Professional Documents
Culture Documents
Genetic Myelopathies.8
Uploaded by
Mayra AldecoaOriginal Description:
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Genetic Myelopathies.8
Uploaded by
Mayra AldecoaCopyright:
Available Formats
Genetic Myelopathies REVIEW ARTICLE
By Kara Stavros, MD, FAAN C O N T I N U UM A U D I O
I NT E R V I E W A V A I L AB L E
ONLINE
Downloaded from http://journals.lww.com/continuum by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCyw
ABSTRACT
OBJECTIVE: This article provides an overview of genetic myelopathies, a
CX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC4/OAVpDDa8K2+Ya6H515kE= on 02/16/2024
diverse group of inherited, degenerative conditions that may be broadly
categorized as motor neuron disorders, disorders of spinocerebellar
degeneration, leukodystrophies, and hereditary spastic paraplegia.
Clinical examples from each category are provided to illustrate the
spectrum of genetic myelopathies and their distinguishing features that aid
in differentiating genetic myelopathies from potentially treatable acquired
causes of myelopathy.
LATEST DEVELOPMENTS: Advances in genetic testing have vastly enhanced
current knowledge of genetic myelopathies and the ability to diagnose and
provide appropriate counseling to patients and their families. However,
potential health care disparities in access to genetic testing is a topic that
must be further explored. Although treatment for most of these conditions
is typically supportive, there have been recent therapeutic breakthroughs
in treatments for amyotrophic lateral sclerosis, spinal muscular atrophy,
and Friedreich ataxia.
Genetic myelopathies may present with chronic and
ESSENTIAL POINTS:
progressive symptoms, a family history of similar symptoms, and
involvement of other structures outside of the spinal cord. Imaging often
shows spinal cord atrophy, but cord signal change is rare. Exclusion of
reversible causes of myelopathy is a key step in the diagnosis. There are
many different causes of genetic myelopathies, and in some cases,
symptoms may overlap, which underscores the utility of genetic testing in
CITE AS:
confirming the precise underlying neurologic condition. CONTINUUM (MINNEAP MINN)
2024;30(1, SPINAL CORD
DISORDERS):119–132.
Address correspondence to
Dr Kara Stavros, 593 Eddy St,
APC 5, Providence, RI 02903,
INTRODUCTION Kara_stavros1@brown.edu.
G
enetic myelopathies encompass a wide range of inherited, RELATIONSHIP DISCLOSURE:
degenerative neurologic disorders. Advances in genetics have Dr Stavros reports no
identified a growing array of genes associated with genetic disclosure.
myelopathies, providing a greater understanding of the breadth UNLABELED USE OF
and pathophysiology of these conditions, facilitating greater PRODUCTS/INVESTIGATIONAL
USE DISCLOSURE:
diagnostic closure for patients, and identifying potential targets for future
Dr Stavros reports no
therapeutics. In this article, the range of genetic causes of myelopathy is disclosure.
considered in four broad categories, with specific examples provided in each
category: (1) hereditary spastic paraplegia (HSP), (2) motor neuron disorders, © 2024 American Academy
(3) leukodystrophies, and (4) spinocerebellar degeneration. of Neurology.
CONTINUUMJOURNAL.COM 119
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
GENETIC MYELOPATHIES
GENERAL APPROACH TO PATIENTS WITH SUSPECTED GENETIC
MYELOPATHY
It is important to consider an inherited cause of myelopathy in the differential
diagnosis for patients presenting with myelopathic symptoms and, conversely, to
consider spinal cord involvement in patients known to have certain
neurodegenerative conditions. Clinical symptoms of myelopathy due to a genetic
Downloaded from http://journals.lww.com/continuum by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCyw
cause are similar to those in patients with chronic myelopathy from other causes.
Presentations typically include a variable combination of motor and sensory
deficits, spasticity, hyperreflexia, and bladder symptoms. The age of onset of
CX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC4/OAVpDDa8K2+Ya6H515kE= on 02/16/2024
symptoms may be variable because genetic myelopathies can present across the
lifespan from infancy to adulthood, but the time course is typically chronic and
slowly progressive. In genetic myelopathies, other manifestations of the
underlying disorder outside of the spinal cord may be detected by history or
clinical examination (TABLE 5-1). However, there are some exceptions; for
example, patients with HSP may present with predominantly myelopathic
symptoms without significant systemic features.1,2
Assessment of a patient with a suspected genetic cause of myelopathy requires
obtaining a detailed family history to probe for relatives with similar symptoms.
However, it should be noted that a negative family history does not exclude the
possibility of a genetic cause. Family history may be unrevealing for a variety of
reasons, such as cases of de novo genetic variations, variable penetrance and
phenotypes within the same family, autosomal recessive inheritance, or a
patient’s lack of knowledge of family members’ medical histories.3
Evaluation of a suspected genetic myelopathy should always include testing to
exclude acquired and potentially treatable causes of myelopathy, such as
structural, nutritional, vascular, or demyelinating etiologies. This may include
neuroimaging of the brain and spinal cord, as well as laboratory studies or nerve
conduction studies and EMG. In patients with genetic myelopathies, MRI of the
spinal cord may be normal or may show spinal cord atrophy without signal
TABLE 5-1 Extraspinal Symptoms in Selected Genetic Myelopathies
Genetic myelopathy Extraspinal symptoms
Familial amyotrophic Pseudobulbar affect, cognitive impairment, dementia
lateral sclerosis
Spinobulbar muscular Gynecomastia, infertility, testicular atrophy, diabetes,
atrophy sensory neuropathy
Hereditary spastic Numerous phenotypes; may include cognitive changes,
paraparesis extrapyramidal symptoms, seizures, hearing loss, optic
atrophy, ataxia, dysarthria
Hexosaminidase A Cerebellar atrophy, ataxia, dysarthria, dysphagia,
deficiency psychiatric symptoms
Adrenomyeloneuropathy Adrenal insufficiency, cognitive changes, peripheral
neuropathy
Friedreich ataxia Optic atrophy, hearing loss, hypertrophic cardiomyopathy,
ataxia, dysphagia, nystagmus, scoliosis, dysarthria,
peripheral neuropathy
120 F E B R U A R Y 2 0 24
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
change. It is rare for MRI to show signal change in the spinal cord in these cases; KEY POINTS
there are some exceptions, including several of the genetic leukodystrophies, but
● Genetic myelopathies
in these patients, there is usually concomitant cerebral involvement.4 Diagnostic often manifest with other
testing not only excludes acquired causes of myelopathy but may offer clues as to systemic signs or symptoms
the underlying inherited condition. associated with the
myelopathy, and these may
Downloaded from http://journals.lww.com/continuum by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCyw
be clues to the diagnosis.
GENETIC TESTING
Genetic testing can help confirm the diagnosis once the initial diagnostic workup ● On neurologic history,
is performed to exclude acquired causes and narrow the differential diagnosis.
CX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC4/OAVpDDa8K2+Ya6H515kE= on 02/16/2024
suspicion for genetic
Genetic testing plays an important role in making a final diagnosis, particularly myelopathy may be raised if
because many of the clinical symptoms may overlap in different genetic there is a slow progression
of symptoms and a family
conditions. There are no clinical guidelines providing recommendations for history of similar symptoms.
when and how to pursue genetic testing in genetic myelopathies, but testing However, a negative family
should always be carefully considered and the potential disadvantages and history does not exclude a
benefits explored. Options may include testing a panel of genes targeted to the genetic cause.
suspected condition or whole-exome sequencing. Whole-exome sequencing ● Evaluation for a genetic
diagnostic yield is highly variable but may identify a specific diagnosis in myelopathy should always
neurogenetic conditions at a rate of approximately 30%.5,6 Whole-exome include testing to rule out
sequencing may be less sensitive in detecting gene deletions or duplications. potentially reversible
causes of myelopathy.
