You might also like
- 11 Blues Piano Voicings AnalysisDocument11 pages11 Blues Piano Voicings AnalysisBHNo ratings yet
- The Lord of The Rings Real HistoryDocument2 pagesThe Lord of The Rings Real HistoryDUNCAN0420No ratings yet
- Bible Reading ChartDocument2 pagesBible Reading ChartZ. Wen100% (6)
- Jean Genet - Deathwatch-Faber & Faber (1961) PDFDocument38 pagesJean Genet - Deathwatch-Faber & Faber (1961) PDFValentin MarcosNo ratings yet
- Neurology StrokeDocument1,531 pagesNeurology StrokelguerreroNo ratings yet
- Pregnancy Tests Explained (2Nd Edition): Current Trends of Antenatal TestsFrom EverandPregnancy Tests Explained (2Nd Edition): Current Trends of Antenatal TestsNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 8: UrologyFrom EverandComplementary and Alternative Medical Lab Testing Part 8: UrologyRating: 3 out of 5 stars3/5 (1)
- Harry Potter and The Sorceror's StoneDocument17 pagesHarry Potter and The Sorceror's StoneParth Tiwari50% (4)
- Expertravel V CA DigestDocument2 pagesExpertravel V CA DigestJeahMaureenDominguez100% (1)
- Cystatin C As A Novel Predictor of Preterm Labor in Severe PreeclampsiaDocument9 pagesCystatin C As A Novel Predictor of Preterm Labor in Severe PreeclampsiahandiNo ratings yet
- RESEARCH ARTICLEOpen AccessChallenges of Acute Peritoneal Dialysis Inextremely-Low-Birth-Weight Infants - Aretrospective Cohort StudyDocument9 pagesRESEARCH ARTICLEOpen AccessChallenges of Acute Peritoneal Dialysis Inextremely-Low-Birth-Weight Infants - Aretrospective Cohort StudysavitageraNo ratings yet
- A Study To Compare Maternal and Perinatal Outcome in Early vs. Late Onset PreeclampsiaDocument8 pagesA Study To Compare Maternal and Perinatal Outcome in Early vs. Late Onset PreeclampsiaEriekafebriayana RNo ratings yet
- Captura de Pantalla 2022-10-31 A La(s) 15.52.35 PDFDocument9 pagesCaptura de Pantalla 2022-10-31 A La(s) 15.52.35 PDFEliab Rene RobletoNo ratings yet
- Study of Sociodemographic Profile, Maternal, Fetal Outcome in Preeclamptic and Eclamptic Women A Prospective StudyDocument6 pagesStudy of Sociodemographic Profile, Maternal, Fetal Outcome in Preeclamptic and Eclamptic Women A Prospective StudyHarvey MatbaganNo ratings yet
- Early - and Late-Onset Preeclampsia A ComprehensiveDocument10 pagesEarly - and Late-Onset Preeclampsia A ComprehensiveEriekafebriayana RNo ratings yet
- The Association Between HaemogDocument13 pagesThe Association Between Haemogmiss betawiNo ratings yet
- Hellp Syndrome PDFDocument11 pagesHellp Syndrome PDFLisya AnggraeniNo ratings yet
- Defining Reduced Urine Output in Neonatal ICU ImpoDocument10 pagesDefining Reduced Urine Output in Neonatal ICU Impohamudek kasaNo ratings yet
- Supportive Management of Pregnancy-Associated Aplastic AnemiaDocument6 pagesSupportive Management of Pregnancy-Associated Aplastic AnemiaAs YuYu MustafaNo ratings yet
- Fetomaternal Outcome and Raised Bilirubin Level in PregnancyDocument4 pagesFetomaternal Outcome and Raised Bilirubin Level in PregnancyPrima Hari PratamaNo ratings yet
- Does This Patient Have Acute Kidney Injury? An AKI ChecklistDocument4 pagesDoes This Patient Have Acute Kidney Injury? An AKI ChecklistOlga HMNo ratings yet
- Asociacion Funcion Renal Materna y Resultados Embarazo DM 1 y 2.seah.2020Document8 pagesAsociacion Funcion Renal Materna y Resultados Embarazo DM 1 y 2.seah.2020Andrés Gaviria CNo ratings yet
