You might also like
- Cervical Stenosis 2006Document16 pagesCervical Stenosis 2006kppsadiNo ratings yet
- Celiac Disease: DR Ajeet Kumar Lohana Senior Registrar Gastroenterology AtmcDocument59 pagesCeliac Disease: DR Ajeet Kumar Lohana Senior Registrar Gastroenterology AtmcAjeet LohanaNo ratings yet
- RMO Handbook AussieDocument48 pagesRMO Handbook Aussienvrtm43No ratings yet
- Gestational Diabetes MellitusDocument69 pagesGestational Diabetes MellitusStephen BakingNo ratings yet
- Acuan Tarif Jasa Medik Dokter (IDI)Document214 pagesAcuan Tarif Jasa Medik Dokter (IDI)kiyoeugraNo ratings yet
- Reading Comprehension f1Document3 pagesReading Comprehension f1suhailinamohdikhwanNo ratings yet
- Don't Drink Your MilkDocument123 pagesDon't Drink Your MilkConventionalThinker100% (3)
- nsg-432 Careplan 2Document11 pagesnsg-432 Careplan 2api-521003884No ratings yet
- Approach To Neonatal JaundiceDocument73 pagesApproach To Neonatal JaundiceG Venkatesh50% (2)
- Popular Sweeteners and Their Health Effects PDFDocument163 pagesPopular Sweeteners and Their Health Effects PDFMohammad AwaisNo ratings yet
- Giving Instruction To The Patients Nursing / Midwifery English PhrasesDocument31 pagesGiving Instruction To The Patients Nursing / Midwifery English PhrasesOctavia NurulNo ratings yet
- Autoimmune Hepatitis FinalDocument44 pagesAutoimmune Hepatitis FinalritzbinNo ratings yet
- Boala CeliacaDocument111 pagesBoala CeliacaMihaela Boanca100% (1)
- Celiac DiseaseDocument4 pagesCeliac DiseaseEnzo EnzowzowNo ratings yet
- New Guidelines For The Diagnosis of Paediatric Coeliac DiseaseDocument3 pagesNew Guidelines For The Diagnosis of Paediatric Coeliac DiseaseDiana NicaNo ratings yet
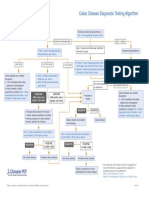
- Celiac Disease Diagnostic Testing AlgorithmDocument1 pageCeliac Disease Diagnostic Testing AlgorithmtarogiosdrakNo ratings yet
- New Guidelines For The Diagnosis of Paediatric Coeliac DiseaseDocument3 pagesNew Guidelines For The Diagnosis of Paediatric Coeliac DiseaseLizette MirandaNo ratings yet
- Criteria 2017Document1 pageCriteria 2017Faidil AkbarNo ratings yet
- Criteria 2017Document1 pageCriteria 2017Nabila ShaharilNo ratings yet
- Anik Widijanti: Clinical Pathology Department Saiful Anwar Hospital / Medical Faculty Brawijaya University MALANGDocument40 pagesAnik Widijanti: Clinical Pathology Department Saiful Anwar Hospital / Medical Faculty Brawijaya University MALANGTutde SedanaNo ratings yet
- Anik Widijanti: Clinical Pathology Department Saiful Anwar Hospital / Medical Faculty Brawijaya University MALANGDocument48 pagesAnik Widijanti: Clinical Pathology Department Saiful Anwar Hospital / Medical Faculty Brawijaya University MALANGTiti 9No ratings yet
- Celiacdiseaseand Nonceliacgluten Sensitivity: Runa D. Watkins,, Shamila ZawahirDocument14 pagesCeliacdiseaseand Nonceliacgluten Sensitivity: Runa D. Watkins,, Shamila ZawahirVicky MacNo ratings yet
- Assessment of A Test For The Screening and Diagnosis of Celiac DiseaseDocument6 pagesAssessment of A Test For The Screening and Diagnosis of Celiac DiseasekameliasitorusNo ratings yet
- Chronic Constipation in A 7-Year-Old Boy: Judy-April Oparaji, MD, RDN, CSP, Theresa Heifert, MDDocument5 pagesChronic Constipation in A 7-Year-Old Boy: Judy-April Oparaji, MD, RDN, CSP, Theresa Heifert, MDbella friscaamaliaNo ratings yet
- Medicine Revision NotesDocument11 pagesMedicine Revision NotesPrerana MahadevaNo ratings yet
- EBM - Diabetes Guidelines (Javidan) 7Document198 pagesEBM - Diabetes Guidelines (Javidan) 7Ash JavidanNo ratings yet
- 5a. Pem Lab DM 2016Document44 pages5a. Pem Lab DM 2016Muhammad DaviqNo ratings yet
- Celiac Disease by DR Mohamed EbraheemDocument12 pagesCeliac Disease by DR Mohamed EbraheemFercho MedNo ratings yet
- Test Purpose Significance: HGB and HCT CBC Blood GroupingDocument1 pageTest Purpose Significance: HGB and HCT CBC Blood GroupingMarwina DorieNo ratings yet