Current understanding of the genes implicated in genetic myelopathies has
steadily advanced, but it is still an evolving landscape. Results of testing can at ● In genetic myelopathies,
times be inconclusive or falsely negative because many of the genetic variations MRI of the spine most
that underlie these disorders have yet to be identified; therefore, a negative test commonly shows spinal
result does not definitively exclude a potential genetic etiology. Interpretation of cord atrophy without signal
change.
variants of uncertain significance is a persistent challenge. Another limitation of
genetic testing may be the cost, although free sponsored testing may be available ● Barriers to access to
in some cases from nonprofit organizations or pharmaceutical companies. genetic testing exist,
Additionally, health care disparities exist regarding ensuring equitable access to including cost, location, lack
of awareness, and distrust.
genetic testing; some patients may have limited access because of location,
socioeconomic factors, a lack of awareness, or distrust of how their medical ● Genetic testing should be
information will be used.7-9 performed by a physician
Genetic testing should be ordered and reviewed always by a physician who has with expertise in counseling
patients and their families,
the expertise and resources to counsel patients and their families on the results
and coordination of care
regardless of whether they are positive, negative, or inconclusive. Coordination with a medical geneticist
of care with a medical geneticist and genetic counselor is extremely beneficial. may be beneficial.
HEREDITARY SPASTIC PARAPLEGIA
HSP comprises a large group of disorders characterized by degeneration of the
corticospinal tracts and dorsal column tracts and classically presents with
progressive spasticity, weakness in the lower extremities, and hyperreflexia,
typically with sensory deficits and bladder involvement. This clinical
presentation is further illustrated in CASE 5-1. In the realm of genetic
myelopathies, HSP may be variably characterized as a motor neuron disorder or a
distal motor-sensory axonopathy. Onset may occur during childhood or
adulthood, and many associated symptoms have been described in different
genotypes and phenotypes of HSP, including neuropathy, cognitive changes,
extrapyramidal symptoms, hearing loss, seizures, optic atrophy, ataxia, and
dysarthria among others.2 HSP may be classified as complicated when associated
with these additional neurologic or systemic findings, as opposed to what may
variably be referred to as the pure, simple, or uncomplicated form presenting
CONTINUUMJOURNAL.COM 121
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
GENETIC MYELOPATHIES
predominantly with weakness and spasticity. These classifications do not reflect
the wide variability in genotypic-phenotypic correlation that may be seen; for
example, patients with genetic variations typically associated with
uncomplicated HSP may present with other systemic manifestations, and
conversely, patients with genetic variations typically associated with complicated
HSP may have relatively few systemic manifestations.10,11
Downloaded from http://journals.lww.com/continuum by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCyw
The inheritance pattern of HSP can be autosomal recessive, autosomal
dominant, or X-linked. To date, more than 79 genes have been implicated in
HSP,11 and this heterogeneity in genotype as well as phenotype contributes to the
CX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC4/OAVpDDa8K2+Ya6H515kE= on 02/16/2024
challenges in both diagnosis and development of therapeutic advances for this
disorder. The most frequent type of autosomal dominant HSP is caused by a
variation in the SPG4 gene, which encodes the spastin protein. Several different
SPG4 variations have been observed, including missense, frameshift, deletions,
and nonsense variants, all resulting in a reduction in the spastin protein, which
plays a role in microtubule function.11 The specific type of genetic variation may
be associated with the age of onset of symptoms because age of onset is highly
variable, ranging from infancy through late adulthood. This type of HSP typically
presents with a phenotype characterized by weakness and spasticity, although
there have been reports of patients with cognitive impairment, ataxia, and
thinning of the corpus callosum.10
Variants in SPG11 are the most common autosomal recessive form of HSP,
impacting the spatacsin protein, which is involved in lysosome recycling and
clearance of gangliosides.11 This form of HSP typically presents early in childhood
or adolescence, and it may be associated with other neurologic and systemic
symptoms, including cognitive impairment, ataxia, neuropathy, and retinal
CASE 5-1 A 33-year-old man presented to the neurology clinic with symptoms of
gradually progressive lower extremity spasticity over the past several
years. He reported a family history of similar symptoms in his father who
had leg stiffness and trouble walking, and more recently a younger sibling
started to notice similar symptoms. He has no symptoms in his arms. On
neurologic examination, he has spasticity in both lower extremities
without any other neurologic abnormalities. MRI of his brain and entire
spine was unremarkable. Serum laboratory values for vitamin B12 and
copper were normal, human immunodeficiency virus (HIV) and human
T-cell lymphotropic virus type 1 (HTLV-1) tests were negative, and a
lumbar puncture showed no evidence of infection or inflammation.
COMMENT This patient’s clinical presentation raised concern for hereditary spastic
paraplegia, with hallmark features of bilateral lower extremity spasticity in
the setting of a family history of similar symptoms and exclusion of other
causes of myelopathy through imaging, serum, and CSF studies. The next
step is consultation with a geneticist and genetic counselor to discuss the
advantages and disadvantages of seeking genetic testing to confirm this
diagnosis for the patient and possibly his family members.
122 F E B R U A R Y 2 0 24
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
degeneration.11 Both SPG11 and KEY POINT
SPG15 variations have been
● The hereditary spastic
associated with thinning of the paraplegia inheritance
corpus callosum and a pattern may be autosomal
characteristic finding on MRI of dominant, autosomal
the brain wherein the forceps recessive, or X-linked, with
Downloaded from http://journals.lww.com/continuum by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCyw
significant genotypic and
minor of the corpus callosum
phenotypic heterogeneity.
appears bright on FLAIR images
and dark on T1-weighted
CX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC4/OAVpDDa8K2+Ya6H515kE= on 02/16/2024
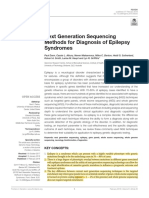
images.12 This is known as the
ears of the lynx sign, reminiscent
of the tufts of hair seen on the
pointed ears of the lynx wild cat
(FIGURE 5-1). Other notable gene
variations in HSP include SPG7,
which is autosomal recessive and
has been associated with
cerebellar ataxia, and SACS,
which is also autosomal recessive
and associated with FIGURE 5-1
11 Ears of the lynx on MRI. A, Axial MRIs from a
neuropathy.
patient with hereditary spastic paraplegia (HSP)
Although genotype-
due to SPG11 genetic variation show an
phenotype correlations are not abnormality in the corpus callosum (red arrows)
always straightforward in HSP,13 appearing dark on a T1-weighted image and bright
the pursuit of genetic diagnosis is on fluid-attenuated inversion recovery (FLAIR)
still important in guiding patient imaging. This is known as the ears of the lynx sign
and may be seen in SPG11 and SPG15 forms of HSP.
management, counseling, and Comparison to healthy control patients without
anticipation of any associated HSP is illustrated in the first and third images.
symptoms outside of the spinal B, Corresponding images of a lynx wild cat.
Reprinted with permission from Pascual B, et al, AJNR Am J
cord. Treatment is supportive,
Neuroradiol.12 © 2019 American Society of Neuroradiology.
consisting of pharmacologic
therapy for spasticity to increase
mobility and reduce discomfort as well as bracing and assistive devices as
indicated. Systemic symptoms such as fatigue, sphincter dysfunction, and others
should also be addressed and often require multidisciplinary care.
MOTOR NEURON DISORDERS
Motor neuron disorders may be caused by dysfunction of the lower motor
neurons, corticospinal tracts, or both and may be either inherited or acquired.
Patients can present with lower motor neuron signs such as fasciculations,
hyporeflexia, or atrophy and upper motor neuron signs such as increased tone,
hyperreflexia, or positive plantar reflexes (the Babinski sign). This section
focuses on two examples of inherited motor neuron disorders: amyotrophic
lateral sclerosis (ALS) and spinal muscular atrophy (SMA).