- Detal Grouth Restriccion As Initial Finding of Preecalmpsia Is A Clinical Predictor of Maternal and Neonatal Prognoses A Singel Centrer Retrospective StudyDocument8 pagesDetal Grouth Restriccion As Initial Finding of Preecalmpsia Is A Clinical Predictor of Maternal and Neonatal Prognoses A Singel Centrer Retrospective Studyalexriosparra92No ratings yet
- Acute Kidney Injury in ChildrenDocument8 pagesAcute Kidney Injury in ChildrenInfectologia ClinicaNo ratings yet
- Hematological Profile of Pregnant Women at St. Paul 'S Hospital Millennium Medical College, Addis Ababa, EthiopiaDocument7 pagesHematological Profile of Pregnant Women at St. Paul 'S Hospital Millennium Medical College, Addis Ababa, Ethiopiaade lydia br.siregarNo ratings yet
- E058068 FullDocument7 pagesE058068 FullJordan HutabaratNo ratings yet
- Management of Acute Kidney Injury in Children: Sri Lanka Journal of Child Health January 2019Document6 pagesManagement of Acute Kidney Injury in Children: Sri Lanka Journal of Child Health January 2019HannaSaskiaIINo ratings yet
- 8 Juni Folic Acid GDM 2020Document14 pages8 Juni Folic Acid GDM 2020Ario DaniantoNo ratings yet
- Pregnancy-Related Liver Disorders: Seminar Journal of Clinical and Experimental HepatologyDocument12 pagesPregnancy-Related Liver Disorders: Seminar Journal of Clinical and Experimental HepatologysaryindrianyNo ratings yet
- 2014 Article 390 PDFDocument8 pages2014 Article 390 PDFGlucose DRglucoseNo ratings yet
- Anemia-1Document15 pagesAnemia-1Intan Wahyu CahyaniNo ratings yet
- Pregnancy and Peritoneal Dialysis An Updated ReviewDocument12 pagesPregnancy and Peritoneal Dialysis An Updated ReviewSid TorresNo ratings yet
- MJMU Volume 50 Issue 4 Pages 155-163-1Document9 pagesMJMU Volume 50 Issue 4 Pages 155-163-1Fred OkelloNo ratings yet
- The Definition of Acute Kidney Injury and Its Use in PracticeDocument12 pagesThe Definition of Acute Kidney Injury and Its Use in PracticeErwin SiahaanNo ratings yet
- FullPIERS Paper-LancetDocument39 pagesFullPIERS Paper-LancetRyan SadonoNo ratings yet
- A K N H: Evidence Based Clinical Practice Guidelines For The Management of Severe Pre-EclampsiaDocument14 pagesA K N H: Evidence Based Clinical Practice Guidelines For The Management of Severe Pre-EclampsiaAL AHLINo ratings yet
- Medi 102 E33898Document7 pagesMedi 102 E33898ade lydia br.siregarNo ratings yet
- Articulo 1Document8 pagesArticulo 1maria cotamoNo ratings yet
- Diagnosis and Treatment of Acute Kidney Injury in PediatricsDocument13 pagesDiagnosis and Treatment of Acute Kidney Injury in PediatricsagungNo ratings yet
- Nakimuli2016 Article TheBurdenOfMaternalMorbidityAnDocument8 pagesNakimuli2016 Article TheBurdenOfMaternalMorbidityAnPriscilla AdetiNo ratings yet
- The Definition of Acute Kidney Injury and Its Use in PracticeDocument12 pagesThe Definition of Acute Kidney Injury and Its Use in PracticewelinNo ratings yet
- ACOG Committee Opinion No 348 Umbilical Cord Blood Gas and Acid-Base AnalysisDocument4 pagesACOG Committee Opinion No 348 Umbilical Cord Blood Gas and Acid-Base AnalysisLina E. Arango100% (1)
- Uq398926 OaDocument56 pagesUq398926 OaBárbara Irrazabal MedinaNo ratings yet
- Maternal and Perinatal Complications of Severe Preeclampsia in Three Referral Hospitals in Yaoundé, CameroonDocument8 pagesMaternal and Perinatal Complications of Severe Preeclampsia in Three Referral Hospitals in Yaoundé, CameroonIke Istofani KNo ratings yet
- Jurnal Reading ObygnDocument6 pagesJurnal Reading ObygnLimastani FebrianaNo ratings yet
