You might also like
- Backache PDFDocument173 pagesBackache PDFteammrau100% (6)
- Disciplinary procedure stepsDocument10 pagesDisciplinary procedure stepsEl KhanNo ratings yet
- Grade 8 BowDocument7 pagesGrade 8 BowJorely Barbero MundaNo ratings yet
- Effect of Myofascial Release on Neck and Arm Pain FunctionDocument9 pagesEffect of Myofascial Release on Neck and Arm Pain FunctionDonny HendrawanNo ratings yet
- Tibia and Fibula Fracture PhysiotherapyDocument31 pagesTibia and Fibula Fracture Physiotherapyunknown unknown100% (1)
- Muscle & Fittness: Resents TheDocument34 pagesMuscle & Fittness: Resents TheauqaabNo ratings yet
- Effectiveness of Myofascial Trigger Point Release Technique To Evaluate Pain in Chronic Tension Type Headache Patients.Document40 pagesEffectiveness of Myofascial Trigger Point Release Technique To Evaluate Pain in Chronic Tension Type Headache Patients.Dr.Gopinath SaravananNo ratings yet
- Meaning and Definition of Management DevelopmentDocument7 pagesMeaning and Definition of Management DevelopmentRiteshTirkey100% (2)
- Community Engagement, Solidarity and Citizenship: Module 5 - Quarter 1Document28 pagesCommunity Engagement, Solidarity and Citizenship: Module 5 - Quarter 1Benjamin Fernandez Jr.67% (3)
- NEW - Hormone Balancing DrinkDocument9 pagesNEW - Hormone Balancing DrinkTAE'S POTATONo ratings yet
- Manual Therapy: Original ArticleDocument6 pagesManual Therapy: Original ArticleAlberto BeskowNo ratings yet
- Advances in The Diagnosis & Management of Neck Pain - Article.Document19 pagesAdvances in The Diagnosis & Management of Neck Pain - Article.salmankhan09215No ratings yet
- Changing Light Bulbs SafelyDocument1 pageChanging Light Bulbs SafelyAshok Suresh100% (4)
- India 2030 PDFDocument188 pagesIndia 2030 PDFGray HouserNo ratings yet
- Musculoskeletal Science and PracticeDocument7 pagesMusculoskeletal Science and Practicecris.endo.ceNo ratings yet
- EN - Cefaleia Tensional e Coluna CervicalDocument8 pagesEN - Cefaleia Tensional e Coluna Cervicalericagomes.fisioterapeutaNo ratings yet
- Physiotherapy Management of Neck Pain: Arianne P VerhagenDocument7 pagesPhysiotherapy Management of Neck Pain: Arianne P VerhagenHari25885No ratings yet
- A Neuroscience Perspective of Physical Treatment of Headache and Neck PainDocument7 pagesA Neuroscience Perspective of Physical Treatment of Headache and Neck PainOcha24 TupamahuNo ratings yet
- Multidisciplinary Manual Therapy Management of Cervicogenic Headache: A Case ReportDocument9 pagesMultidisciplinary Manual Therapy Management of Cervicogenic Headache: A Case ReportChirag MunjalNo ratings yet
- Estudio 7 - 10.1016@j.clinbDocument9 pagesEstudio 7 - 10.1016@j.clinbOLGUIN HUERTA CRISTIAN RODRIGONo ratings yet
- Florencio Et Al-2015-Pain MedicineDocument6 pagesFlorencio Et Al-2015-Pain Medicinecris.endo.ceNo ratings yet
- Ejp 1773Document20 pagesEjp 1773xbeligNo ratings yet
- Advances in The Diagnosis and Management of Neck PainDocument19 pagesAdvances in The Diagnosis and Management of Neck PainJose Fernando DiezNo ratings yet
- Bachelor of PhysiotherapyDocument9 pagesBachelor of Physiotherapyanushka.ganasanNo ratings yet
- Fpain 02 765921Document14 pagesFpain 02 765921xbeligNo ratings yet