Inherited Amyotrophic Lateral Sclerosis
While ALS is not conventionally considered a myelopathy, the spinal cord is one
site of the pathophysiology of this disease, and patients with ALS may present
with clinical features similar to myelopathy (especially with lower limb–onset
disease). ALS often presents with bulbar or limb onset of symptoms and a
CONTINUUMJOURNAL.COM 123
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
GENETIC MYELOPATHIES
combination of both upper and lower motor neuron signs. Associated symptoms
may also include cognitive impairment that varies in severity but may meet the
criteria for frontotemporal dementia in some cases.14 Patients may also
experience pseudobulbar affect, a dysregulation of motor output of emotion that
is difficult to localize anatomically but may involve more widely dispersed
networks.15,16 ALS is most commonly sporadic; however, approximately 10% to
Downloaded from http://journals.lww.com/continuum by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCyw
15% of cases of ALS are familial,17,18 with speculation that this range could
underestimate the true prevalence of inherited ALS because of factors such as
incomplete knowledge of family history or low-penetrance genetic variations.17
CX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC4/OAVpDDa8K2+Ya6H515kE= on 02/16/2024
So far, more than 50 genes have been implicated in familial ALS, with the most
common being C9orf72, which has a notable association with frontotemporal
dementia.14 The mechanism by which variations in C9orf72 cause disease is still
being elucidated.19 Other notable genes implicated in familial ALS include SOD1,
TDP-43, and FUS.17,18,20
The diagnosis of familial ALS, like acquired ALS, is based on history and
neurologic examination coupled with nerve conduction studies and EMG
suggestive of a motor neuron disorder and exclusion of other possible diagnoses
through additional testing as indicated by each patient’s presentation. There may
be a family history of ALS that prompts the patient’s evaluation. The clinical
symptoms of familial ALS may be clinically indistinguishable from sporadic ALS,
although the average age of onset of ALS symptoms in patients with familial ALS
is approximately 5 years younger than for nongenetic, sporadic ALS.21
Studies show that patients are generally favorable to genetic testing in ALS and
view it as beneficial, although access to testing and awareness may be limited,
and among presymptomatic individuals, 60% of patients would choose to get
tested.22-24 The ethical implications of performing genetic testing on
presymptomatic family members should be carefully considered. Any discussion
should be undertaken with the goal of better informing the patient and include
consideration of the disadvantages versus benefits of pursuing this testing.25
Recommendations for the principles and practice of presymptomatic genetic
testing for ALS are available for guidance.26
Currently, the treatment for ALS, whether familial or sporadic, is centered on
symptomatic care and four US Food and Drug Administration (FDA)–approved
medications that may modestly delay progression of the disease. These include
riluzole, edaravone,27 combination sodium phenylbutyrate and taurursodiol,28
and tofersen.29 Toferson is indicated only for patients with ALS caused by
variations in SOD1.
Spinal Muscular Atrophy
SMA is an autosomal recessive, lower motor neuron disorder that encompasses a
spectrum of clinical phenotypes that are separated by age of onset and degree of
weakness.30 It is caused by variations in the SMN1 gene, resulting in reduced
expression of the survival motor neuron protein and leading to loss of anterior
horn cells.31 Infantile-onset forms are severe, with patients demonstrating
profound hypotonia and progressive respiratory and swallowing difficulties. Left
untreated, the infantile-onset forms of SMA are usually fatal before the age of
2 years.32 Symptoms are relatively milder in later-onset forms but still include a
slow progression of weakness impacting mobility and gait with more severe
phenotypes and poorer prognosis associated with an earlier age of onset. Genetic
testing typically confirms the diagnosis. In patients presenting later in life, nerve
124 F E B R U A R Y 2 0 24
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
conduction studies and EMG may also provide important clues in narrowing the KEY POINTS
differential diagnosis.
● The most common
The mainstays of treatment were previously supportive in nature and genetic variation implicated
comprised physical therapy, orthopedic management, and respiratory care. in inherited forms of
However, in recent years treatments with novel mechanisms of action have amyotrophic lateral
been developed that increase the expression of the survival motor neuron sclerosis is in the C9orf72
Downloaded from http://journals.lww.com/continuum by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCyw
gene.
protein. These treatments include an antisense oligonucleotide, nusinersen;
a small molecule splicing modifier, risdiplam; and gene therapy with ● Presymptomatic genetic
onasemnogene abeparvovec-xioi.33-35 These treatments are quickly becoming
CX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC4/OAVpDDa8K2+Ya6H515kE= on 02/16/2024
testing for amyotrophic
routine components of care for early-onset SMA. The advent of these new lateral sclerosis in a patient
therapies has led to the consideration of new SMA phenotypes and redefinition with a known family history
should be undertaken with
of the natural history of this condition.31 These treatment options underscore caution and with reference
the need to diagnose and treat patients as soon as possible to prevent more to available practice
severe disease manifestations and has led to a call for increased newborn principles.
screening for SMA.36 Issues of cost and insurance coverage for these new
● Several disease-
medications and access for patients with later-onset forms of SMA may create modifying medications with
socioeconomic health care disparities.37 novel mechanisms of action
for the treatment of spinal
Other Hereditary Motor Neuron Disorders muscular atrophy have
become integrated into
Numerous other disorders affecting the motor neurons fall on the spectrum of
routine practice and are
genetic myelopathy. Inherited forms of primary lateral sclerosis, a demonstrating improved
predominantly upper motor neuron syndrome, are very rare but have been patient outcomes.
described.38 Primary lateral sclerosis presents at a mean age of 50 years old with
upper motor neuron–predominant symptoms including stiffness, corticobulbar ● Hallmark clinical features
of spinal bulbar muscular
dysfunction, and reduced mobility.39 atrophy (Kennedy disease)
Hexosaminidase A deficiency is a rare cause of lower motor neuron include limb and bulbar
dysfunction, presenting with symptoms of limb muscle weakness and atrophy, weakness, atrophy, facial
and may be associated with dysphagia and dysarthria.40 The disorder is fasciculations, and
gynecomastia.
caused by a variation in the HEXA gene. The infantile form results in a more
severe presentation of Tay-Sachs disease, whereas the adult-onset form presents ● Workup for
with a more variable phenotype and better prognosis. Adult onset of adrenomyeloneuropathy
hexosaminidase A deficiency has also been associated with syndromes of may include testing of
adrenal function, evaluation
cerebellar ataxia and cerebellar atrophy on neuroimaging, as well as
for elevation in very long
psychiatric symptoms.40 chain fatty acids in the
Spinal bulbar muscular atrophy, or Kennedy disease, is inherited in an serum, and genetic testing
X-linked recessive pattern associated with a CAG repeat expansion in the for pathogenic variants in
the ABCD1 gene on the X
androgen receptor gene AR. Patients with spinal bulbar muscular atrophy
chromosome.
typically present in the third to seventh decades of life and may report symptoms
of muscle atrophy, weakness in the bulbar and limb muscles, sensory ● Friedreich ataxia presents
neuropathy, and perioral facial fasciculations.41 Non-neurologic hallmarks of this with symptoms of ataxia,
syndrome are gynecomastia and reduced fertility. The diagnosis is confirmed by neuropathy, and upper
motor neuron signs. Patients
genetic testing. CASE 5-2 illustrates a patient presenting to a neurology clinic with are at risk for
spinal bulbar muscular atrophy. cardiomyopathy and must
undergo cardiac evaluation.
LEUKODYSTROPHIES
Many of the leukodystrophies present predominantly with cerebral symptoms;
however, several leukodystrophies may be associated with myelopathic
features in addition to cerebral involvement. This section highlights
adrenomyeloneuropathy and adult polyglucosan body disease as two examples
of leukodystrophies with myelopathic involvement.
CONTINUUMJOURNAL.COM 125
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
GENETIC MYELOPATHIES
X-linked Adrenoleukodystrophy and Adrenomyeloneuropathy
Adrenoleukodystrophy and adrenomyeloneuropathy are X-linked conditions
caused by a variation on the ABCD1 gene that encodes a peroxisomal
transmembrane protein, leading to accumulation of very long chain fatty acids.
In adrenoleukodystrophy, symptoms manifest in boys during childhood, with
symptoms of cognitive changes, optic atrophy, hearing loss, seizures, and
Downloaded from http://journals.lww.com/continuum by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCyw
spasticity, as well as adrenal insufficiency.42 As demonstrated in CASE 5-3, the
adrenomyeloneuropathy phenotype typically presents in the third to fifth
decades of life with progressive spastic paraparesis and peripheral neuropathy.