- BR J Haematol - 2014 - Oteng Ntim - Pregnancy Outcome in Patients With Sickle Cell Disease in The UK A National CohortDocument9 pagesBR J Haematol - 2014 - Oteng Ntim - Pregnancy Outcome in Patients With Sickle Cell Disease in The UK A National CohortJustine ObedNo ratings yet
- 3 Nefro AnakDocument9 pages3 Nefro AnakPutri Rizky AmaliaNo ratings yet
- LkjsfandfksdaDocument6 pagesLkjsfandfksdanatalpaatNo ratings yet
- Hellp WordDocument3 pagesHellp WordriannofiansyahNo ratings yet
- Spot Urinary Albumin Creatinine Ratio As A PredictDocument7 pagesSpot Urinary Albumin Creatinine Ratio As A PredictFatimahNo ratings yet
- The Effect of Maternal Anemia On Maternal and Neonatal Outcomes in Twin PregnanciesDocument5 pagesThe Effect of Maternal Anemia On Maternal and Neonatal Outcomes in Twin PregnanciesDarmawan HariyantoNo ratings yet
- Effect of High-Dose Folic Acid Supplementation On The Prevention of Preeclampsia in Twin PregnancyDocument7 pagesEffect of High-Dose Folic Acid Supplementation On The Prevention of Preeclampsia in Twin PregnancyAzmia TabahNo ratings yet
- Yuan2019 Article IronDeficiencyInLatePregnancyA PDFDocument11 pagesYuan2019 Article IronDeficiencyInLatePregnancyA PDFDekaraNo ratings yet
- Short Term Prediction of PE 2020Document9 pagesShort Term Prediction of PE 2020marag10No ratings yet
- 1471 2369 14 154 PDFDocument10 pages1471 2369 14 154 PDFhanifahrafaNo ratings yet
- Chronic Kidney Disease: A Large-Scale Population-Based Study of The Effects of Introducing The CKD-EPI Formula For eGFR ReportingDocument10 pagesChronic Kidney Disease: A Large-Scale Population-Based Study of The Effects of Introducing The CKD-EPI Formula For eGFR Reportingmufti alghoffarNo ratings yet
- Association Between Neonatal Hyperglycemia and Retinopathy of Prematurity 2021Document10 pagesAssociation Between Neonatal Hyperglycemia and Retinopathy of Prematurity 2021juancho_3m7No ratings yet
- Jog 13555Document9 pagesJog 13555nilamsaryNo ratings yet
- Sick Day Management in Children and Adolescents With Diabetes 2009Document8 pagesSick Day Management in Children and Adolescents With Diabetes 2009golden fleeceNo ratings yet
- The Importance of Proteinuria in Preeclampsia and Its Predictive Role in Maternal and Neonatal OutcomesDocument9 pagesThe Importance of Proteinuria in Preeclampsia and Its Predictive Role in Maternal and Neonatal OutcomesimuhammadfahmiNo ratings yet
- DIC in Abruptio 2Document5 pagesDIC in Abruptio 2HoneylynNo ratings yet
- 1 s2.0 S2210778919304714 MainDocument6 pages1 s2.0 S2210778919304714 MainsandrakucabaNo ratings yet
- Jurnal Intern 2Document7 pagesJurnal Intern 2Annisaa AndrianaNo ratings yet
- Maternal Serum Leptin As A Marker of PreeclampsiaDocument6 pagesMaternal Serum Leptin As A Marker of PreeclampsiaAlfa FebriandaNo ratings yet
- Calcium For Pre-Eclampsia Prevention: A Systematic Review and Network Meta - Analysis To Guide Personalised Antenatal CareDocument11 pagesCalcium For Pre-Eclampsia Prevention: A Systematic Review and Network Meta - Analysis To Guide Personalised Antenatal CareNetty AndrianaNo ratings yet
- Jurnal PEDocument7 pagesJurnal PEIris BerlianNo ratings yet
- European Journal of Obstetrics & Gynecology and Reproductive BiologyDocument5 pagesEuropean Journal of Obstetrics & Gynecology and Reproductive BiologyMostafa hosnyNo ratings yet
- Cardiology Síndrome de TakotsuboDocument7 pagesCardiology Síndrome de TakotsubolguerreroNo ratings yet
- Kidney Treatment Guidelines For HyponatremiaDocument7 pagesKidney Treatment Guidelines For HyponatremialguerreroNo ratings yet