- Neck Pain Practice Guidelines 2016Document17 pagesNeck Pain Practice Guidelines 2016pbhqanzghlcuviycmzNo ratings yet
- Neck Pain and Lower Back Pain. Med Clin N Am. 2019.Document14 pagesNeck Pain and Lower Back Pain. Med Clin N Am. 2019.Jose Fernando Diez100% (1)
- How To Explain Central Sensitization To PatientsDocument6 pagesHow To Explain Central Sensitization To PatientsrameshkulkarNo ratings yet
- Depauw 2014Document9 pagesDepauw 2014CarolinaNo ratings yet
- 1nueua6Document10 pages1nueua6Ncuhi DonggoNo ratings yet
- Evidence-Based PT for Cervical RadiculopathyDocument9 pagesEvidence-Based PT for Cervical RadiculopathyDr Abdallah BahaaNo ratings yet
- PHD ThesisDocument238 pagesPHD ThesisIlse van der BeekNo ratings yet
- 2013 Trriger Point ECOM + TMO en Cefalea CervicogenicaDocument9 pages2013 Trriger Point ECOM + TMO en Cefalea CervicogenicaPablo Cuevas SaldivarNo ratings yet
- 10 1002@ejp 1666Document45 pages10 1002@ejp 1666Gabriel DelfinoNo ratings yet
- J JBMT 2014 01 001Document10 pagesJ JBMT 2014 01 001yoverNo ratings yet
- Nonpharmacologic Management of Pain: Scott F. Nadler, DODocument7 pagesNonpharmacologic Management of Pain: Scott F. Nadler, DOGopi KrishnanNo ratings yet
- Evidence-Based Clinically-Informed Manual Therapy Clinical Reasoning For Headache ManagementDocument2 pagesEvidence-Based Clinically-Informed Manual Therapy Clinical Reasoning For Headache ManagementMarco AguirreNo ratings yet
- Tzenalis Study ProtocolDocument9 pagesTzenalis Study ProtocolCristoper PanjaitanNo ratings yet
- Clinical Presentation and Manual TherapyDocument11 pagesClinical Presentation and Manual TherapyVladislav KotovNo ratings yet
- Review of Vestibular Migraine: Current Understanding and Future DirectionsDocument15 pagesReview of Vestibular Migraine: Current Understanding and Future DirectionsSerdar MeteNo ratings yet
- 10 1097@j Pain 0000000000000591Document40 pages10 1097@j Pain 0000000000000591alonsoNo ratings yet
- Cervicogenic Headache Diagnosis and Treatment BogdukDocument10 pagesCervicogenic Headache Diagnosis and Treatment BogdukYoan PereiraNo ratings yet
- 1 s2.0 S0161475418300861 MainDocument9 pages1 s2.0 S0161475418300861 MainJuan David Arenas MendozaNo ratings yet
- Manual Therapy Versus Therapeutic Exercise in Non-Specific Chronic Neck Pain: A Randomized Controlled TrialDocument10 pagesManual Therapy Versus Therapeutic Exercise in Non-Specific Chronic Neck Pain: A Randomized Controlled TrialMichele MarengoNo ratings yet
- J JMPT 2012 09 003Document6 pagesJ JMPT 2012 09 003Tahira RajputNo ratings yet
- 2055 2386 5 14 PDFDocument8 pages2055 2386 5 14 PDFrima rizky nourliaNo ratings yet
- Practical Neurology - Evaluation of Cervicalgia With Headache (November - December 2010)Document8 pagesPractical Neurology - Evaluation of Cervicalgia With Headache (November - December 2010)KaniNo ratings yet
- PQ Art 37583-10Document7 pagesPQ Art 37583-10Vinay KumarNo ratings yet
- Comparison of Shoulder Muscle Strengthening Exercises With The Conventional Treatment of Mechanical Neck PainDocument13 pagesComparison of Shoulder Muscle Strengthening Exercises With The Conventional Treatment of Mechanical Neck PainDr. Krishna N. SharmaNo ratings yet