CX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC4/OAVpDDa8K2+Ya6H515kE= on 02/16/2024
Adrenal insufficiency is evident in most patients with
adrenomyeloneuropathy, and cognitive changes may develop in some patients
later in the disease course. Recognition of cerebral complications in patients with
adrenomyeloneuropathy is increasing, with 60% of patients with
adrenomyeloneuropathy found to develop cerebral demyelination, which is
associated with rapid progression and poor survival.43 Female carriers can rarely
develop symptoms, such as progressive myelopathy later in life.44,45 The
diagnosis may be made by genetic testing; however, a finding of elevated very
long chain fatty acid levels on laboratory evaluation is also key. Patients may also
have laboratory evidence of adrenal insufficiency, providing additional clues to
the diagnosis.
Adrenal insufficiency may be treated with replacement therapy, and other
adrenomyeloneuropathy symptoms may be addressed with supportive therapies
for pain and spasticity to enhance functional ability and quality of life, often
CASE 5-2 A 44-year-old man presented to the clinic for evaluation of proximal
muscle weakness, including difficulty raising his arms and trouble
climbing stairs. He also reported that he had noticed muscle twitches in
his body and face over the past few years, which he mostly ignored, but it
could sometimes cause him to feel self-conscious. He described a family
history of symptoms of weakness and trouble walking on his mother’s
side. Neurologic examination demonstrated proximal muscle weakness
with 4/5 strength in shoulder abduction and hip flexion, associated
muscle atrophy in his shoulder girdle and hip girdle muscles, diffuse
hyporeflexia, rare fasciculations in the perioral area, and evidence of
gynecomastia. His electrodiagnostic evaluation demonstrated a
widespread, chronic disorder of motor neurons with a mild superimposed
sensory neuropathy.
COMMENT This patient presented with a clinical picture suggestive of spinal bulbar
muscular atrophy, or Kennedy disease. If the patient consents, genetic
testing would help confirm this diagnosis. There currently are no
disease-modifying treatments for this disorder, but he could benefit from
physical therapy and consideration of an assistive device for greater safety
during ambulation. He should be screened for any bulbar weakness
affecting his speech, chewing, or swallowing that might require further
assessment.
126 F E B R U A R Y 2 0 24
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
benefitting from a multidisciplinary approach.46 There are currently no proven
disease-modifying therapies for the neurologic manifestations in patients with
adult-onset disease.42,45 Leriglitazone is a selective peroxisome proliferator-
activated receptor gamma agonist implicated in neuroinflammation and
degeneration, and although a recent trial of leriglitazone did not demonstrate
efficacy, other potential targeted therapies may follow.47
Downloaded from http://journals.lww.com/continuum by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCyw
Other Leukodystrophies
Other leukodystrophies that may involve the spinal cord include Alexander
CX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC4/OAVpDDa8K2+Ya6H515kE= on 02/16/2024
disease (GFAP), leukoencephalopathy with brainstem and spinal cord
involvement and lactate elevation (DARS2), and adult polyglucosan body disease
(GBE1).4,42,48 Adult polyglucosan body disease is an autosomal recessive
condition resulting from a variation in the GBE1 gene, which causes a deficiency
in glycogen-debranching enzyme and storage of polyglucosan bodies.49 This
disorder may be underrecognized and can manifest with a variety of clinical
phenotypes, typically presenting in adults in the fourth to seventh decades with
slowly progressive weakness, spasticity, bulbar symptoms, neurogenic bladder,
and neuropathy.49 Cognitive symptoms such as impairment in memory and
executive function have also been described,50 and brain imaging may reveal
cerebral and cerebellar atrophy and diffuse leukoencephalopathy.49 Spinal
imaging may show medullary and spinal cord atrophy without signal change
A 40-year-old man presented to the clinic with progressive neurologic CASE 5-3
symptoms spanning many years. He could not recall any symptoms in his
childhood or adolescence but said that in his early twenties, he started to
notice numbness and tingling in his feet and poor balance. This gradually
worsened over the past few years, and he started using a cane to walk.
He also reported some progressive issues emptying his bladder, and he
had to start doing self-catheterization. His past medical history was
notable for multiple hospital admissions for hypotension and
hypoglycemia, requiring steroids. He did not have a close relationship
with his mother but could recall that she had trouble walking. On
examination, he had normal strength and tone in both legs but
hyperreflexia and an abnormal plantar reflex. Sensation to vibration was
reduced distally in his lower extremities on both sides. MRI of his brain
and entire spinal cord was normal.
This patient’s symptoms raise concern for adrenomyeloneuropathy. He COMMENT
can be further evaluated for this by serum testing for elevation in very long
chain fatty acids and through genetic testing. His history of hypotension
and hypoglycemia may be indicative of adrenal dysfunction, and
consultation with an endocrinology specialist may be warranted. Although
there are no effective disease-modifying treatments for adult-onset
disease at this time, he may benefit from physical therapy, counseling on
fall risk, and optimization of home safety and assistive devices.
CONTINUUMJOURNAL.COM 127
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
GENETIC MYELOPATHIES
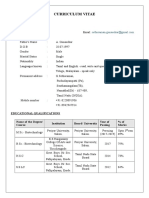
(FIGURE 5-2).4,49 There are no
disease-modifying treatments
available for adult polyglucosan
body disease at present, and the
mainstay of treatment
is supportive.
Downloaded from http://journals.lww.com/continuum by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCyw
SPINOCEREBELLAR
DEGENERATION
CX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC4/OAVpDDa8K2+Ya6H515kE= on 02/16/2024
The hereditary ataxias are a
widely diverse group of inherited
disorders that can involve
progressive ataxia, dorsal column
impairment, and corticospinal
FIGURE 5-2 tract degeneration to varying
Sagittal T2-weighted MRI of the cervical spine in a degrees.
patient with adult polyglucosan body disease
demonstrates severe spinal cord atrophy without
signal change.
Figure courtesy of Shamik Bhattacharyya, MD, FAAN.
CASE 5-4 A 54-year-old woman was referred to the clinic for evaluation of ataxia.
She said that her symptoms started about 8 years ago and had been slowly
worsening over time. She reported weakness in both legs, intermittent
dizziness, and trouble with balance. She had been using a walker for the
past year, and she had several falls. She recalled that she was diagnosed
with a degenerative neurologic condition in the past but didn’t recall if a
specific diagnosis was made. She reported that past nerve conduction
studies and EMG, lumbar puncture, and MRI of her brain and spine were
normal. Of note, she reported that she was currently undergoing a cardiac
workup because of symptoms of leg swelling and fatigue. On neurologic
examination, she had intact strength in all limbs, reduced vibration and
joint position sensation in her toes, hyperreflexia, and marked dysmetria
on finger-to-nose testing on both sides. Her rapid alternating movements
were slow and clumsy. Her gait was slow, wide-based, and cautious.
Her laboratory workup was unremarkable. An echocardiogram
showed evidence of cardiomyopathy. Repeated nerve conduction
studies and EMG and MRI of her brain and spine were unrevealing. She
was referred to a genetics clinic for further evaluation for a suspected
inherited cause of ataxia. Genetic testing demonstrated a pathogenic
GAA repeat expansion in the FXN gene (repeat number 144 in both
alleles), consistent with Friedreich ataxia.
COMMENT This patient presented with a late onset of Friedreich ataxia, which was
confirmed by genetic testing. Although Friedreich ataxia typically presents
during childhood or adolescence, later-onset forms may be seen and are
important to consider. Hypertrophic cardiomyopathy is an important
associated feature of the disorder.