- Hepatic EncephalopahyDocument13 pagesHepatic EncephalopahylguerreroNo ratings yet
- Kidney Preeclampsia 3Document6 pagesKidney Preeclampsia 3lguerreroNo ratings yet
- Ss 216 PDFDocument13 pagesSs 216 PDFlguerreroNo ratings yet
- Laboratory Guideline For Turner Syndrome.Document4 pagesLaboratory Guideline For Turner Syndrome.lguerreroNo ratings yet
- DeFronzo Et Al-2012-Diabetes, Obesity and MetabolismDocument10 pagesDeFronzo Et Al-2012-Diabetes, Obesity and MetabolismlguerreroNo ratings yet
- Genetica de La IraDocument11 pagesGenetica de La IralguerreroNo ratings yet
- Biography Charles Edouard Brown Sequard PDFDocument278 pagesBiography Charles Edouard Brown Sequard PDFlguerrero100% (1)
- Protein KinasesDocument494 pagesProtein KinaseslguerreroNo ratings yet
- Enfermedad de HirataDocument4 pagesEnfermedad de HiratalguerreroNo ratings yet
- Bristol Stool ChartDocument5 pagesBristol Stool ChartlguerreroNo ratings yet
- Capital Gains Tax Return BIR Form No 1706Document1 pageCapital Gains Tax Return BIR Form No 1706NGITPANo ratings yet
- LibreView Guide - Italian PaperDocument12 pagesLibreView Guide - Italian PaperJesus MuñozNo ratings yet
- Syllabus BSCDocument2 pagesSyllabus BSCHassan AliNo ratings yet
- 10th STD Smart English 2021-22 EditionDocument46 pages10th STD Smart English 2021-22 EditionSecure Chennai100% (1)
- Daftar PustakaDocument11 pagesDaftar PustakaHilyaNo ratings yet
- Desilvey S Curated Decay Heritage Beyond SavingDocument197 pagesDesilvey S Curated Decay Heritage Beyond SavingNastassjaSimeNo ratings yet
- Q1-M2 Genres of ViewingDocument41 pagesQ1-M2 Genres of ViewingChristine LlantoNo ratings yet
- Effect of Audit Findings and Audit RecommendationDocument25 pagesEffect of Audit Findings and Audit RecommendationDwi Puspita SariNo ratings yet
- CFA Career Guide 2014 PDFDocument121 pagesCFA Career Guide 2014 PDFAlex CNo ratings yet
- SNS CFE 102 0830 Religious Involvement 1 Paraan JoshuaDocument1 pageSNS CFE 102 0830 Religious Involvement 1 Paraan JoshuaLara May BasiladNo ratings yet
- Dress Code Lesson PlanDocument3 pagesDress Code Lesson Planapi-321908127No ratings yet
- Corporation PDFDocument8 pagesCorporation PDFKAMALINo ratings yet
- Department of Haematology: Test Name Result Unit Bio. Ref. Range MethodDocument4 pagesDepartment of Haematology: Test Name Result Unit Bio. Ref. Range MethodSiddhartha GuptaNo ratings yet
- MQB 09 WS 2Document4 pagesMQB 09 WS 2Nasmer BembiNo ratings yet
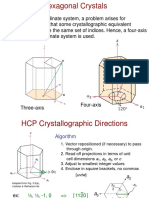
- Chap3.3 HexCrystal DirectionsDocument6 pagesChap3.3 HexCrystal DirectionsJeonghun LeeNo ratings yet
- Original PDF Deviant Behavior 11th Edition by Erich Goode PDFDocument41 pagesOriginal PDF Deviant Behavior 11th Edition by Erich Goode PDFcynthia.stewart295100% (32)
- PssDocument174 pagesPssdavev2005No ratings yet
- Trump Presidency 38 - June 20th, 2018 To July 14th, 2018Document501 pagesTrump Presidency 38 - June 20th, 2018 To July 14th, 2018FW040No ratings yet
- BBM11411 Final Exam 2022 S1Document5 pagesBBM11411 Final Exam 2022 S1bonaventure chipetaNo ratings yet
- 261 - TQB - Test HK2-11Document3 pages261 - TQB - Test HK2-11An LêNo ratings yet
- Jaltarang Instruments ShreyaDocument24 pagesJaltarang Instruments ShreyaKaushal DidwaniaNo ratings yet
- 4.-Content Based LearningDocument3 pages4.-Content Based LearningLuis Paz100% (1)
- Hsyallx: Tutorial Letter 301/3/2023Document32 pagesHsyallx: Tutorial Letter 301/3/2023Lebohang MalauNo ratings yet
- Art 2 SyllabusDocument2 pagesArt 2 Syllabusapi-260266731No ratings yet