisDocument0 pagesPsoriasisaurax143No ratings yet
- Tabel Severitas BPJS Tindakan JantungDocument9 pagesTabel Severitas BPJS Tindakan JantungTeduh ParamadinaNo ratings yet
- Investigatory Project On AnalgesicsDocument30 pagesInvestigatory Project On AnalgesicsAnurag Singh100% (1)
- Management of The Third Stage of LaborDocument12 pagesManagement of The Third Stage of Laborayu_pieterNo ratings yet
- Journal Reading - Myringitis - Elisabeth PattyDocument14 pagesJournal Reading - Myringitis - Elisabeth PattyLipatOla123No ratings yet