128 F E B R U A R Y 2 0 24
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Friedreich Ataxia
Friedreich ataxia is autosomal recessive, caused by an expanded GAA
trinucleotide repeat in the FXN gene. Friedreich ataxia typically presents in
childhood or adolescence with symptoms of ataxia, neuropathy, and upper
motor neuron findings. Other symptoms may include dysarthria, optic atrophy,
hearing loss, and cardiomyopathy. Late-onset forms in adulthood, as shown in
Downloaded from http://journals.lww.com/continuum by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCyw
CASE 5-4, have also been described. In the case of late-onset Friedreich ataxia,
symptoms may be atypical and can be characterized by retained reflexes, lack of
dysarthria, lack of systemic signs, or slower overall progression.51
CX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC4/OAVpDDa8K2+Ya6H515kE= on 02/16/2024
Patients with Friedreich ataxia benefit from a multidisciplinary care team,
including a cardiologist to monitor cardiac complications, to address the
numerous associated symptoms. Until recently, there were no specific
disease-modifying treatments available for Friedreich ataxia.52 The first
treatment for Friedreich ataxia was approved by the FDA in 2023 after
omaveloxolone, which acts to restore mitochondrial function, demonstrated a
benefit in the disease course and progression in randomized trials.53
Other Hereditary Ataxias
There are more than 40 different types of spinocerebellar ataxias, not all of which
have predominant spinal cord involvement. Spinocerebellar ataxia type 1 and
spinocerebellar ataxia type 3 (Machado-Joseph disease) may include symptoms
of spasticity and involve a CAG repeat in the ATXN1 and ATXN3 genes,
respectively.54,55 Ataxia and spinal cord involvement have also been reported in
abetalipoproteinemia and ataxia with isolated vitamin E deficiency.48
CONCLUSION
Genetic myelopathies comprise a large and diverse group of neurologic disorders.
Key features that may help distinguish a potential genetic myelopathy from an
acquired cause include a family history of similar neurologic symptoms, chronic
or slow progression over time, and the presence of additional symptoms not
strictly isolated to the spinal cord. In general, imaging typically shows spinal cord
atrophy without signal change. Genetic testing capabilities have expanded to
identify more genes implicated in these disorders than ever before but is still an
area in which knowledge is continuing to evolve. Few treatments are available for
any of the genetic myelopathies; however, in recent years new disease-modifying
treatments have become available for SMA, ALS, and Friedreich ataxia.
USEFUL WEBSITES
Brain & Life National Ataxia Foundation
The Brain & Life website offers patient education Patients with ataxia, including spinocerebellar ataxia
materials on several inherited myelopathies, and Friedreich ataxia, may find helpful resources on
including ALS, SMA, HSP, and Friedreich ataxia. the National Ataxia Foundation website.
brainandlife.org ataxia.org
Spastic Paraplegia Foundation
Further information and resources for patients with
HSP and primary lateral sclerosis can be found on
the website of the Spastic Paraplegia Foundation.
sp-foundation.org
CONTINUUMJOURNAL.COM 129
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
GENETIC MYELOPATHIES
REFERENCES
1 Shribman S, Reid E, Crosby AH, Houlden H, 13 Cunha IA, Ribeiro JA, Santos MC. Hereditary
Warner TT. Hereditary spastic paraplegia: from spastic paraparesis: the real-world experience
diagnosis to emerging therapeutic approaches. from a neurogenetics outpatient clinic. Eur J Med
Lancet Neurol 2019;18(12):1136-1146. doi:10.1016/ Genet 2022;65(3):104430. doi:10.1016/j.ejmg.
S1474-4422(19)30235-2 2022.104430
Downloaded from http://journals.lww.com/continuum by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCyw
2 McDermott C, White K, Bushby K, Shaw P. 14 Balendra R, Isaacs AM. C9orf72-mediated
Hereditary spastic paraparesis: a review of new ALS and FTD: multiple pathways to disease.
developments. J Neurol Neurosurg Psychiatry Nat Rev Neurol 2018;14(9):544-558. doi:10.1038/
CX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC4/OAVpDDa8K2+Ya6H515kE= on 02/16/2024
2000;69(2):150-160. doi:10.1136/jnnp.69.2.150 s41582-018-0047-2
3 Maas JW. Inherited myelopathies. Semin Neurol 15 Klingbeil J, Wawrzyniak M, Stockert A, et al.
2012;32(2):114-122. doi:10.1055/s-0032-1322581 Pathological laughter and crying: insights from
lesion network-symptom-mapping. Brain 2021;
4 Marelli C, Salsano E, Politi LS, Labauge P. Spinal
144(10):3264-3276. doi:10.1093/brain/awab224
cord involvement in adult-onset metabolic and
genetic diseases. J Neurol Neurosurg Psychiatry 16 Ghaffar O, Chamelian L, Feinstein A.
2019;90(2):211-218. doi:10.1136/jnnp-2018-318666 Neuroanatomy of pseudobulbar affect: a
quantitative MRI study in multiple sclerosis.
5 Guo MH, Bardakjian TM, Brzozowski MR, et al.
J Neurol 2008;255(3):406-412. doi:10.1007/s00415-
Temporal trends and yield of clinical diagnostic
008-0685-1
genetic testing in adult neurology. Am J Med
Genet A 2021;185(10):2922-2928. doi:10.1002/ 17 Feldman EL, Goutman SA, Petri S, et al.
ajmg.a.62372 Amyotrophic lateral sclerosis. Lancet Lond
Engl 2022;400(10360):1363-1380. doi:10.1016/
6 Córdoba M, Rodriguez-Quiroga SA, Vega PA,
S0140-6736(22)01272-7
et al. Whole exome sequencing in neurogenetic
odysseys: an effective, cost- and time-saving 18 Mejzini R, Flynn LL, Pitout IL, et al. ALS genetics,
diagnostic approach. PloS One 2018;13(2): mechanisms, and therapeutics: where are we
e0191228. doi:10.1371/journal.pone.0191228 now? Front Neurosci 2019;13:1310. doi:10.3389/
fnins.2019.01310
7 Saulsberry K, Terry SF. The need to build trust:
a perspective on disparities in genetic testing. 19 Taylor JP, Brown RH, Cleveland DW. Decoding
Genet Test Mol Biomark 2013;17(9):647-648. ALS: from genes to mechanism. Nature 2016;
doi:10.1089/gtmb.2013.1548 539(7628):197-206. doi:10.1038/nature20413
8 Suther S, Kiros GE. Barriers to the use of genetic 20 Al-Chalabi A, Hardiman O. The epidemiology of
testing: a study of racial and ethnic disparities. ALS: a conspiracy of genes, environment and
Genet Med Off J Am Coll Med Genet 2009;11(9): time. Nat Rev Neurol 2013;9(11):617-628.
655-662. doi:10.1097/GIM.0b013e3181ab22aa doi:10.1038/nrneurol.2013.203
9 National Academies of Sciences, Engineering, 21 Mehta PR, Jones AR, Opie-Martin S, et al.
and Medicine, Health and Medicine Division, Younger age of onset in familial amyotrophic
Board on Health Sciences Policy, Roundtable on lateral sclerosis is a result of pathogenic gene
Genomics and Precision Health. Exploring the variants, rather than ascertainment bias. J Neurol
barriers to accessing genomic and genetic Neurosurg Psychiatry 2019;90(3):268-271.
services. In: Understanding Disparities in Access doi:10.1136/jnnp-2018-319089
to Genomic Medicine: Proceedings of a
22 Wagner KN, Nagaraja H, Allain DC, et al. Patients
Workshop. National Academies Press (US); 2018.
with amyotrophic lateral sclerosis have high
Accessed August 28, 2023. ncbi.nlm.nih.gov/
interest in and limited access to genetic testing.
books/NBK538442/
J Genet Couns 2017;26(3):604-611. doi:10.1007/
10 Fink JK. Hereditary spastic paraplegia: s10897-016-0034-y
clinico-pathologic features and emerging
23 Wagner KN, Nagaraja HN, Allain DC, et al. Patients
molecular mechanisms. Acta Neuropathol (Berl)
with sporadic and familial amyotrophic lateral
2013;126(3):307-328. doi:10.1007/s00401-013-1115-8
sclerosis found value in genetic testing. Mol
11 Lallemant-Dudek P, Durr A. Clinical and genetic Genet Genomic Med 2018;6(2):224-229.
update of hereditary spastic paraparesis. Rev doi:10.1002/mgg3.360
Neurol (Paris) 2021;177(5):550-556. doi:10.1016/
24 Fanos JH, Gelinas DF, Miller RG. “You have shown
j.neurol.2020.07.001
me my end”: attitudes toward presymptomatic
12 Pascual B, de Bot ST, Daniels MR, et al. testing for familial amyotrophic lateral sclerosis.
“Ears of the lynx” MRI sign is associated with Am J Med Genet A 2004;129A(3):248-253.