- Clinical Neurophysiology of Fatigue: M.J. Zwarts, G. Bleijenberg, B.G.M. Van EngelenDocument9 pagesClinical Neurophysiology of Fatigue: M.J. Zwarts, G. Bleijenberg, B.G.M. Van EngelenShyamali Kaushalya FernandoNo ratings yet
- Exercise Altering Pain MemoriesDocument6 pagesExercise Altering Pain MemoriesCelia CaballeroNo ratings yet
- Assessment of Chronic PainDocument7 pagesAssessment of Chronic PainFranciscoGarciaNo ratings yet
- Profile of Craniomandibular Disorders subjects with concomitant occipital neuralgia regarding previous consultations and use of medicationDocument7 pagesProfile of Craniomandibular Disorders subjects with concomitant occipital neuralgia regarding previous consultations and use of medicationomar franklin molina tinocoNo ratings yet
- Afzal Et Al Int. J. Med. Appl. Health. Vol. 4, No. 2, 2016Document2 pagesAfzal Et Al Int. J. Med. Appl. Health. Vol. 4, No. 2, 2016RenaldiPrimaSaputraNo ratings yet
- Systematic Review of Diagnostic Utility and Therapeutic Effectiveness of Cervical Facet Joint InterventionsDocument23 pagesSystematic Review of Diagnostic Utility and Therapeutic Effectiveness of Cervical Facet Joint InterventionsJaviMéndezNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument5 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- Journal Homepage: - : IntroductionDocument5 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Effectiveness of Isometric Neck Exercises, Stretching and Ergonomics Over Ergonomic Alone For Neck Pain in PhysiotherapistsDocument6 pagesEffectiveness of Isometric Neck Exercises, Stretching and Ergonomics Over Ergonomic Alone For Neck Pain in PhysiotherapistsAndi Riska AmirullahNo ratings yet
- Cervical Proprioception Impairment in Neck Pain-Pathophysiology, Clinical Evaluation, and Management: A Narrative ReviewDocument22 pagesCervical Proprioception Impairment in Neck Pain-Pathophysiology, Clinical Evaluation, and Management: A Narrative ReviewsoylahijadeunvampiroNo ratings yet
- Cervicogenic Headache BasicDocument2 pagesCervicogenic Headache BasicpervinkumarNo ratings yet
- None 2Document9 pagesNone 2Alfina RahmiNo ratings yet
- PDF AlgologiaDocument11 pagesPDF AlgologiaThamires BritoNo ratings yet
- Va Medica: Effects of Myofascial Technique in Patients With Subacute Whiplash Associated Disorders: A Pilot StudyDocument0 pagesVa Medica: Effects of Myofascial Technique in Patients With Subacute Whiplash Associated Disorders: A Pilot StudyKaren Jeanette Valderrama CortesNo ratings yet
- Rana2013 2Document14 pagesRana2013 2Shaun TylerNo ratings yet
- Thoracic Spine Manipulation For The Management of Mechanical Neck Pain: A Systematic Review and Meta-AnalysisDocument28 pagesThoracic Spine Manipulation For The Management of Mechanical Neck Pain: A Systematic Review and Meta-AnalysisskNo ratings yet
- 1 s2.0 S1413355523000163 MainDocument12 pages1 s2.0 S1413355523000163 Maincarlosso16hotmail.comNo ratings yet
- Musculoskeletal Science and PracticeDocument11 pagesMusculoskeletal Science and PracticeAnii warikarNo ratings yet
- Effectiveness of Manual Traction and Other Physiotherapy Treatment in The Management of Painful Cervical RadiculopathyDocument5 pagesEffectiveness of Manual Traction and Other Physiotherapy Treatment in The Management of Painful Cervical RadiculopathyAgus Dwiyana NMNo ratings yet