SPG11 and SPG15 hereditary spastic paraplegia. doi:10.1002/ajmg.a.30178
AJNR Am J Neuroradiol 2019;40(1):199-203.
25 Carmack AJK. Ethical issues in screening.
doi:10.3174/ajnr.A5935
AMA J Ethics 2006;8(1):1-65. doi:10.1001/
virtualmentor.2006.8.1.fred1-0601
130 F E B R U A R Y 2 0 24
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
26 Benatar M, Stanislaw C, Reyes E, et al. 38 Silani V, Corcia P, Harms MB, et al. Genetics of
Presymptomatic ALS genetic counseling and primary lateral sclerosis. Amyotroph Lateral
testing: experience and recommendations. Scler Front Degener 2020;21(sup1):28-34.
Neurology 2016;86(24):2295-2302. doi:10.1212/ doi:10.1080/21678421.2020.1837177
WNL.0000000000002773
39 Turner MR, Barohn RJ, Corcia P, et al. Primary
27 Witzel S, Maier A, Steinbach R, et al. Safety lateral sclerosis: consensus diagnostic criteria.
and effectiveness of long-term intravenous J Neurol Neurosurg Psychiatry 2020;91(4):
administration of edaravone for treatment of 373-377. doi:10.1136/jnnp-2019-322541
Downloaded from http://journals.lww.com/continuum by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCyw
patients with amyotrophic lateral sclerosis.
40 Masingue M, Dufour L, Lenglet T, et al. Natural
JAMA Neurol 2022;79(2):121-130. doi:10.1001/
history of adult patients with GM2
jamaneurol.2021.4893
gangliosidosis. Ann Neurol 2020;87(4):609-617.
CX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC4/OAVpDDa8K2+Ya6H515kE= on 02/16/2024
28 Paganoni S, Hendrix S, Dickson SP, et al. doi:10.1002/ana.25689
Long-term survival of participants in the
41 Breza M, Koutsis G. Kennedy’s disease
CENTAUR trial of sodium phenylbutyrate-taurursodiol
(spinal and bulbar muscular atrophy): a clinically
in amyotrophic lateral sclerosis. Muscle Nerve
oriented review of a rare disease. J Neurol 2019;
2021;63(1):31-39. doi:10.1002/mus.27091
266(3):565-573. doi:10.1007/s00415-018-8968-7
29 Miller TM, Cudkowicz ME, Genge A, et al.
42 Köhler W, Curiel J, Vanderver A. Adulthood
Trial of antisense oligonucleotide tofersen for
leukodystrophies. Nat Rev Neurol 2018;14(2):
SOD1 ALS. N Engl J Med 2022;387(12):1099-1110.
94-105. doi:10.1038/nrneurol.2017.175
doi:10.1056/NEJMoa2204705
43 de Beer M, Engelen M, van Geel BM. Frequent
30 Farrar MA, Kiernan MC. The genetics of spinal
occurrence of cerebral demyelination in
muscular atrophy: progress and challenges.
adrenomyeloneuropathy. Neurology 2014;83(24):
Neurother J Am Soc Exp Neurother 2015;12(2):
2227-2231. doi:10.1212/WNL.0000000000001074
290-302. doi:10.1007/s13311-014-0314-x
44 Zhu J, Eichler F, Biffi A, et al. The changing face of
31 Mercuri E, Sumner CJ, Muntoni F, Darras BT,
adrenoleukodystrophy. Endocr Rev 2020;41(4):
Finkel RS. Spinal muscular atrophy. Nat Rev Dis
577-593. doi:10.1210/endrev/bnaa013
Primer 2022;8(1):52. doi:10.1038/s41572-022-
00380-8 45 Engelen M, Kemp S, Poll-The BT. X-linked
adrenoleukodystrophy: pathogenesis and
32 Kolb SJ, Coffey CS, Yankey JW, et al. Natural
treatment. Curr Neurol Neurosci Rep 2014;14(10):
history of infantile-onset spinal muscular
486. doi:10.1007/s11910-014-0486-0
atrophy. Ann Neurol 2017;82(6):883-891.
doi:10.1002/ana.25101 46 Engelen M, van Ballegoij WJC, Mallack EJ, et al.
International recommendations for the
33 Acsadi G, Crawford TO, Müller-Felber W, et al.
diagnosis and management of patients with
Safety and efficacy of nusinersen in spinal
adrenoleukodystrophy: a consensus-based
muscular atrophy: The EMBRACE study. Muscle
approach. Neurology 2022;99(21):940-951.
Nerve 2021;63(5):668-677. doi:10.1002/mus.27187
doi:10.1212/WNL.0000000000201374
34 Mercuri E, Muntoni F, Baranello G, et al.
47 Köhler W, Engelen M, Eichler F, et al. Safety and
Onasemnogene abeparvovec gene therapy for
efficacy of leriglitazone for preventing disease
symptomatic infantile-onset spinal muscular
progression in men with
atrophy type 1 (STR1VE-EU): an open-label,
adrenomyeloneuropathy (ADVANCE): a
single-arm, multicentre, phase 3 trial. Lancet
randomised, double-blind, multi-centre,
Neurol 2021;20(10):832-841. doi:10.1016/
placebo-controlled phase 2-3 trial. Lancet
S1474-4422(21)00251-9
Neurol 2023;22(2):127-136. doi:10.1016/S1474-4422
35 Masson R, Mazurkiewicz-Bełdzińska M, Rose K, (22)00495-1
et al. Safety and efficacy of risdiplam in patients
48 Walker MA. Hereditary myelopathies.
with type 1 spinal muscular atrophy (FIREFISH
Semin Neurol 2021;41(3):303-308. doi:10.1055/
part 2): secondary analyses from an open-label
s-0041-1725153
trial. Lancet Neurol 2022;21(12):1110-1119.
doi:10.1016/S1474-4422(22)00339-8 49 Souza PVS, Badia BML, Farias IB, et al.
GBE1-related disorders: adult polyglucosan body
36 Dangouloff T, Vrščaj E, Servais L, Osredkar D,
disease and its neuromuscular phenotypes.
SMA NBS World Study Group. Newborn
J Inherit Metab Dis 2021;44(3):534-543.
screening programs for spinal muscular atrophy
doi:10.1002/jimd.12325
worldwide: where we stand and where to go.
Neuromuscul Disord NMD 2021;31(6):574-582. 50 Zebhauser PT, Cordts I, Hengel H, et al.
doi:10.1016/j.nmd.2021.03.007 Characterization of cognitive impairment in adult
polyglucosan body disease. J Neurol 2022;269(6):
37 Naveed A, Calderon H. Onasemnogene
2854-2861. doi:10.1007/s00415-022-10960-z
abeparvovec (AVXS-101) for the treatment of
spinal muscular atrophy. J Pediatr Pharmacol 51 Lecocq C, Charles P, Azulay JP, et al.
Ther JPPT Off J PPAG 2021;26(5):437-444. Delayed-onset Friedreich’s ataxia revisited. Mov
doi:10.5863/1551-6776-26.5.437 Disord Off J Mov Disord Soc 2016;31(1):62-69.
doi:10.1002/mds.26382
CONTINUUMJOURNAL.COM 131
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
GENETIC MYELOPATHIES
52 Alper G, Narayanan V. Friedreich’s ataxia. 54 Sullivan R, Yau WY, O’Connor E, Houlden H.
Pediatr Neurol 2003;28(5):335-341. doi:10.1016/ Spinocerebellar ataxia: an update. J Neurol 2019;
s0887-8994(03)00004-3 266(2):533-544. doi:10.1007/s00415-018-9076-4
53 Lynch DR, Chin MP, Delatycki MB. Safety and 55 de Silva RN, Vallortigara J, Greenfield J, et al.
efficacy of omaveloxolone in Friedreich ataxia Diagnosis and management of progressive ataxia
(MOXIe) Study. Ann Neurol 2021;89(2):212-225. in adults. Pract Neurol 2019;19(3):196-207.
doi:10.1002/ana.25934 doi:10.1136/practneurol-2018-002096
Downloaded from http://journals.lww.com/continuum by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCyw
CX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC4/OAVpDDa8K2+Ya6H515kE= on 02/16/2024
132 F E B R U A R Y 2 0 24
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
You might also like
- Terapias para Doenças NeurodegenerativasDocument41 pagesTerapias para Doenças Neurodegenerativasaurora cavalcantiNo ratings yet
- Continuum MyelopathiesDocument28 pagesContinuum MyelopathiesLaura A M MNo ratings yet
- Bianda Axanditya 22010110130181 Bab2ktiDocument10 pagesBianda Axanditya 22010110130181 Bab2ktimeiutaNo ratings yet
- Zhang 2019Document10 pagesZhang 2019NATALIA MARTINEZ CORDOBANo ratings yet
- ChunDocument3 pagesChungassemNo ratings yet
- Jamaneurology Ayrignac 2022 RV 220003b 166022967554335Document10 pagesJamaneurology Ayrignac 2022 RV 220003b 166022967554335FernandoNo ratings yet
- Demyelinating Diseases: My ApproachDocument9 pagesDemyelinating Diseases: My ApproachRyana Fitriana IINo ratings yet
- Ataxias HereditariasDocument9 pagesAtaxias Hereditariasjosebejarano12No ratings yet
- Genetic Epilepsy SyndromesDocument24 pagesGenetic Epilepsy SyndromesAnali Durán CorderoNo ratings yet
- Infantile, Childhood, and Adolescent Epilepsies.9Document34 pagesInfantile, Childhood, and Adolescent Epilepsies.9Silviana IlieNo ratings yet
- Jurnal Reading Epilepsi (Jenifer Johana Paath 201383019)Document28 pagesJurnal Reading Epilepsi (Jenifer Johana Paath 201383019)jenifer paathNo ratings yet
- Cell Based Therapeutic Strategies For Treatment Of.6Document10 pagesCell Based Therapeutic Strategies For Treatment Of.6Tamara MuñozNo ratings yet
- Fnagi 12 581374Document21 pagesFnagi 12 581374Subash Arunagiri (RA1911009010004)No ratings yet
- Transverse Myelitis: Clinical PracticeDocument9 pagesTransverse Myelitis: Clinical PracticearnabNo ratings yet
- Epilepsy Syndromes inDocument24 pagesEpilepsy Syndromes inEdwin AlvarezNo ratings yet
- Ryan's Retina 7th Ed. Vol.3Document1,064 pagesRyan's Retina 7th Ed. Vol.3karpathakimargaritaNo ratings yet
- Review: Mitochondrial Diseases: Hope For The FutureDocument21 pagesReview: Mitochondrial Diseases: Hope For The Futureluqui guzmanNo ratings yet
- An Insight To Oral Epithelial DysplasiaDocument9 pagesAn Insight To Oral Epithelial DysplasiarinakartikaNo ratings yet
- Cold Spring Harb Perspect Biol-2018-Erkkinen-A033118Document46 pagesCold Spring Harb Perspect Biol-2018-Erkkinen-A033118Brenda GutiérrezNo ratings yet
- Crum Rine 2001Document12 pagesCrum Rine 2001FabsscribNo ratings yet
- Adult LeucodystrophyDocument12 pagesAdult LeucodystrophylauraalvisNo ratings yet
- NIH Public Access: Author ManuscriptDocument15 pagesNIH Public Access: Author ManuscriptMarina Milanović LNo ratings yet
- Seizure: Gan You, Zhiyi Sha, Tao JiangDocument7 pagesSeizure: Gan You, Zhiyi Sha, Tao JiangfachriybalafifNo ratings yet
- Axelrod 2004Document12 pagesAxelrod 2004Nesa An YahdiyaniNo ratings yet
- Adult Onset LeukodistrophiesDocument12 pagesAdult Onset LeukodistrophiesIvan MihailovicNo ratings yet
- Genetic and Epigenetic Factors Which Modulate Differentiation Propensity in Human Pluripotent Stem CellsDocument14 pagesGenetic and Epigenetic Factors Which Modulate Differentiation Propensity in Human Pluripotent Stem Cellsblabarry1109No ratings yet
- Genes 14 00585 PDFDocument13 pagesGenes 14 00585 PDFandy sotoNo ratings yet
- DialoguesClinNeurosci 20 301Document26 pagesDialoguesClinNeurosci 20 301Erick HernandezNo ratings yet
- Autoimmune Vestibulocerebellar SyndromesDocument19 pagesAutoimmune Vestibulocerebellar Syndromesrafael rocha novaesNo ratings yet
- Genetics of Endocrinology: Amit R. Majithia - David Altshuler - Joel N. HirschhornDocument20 pagesGenetics of Endocrinology: Amit R. Majithia - David Altshuler - Joel N. HirschhornDr Mehul Kumar ChourasiaNo ratings yet
- Role of Neuroinflammation in Neurodegeneration DevelopmentDocument32 pagesRole of Neuroinflammation in Neurodegeneration Developmentelibb346No ratings yet
- Biologia Da Mielina e LeucodistrofiasDocument16 pagesBiologia Da Mielina e LeucodistrofiasFernando Cezar dos SantosNo ratings yet
- Out PDFDocument12 pagesOut PDFMaria RenjaanNo ratings yet
- 2 Molecular Genetics in Paediatric DermatologyDocument10 pages2 Molecular Genetics in Paediatric DermatologyAna Li SingNo ratings yet
- Reference Material I 13 PDFDocument11 pagesReference Material I 13 PDFMaru Mengesha Worku 18BBT0285No ratings yet
- Neurodegeneration in Multiple Sclerosis and Neuromyelitis OpticaDocument9 pagesNeurodegeneration in Multiple Sclerosis and Neuromyelitis OpticaEs JerukNo ratings yet
- OrganoidesDocument10 pagesOrganoidesg.colleenNo ratings yet
- Rsob 180138Document19 pagesRsob 180138ilmiah neurologiNo ratings yet
- EtiologyEpilepsy2011ExpertRevNeur (Recovered)Document17 pagesEtiologyEpilepsy2011ExpertRevNeur (Recovered)ArwatiKilwowD'ctzGreenNo ratings yet
- Advances in Molecular Pathology Into Brain Tumor DiajDocument29 pagesAdvances in Molecular Pathology Into Brain Tumor DiajAkshhata NarulkarNo ratings yet
- Tum DemDocument2 pagesTum DemKota AnuroopNo ratings yet
- A Clinician's Approach To Peripheral NeuropathyDocument12 pagesA Clinician's Approach To Peripheral Neuropathytsyrahmani100% (1)
- Breast Cancer: Contribution of Molecular Biology To The Management of The DiseaseDocument9 pagesBreast Cancer: Contribution of Molecular Biology To The Management of The DiseaseKevin ArechigaNo ratings yet
- Modifications Epigenetiques Et Maladies Humaines (Translate PDFDocument26 pagesModifications Epigenetiques Et Maladies Humaines (Translate PDFAkadiri AdjibadéNo ratings yet
- Adams and Victor's - Principles of Neurology-Pages-1073-1137 PDFDocument65 pagesAdams and Victor's - Principles of Neurology-Pages-1073-1137 PDFDin100% (2)
- Basic Research: Epigenetic Approaches To Psychiatric DisordersDocument11 pagesBasic Research: Epigenetic Approaches To Psychiatric DisordersË Äë ChNo ratings yet
- Autism Pathogenesis 2Document18 pagesAutism Pathogenesis 2Prateek Kumar PandaNo ratings yet
- Characteristics of Moyamoya Disease Based On National Registry Data in JapanDocument8 pagesCharacteristics of Moyamoya Disease Based On National Registry Data in JapanBhayu RizallinoorNo ratings yet