- Jer 16 6 516Document6 pagesJer 16 6 516cris.endo.ceNo ratings yet
- Low Back Pain and Muscles ActivityDocument7 pagesLow Back Pain and Muscles Activitycris.endo.ceNo ratings yet
- 2021 Article 4080Document9 pages2021 Article 4080cris.endo.ceNo ratings yet
- Iastm ReviewDocument14 pagesIastm Reviewcris.endo.ceNo ratings yet
- Bevilaqua-Grossi Et Al. 2010 CephalalgiaDocument8 pagesBevilaqua-Grossi Et Al. 2010 Cephalalgiacris.endo.ceNo ratings yet
- Sentence Combining 1 - Copy 1Document2 pagesSentence Combining 1 - Copy 1haneen saqerNo ratings yet
- MIDAS QuestionnaireDocument1 pageMIDAS QuestionnaireNHFChicagoNo ratings yet
- Section 16: Additional Information: Health Hazard 3 Fire Hazard 1Document1 pageSection 16: Additional Information: Health Hazard 3 Fire Hazard 1johnNo ratings yet
- Essential Attitudes, Personal Qualities, and Professional Behaviors Required in NursingDocument27 pagesEssential Attitudes, Personal Qualities, and Professional Behaviors Required in NursingshirleyNo ratings yet
- Concept Map - SepsisDocument9 pagesConcept Map - SepsismarkyabresNo ratings yet
- English Assignment Direct and Indirect SentencesDocument6 pagesEnglish Assignment Direct and Indirect SentencesSasmita Novalis ArrizqiNo ratings yet
- Opscom AugustDocument19 pagesOpscom AugustMichelle Motin ToledoNo ratings yet
- Nursing Leadership Roles ResponsibilitiesDocument2 pagesNursing Leadership Roles ResponsibilitiesDan Dan ManaoisNo ratings yet
- Tutorial 1A - Public HealthDocument22 pagesTutorial 1A - Public Healthmuhammad saufi sulaimanNo ratings yet
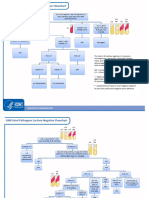
- GNR Stool Pathogens Lactose Negative FlowchartDocument2 pagesGNR Stool Pathogens Lactose Negative FlowchartKeithNo ratings yet
- Ecological Systems Theory by Bronfenbrenner: Prepared By: Karen B. Reginaldo Jung PuertoDocument20 pagesEcological Systems Theory by Bronfenbrenner: Prepared By: Karen B. Reginaldo Jung Puertochristian ferrerNo ratings yet
- Meningioma Review of Epidemiology, Pathology, Diagnosis and TreatmentDocument15 pagesMeningioma Review of Epidemiology, Pathology, Diagnosis and Treatmentwibawa suryaNo ratings yet
- STIKES English ClassDocument9 pagesSTIKES English ClassAnggun suriNo ratings yet
- Madre de Cacao With Lemon Scent As Hand Sanitizer: By: Johnro P. LustadoDocument20 pagesMadre de Cacao With Lemon Scent As Hand Sanitizer: By: Johnro P. LustadoJamailla MelendrezNo ratings yet
- MCN ReviewerDocument3 pagesMCN ReviewerJunghoon YangParkNo ratings yet
- Hospital departments, medical terms, and anatomyDocument18 pagesHospital departments, medical terms, and anatomyThanh ToànNo ratings yet
- Narrative ReportDocument2 pagesNarrative ReportRhisia RaborNo ratings yet
- ABP - MPDO Lakkireddy Palli Mandal Approved LetterDocument3 pagesABP - MPDO Lakkireddy Palli Mandal Approved Letterchild development project officer lakkireddypalliNo ratings yet
- Misrak FeyissaDocument41 pagesMisrak FeyissaN SNo ratings yet
- UCT Postgraduate-Studies BrochureDocument27 pagesUCT Postgraduate-Studies BrochureUsman AhmedNo ratings yet
- MSDS DDDocument2 pagesMSDS DDBaher SaidNo ratings yet