- ALS - An Update For 2018Document12 pagesALS - An Update For 2018Aurelia Sartika TongkuNo ratings yet
- Epilepsy 3 PDFDocument14 pagesEpilepsy 3 PDFfikaNo ratings yet
- Protein AggregationDocument29 pagesProtein AggregationAndré PérezNo ratings yet
- Principal Pathogenetic Components and Biological Endophenotypes in Autism Spectrum Disorders (Autism Research, Vol. 3, Issue 5) (2010)Document16 pagesPrincipal Pathogenetic Components and Biological Endophenotypes in Autism Spectrum Disorders (Autism Research, Vol. 3, Issue 5) (2010)Per DahlNo ratings yet
- G Esch Wind 2011Document8 pagesG Esch Wind 2011fatimahNo ratings yet
- Antibody Mediated Autoimmune Encephalitis in ChildhoodDocument11 pagesAntibody Mediated Autoimmune Encephalitis in ChildhoodTessa CruzNo ratings yet
- CRISPR - Based Functional Genomics For Neurological DiseaseDocument16 pagesCRISPR - Based Functional Genomics For Neurological DiseaseKayo PaivaNo ratings yet
- Topic 6 and 7. Monogenic DisordersDocument26 pagesTopic 6 and 7. Monogenic DisordersharshitaNo ratings yet
- Neuropharmacology: Tjitske Kleefstra, Annette Schenck, Jamie M. Kramer, Hans Van BokhovenDocument12 pagesNeuropharmacology: Tjitske Kleefstra, Annette Schenck, Jamie M. Kramer, Hans Van Bokhovenastir1234No ratings yet
- Gim 200691Document10 pagesGim 200691Swathi sampathkumarNo ratings yet
- Clinical Evaluation and Investigation of Neuropathy: Hugh J Willison, John B WinerDocument7 pagesClinical Evaluation and Investigation of Neuropathy: Hugh J Willison, John B WinerCindy Julia AmandaNo ratings yet
- Fneur 12 706169Document14 pagesFneur 12 706169Mayra AldecoaNo ratings yet
- Writing 8 L10Document1 pageWriting 8 L10Mayra AldecoaNo ratings yet
- Writing 7 L10Document1 pageWriting 7 L10Mayra AldecoaNo ratings yet
- Writing 8Document1 pageWriting 8Mayra AldecoaNo ratings yet
- Genetics in Pedo PDFDocument4 pagesGenetics in Pedo PDFhetal majeethiaNo ratings yet
- PhenylketonuriaDocument10 pagesPhenylketonuriaMalathy Ravendran100% (1)
- Bacteriophage MCQsDocument3 pagesBacteriophage MCQsMahi ShafiqueNo ratings yet
- Peran BF Dalam Pandemi Covid-VaksinDocument28 pagesPeran BF Dalam Pandemi Covid-VaksinFara EsterNo ratings yet
- Ruby Seminar AbstrDocument2 pagesRuby Seminar AbstrDrRuby Ranjan SharmaNo ratings yet
- Journal of Neurology Volume 256 Issue 3 2009 (Doi 10.1007/s00415-009-0149-2) T. Lempert H. Neuhauser - Epidemiology of Vertigo, Migraine and Vestibular MigraineDocument6 pagesJournal of Neurology Volume 256 Issue 3 2009 (Doi 10.1007/s00415-009-0149-2) T. Lempert H. Neuhauser - Epidemiology of Vertigo, Migraine and Vestibular MigraineDevi Arnes SimanjuntakNo ratings yet
- ANTICONVULSANTSDocument1 pageANTICONVULSANTSPadmavathi CNo ratings yet
- Human Anatomy and Physiology II: Topic: Anatomy of The Blood Sub Topic: Introduction To Blood and Its CompositionsDocument28 pagesHuman Anatomy and Physiology II: Topic: Anatomy of The Blood Sub Topic: Introduction To Blood and Its Compositionsngong ngong ametNo ratings yet
- Skin Lesions and DiagnosisDocument25 pagesSkin Lesions and DiagnosisBUCM Class 2023No ratings yet
- Drug Addiction Is A State of PeriodicDocument8 pagesDrug Addiction Is A State of PeriodicBastab DeyNo ratings yet
- Molecular Techniques For Detection, Species DifferentiationDocument43 pagesMolecular Techniques For Detection, Species DifferentiationUziel Castillo VelazquezNo ratings yet
- Tissue Gen Bio ReviewerDocument9 pagesTissue Gen Bio ReviewerAlfred CariñoNo ratings yet
- Life Sciences & Chemical Technology: School ofDocument24 pagesLife Sciences & Chemical Technology: School ofjinnaNo ratings yet
- New Orbital Single Use BioreactorDocument1 pageNew Orbital Single Use BioreactorCharles LeeNo ratings yet
- Detailed EoT Coverage 9 ADVDocument50 pagesDetailed EoT Coverage 9 ADVNKANo ratings yet
- Biology Blueprint of Life PDFDocument14 pagesBiology Blueprint of Life PDFlen2000No ratings yet
- Quiz Chapter 62 63Document2 pagesQuiz Chapter 62 63Amelie AvenidoNo ratings yet
- Curriculum Vitae: G.SethuramanDocument4 pagesCurriculum Vitae: G.SethuramanSethuNo ratings yet
- Group Clinical ManualDocument75 pagesGroup Clinical Manualms_atreadNo ratings yet
- Institute of CancerDocument30 pagesInstitute of CancerFilipa RosaNo ratings yet
- The Role of The Nurse in Health Promotion PDFDocument1 pageThe Role of The Nurse in Health Promotion PDFCie Ladd0% (1)
- Corrections and Additions To Taxonomists' Glossary of Mosquito AnatomyDocument17 pagesCorrections and Additions To Taxonomists' Glossary of Mosquito AnatomymokarahNo ratings yet
- Disabilities Research Paper - Morgen GreifDocument10 pagesDisabilities Research Paper - Morgen Greifapi-604606576No ratings yet
- Eye Cancer - Stages and Grades - 2015-09-01Document7 pagesEye Cancer - Stages and Grades - 2015-09-01Ruslan KamilNo ratings yet
- ACOG Practice Bulletin On Thyroid Disease in PregnancyDocument5 pagesACOG Practice Bulletin On Thyroid Disease in Pregnancygenerics54321No ratings yet
- Combined Low-High-Density Modern and Ancient Genome-Wide Data Document Genomic Admixture History of High-Altitude East AsiansDocument18 pagesCombined Low-High-Density Modern and Ancient Genome-Wide Data Document Genomic Admixture History of High-Altitude East AsiansLương Ngọc LinhNo ratings yet
- A Review On Dermatitis HerpetiformisDocument7 pagesA Review On Dermatitis HerpetiformisjessicaNo ratings yet
- HSB Skeletal NotesDocument2 pagesHSB Skeletal NotesArvin SinghNo ratings yet
- Past Exam QuestionsDocument4 pagesPast Exam Questionskeirob100% (1)
- Humor, Laughter, and AgingDocument2 pagesHumor, Laughter, and AgingGordon LoganNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (32)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 4.5 out of 5 stars4.5/5 (82)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Rating: 3 out of 5 stars3/5 (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- To Explain the World: The Discovery of Modern ScienceFrom EverandTo Explain the World: The Discovery of Modern ScienceRating: 3.5 out of 5 stars3.5/5 (51)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 4 out of 5 stars4/5 (4)
- The Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeFrom EverandThe Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeRating: 4.5 out of 5 stars4.5/5 (2)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesFrom EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesRating: 4.5 out of 5 stars4.5/5 (1412)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (39)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (254)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (170)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (46)
- The Marshmallow Test: Mastering Self-ControlFrom EverandThe Marshmallow Test: Mastering Self-ControlRating: 4.5 out of 5 stars4.5/5 (60)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Hearts of Darkness: Serial Killers, The Behavioral Science Unit, and My Life as a Woman in the FBIFrom EverandHearts of Darkness: Serial Killers, The Behavioral Science Unit, and My Life as a Woman in the FBIRating: 4 out of 5 stars4/5 (20)