- Obstetrics Case PresentationDocument27 pagesObstetrics Case PresentationMahaprasad sahoo 77No ratings yet
- 16.laboratory Support For DiabetesDocument39 pages16.laboratory Support For DiabetesIgwe SolomonNo ratings yet
- Screening and Preventative CareDocument5 pagesScreening and Preventative Carezoozsuhai2No ratings yet
- Lauren Herr Nsg-432cc-Care-Plan-ExemplarDocument11 pagesLauren Herr Nsg-432cc-Care-Plan-Exemplarapi-520453750100% (1)
- 15 Kuliah Sem 4 Kelainan Endokrin AnakDocument65 pages15 Kuliah Sem 4 Kelainan Endokrin Anakhanifah ratna biranaNo ratings yet
- Diabetes Mellitus: Type 1 DM Type 2 DM Gestational DM Other TypesDocument20 pagesDiabetes Mellitus: Type 1 DM Type 2 DM Gestational DM Other Typesmohamed mowafeyNo ratings yet
- Part 2 Ilaban Mo Yan!!!!!! Lord, Help MeDocument17 pagesPart 2 Ilaban Mo Yan!!!!!! Lord, Help MeJoezer Gumangan VeranoNo ratings yet
- Differentiating Gilbert Syndrome From Crigler Najjar Syndrome Type 2 by Phenobarbitone TestDocument3 pagesDifferentiating Gilbert Syndrome From Crigler Najjar Syndrome Type 2 by Phenobarbitone TestSneeze LouderNo ratings yet
- Dr. Hemi - DM Soyjoy 2018Document23 pagesDr. Hemi - DM Soyjoy 2018Yuvensia Anggita Ayu Nan SariNo ratings yet
- PDFDocument2 pagesPDFMohammed FasilNo ratings yet
- Celiac DZ - PedsDocument12 pagesCeliac DZ - PedsbencleeseNo ratings yet
- Simpo 3 - Dr. Bowo SP - pd-kEMD - How TPatients With Co-Formulation InsulinDocument35 pagesSimpo 3 - Dr. Bowo SP - pd-kEMD - How TPatients With Co-Formulation InsulinAgnes Irene ZagotoNo ratings yet
- Diabetes Comprehensive T2DM Management: Hemi SinoritaDocument47 pagesDiabetes Comprehensive T2DM Management: Hemi SinoritaJipeeZedNo ratings yet
- Neonatal Jaundice: Carolyn Joy Mendoza-Capisnon Geraldine Marie SalvoDocument46 pagesNeonatal Jaundice: Carolyn Joy Mendoza-Capisnon Geraldine Marie SalvoCarolyn CapisnonNo ratings yet
- Type2 diabetes susceptible loci PPARγ2 is not associated with type1 diabetes at age of ~30 in Bangladeshi healthy peopleDocument6 pagesType2 diabetes susceptible loci PPARγ2 is not associated with type1 diabetes at age of ~30 in Bangladeshi healthy peopleOpenaccess Research paperNo ratings yet
- Diagnosis and Management of Paediatric Autoimmune Hepatitis AIH. ESPGHAN Advice Guide. 2019. Ver1.Document4 pagesDiagnosis and Management of Paediatric Autoimmune Hepatitis AIH. ESPGHAN Advice Guide. 2019. Ver1.Carmen OpreaNo ratings yet
- CPT CC5Document103 pagesCPT CC5KAYLLIEN DURANNo ratings yet
- Hellp 2Document57 pagesHellp 2Angela CaguitlaNo ratings yet
- 1.a Diagnostic Test in High Risk Pregnancy LecDocument12 pages1.a Diagnostic Test in High Risk Pregnancy LecFarmisa MannanNo ratings yet
- Diabetes Mellitus: Vy Vu Doctor of Pharmacy Hutech University 07/29/2020Document56 pagesDiabetes Mellitus: Vy Vu Doctor of Pharmacy Hutech University 07/29/2020cyber elf XNo ratings yet
- Management of Type 2 Diabetes and Its ChallengesDocument81 pagesManagement of Type 2 Diabetes and Its ChallengesKay BristolNo ratings yet
- Doença Celíaca Revisão 2017Document14 pagesDoença Celíaca Revisão 2017Bianca CorreaNo ratings yet
- Early Detection and Standardized Diabetes ManagementDocument31 pagesEarly Detection and Standardized Diabetes ManagementaranspeterNo ratings yet
- Jurnal Gastroenterology, Hepatology, and Nutrition PediatricDocument71 pagesJurnal Gastroenterology, Hepatology, and Nutrition PediatricJonathan WelchNo ratings yet
- Boala CeliacaDocument4 pagesBoala CeliacaCristina TudorNo ratings yet
- ABO Hemolytic DiseaseDocument25 pagesABO Hemolytic DiseaseStephanus Alvian RuchiatnaNo ratings yet
- Medicine OSCE - Common Diseases Ver1Document4 pagesMedicine OSCE - Common Diseases Ver1TrisNo ratings yet
- Note 26 Oct 2023Document4 pagesNote 26 Oct 2023Muna HassanNo ratings yet
- File - 20220320 - 212040 - QC1 1134uc 2022-11Document5 pagesFile - 20220320 - 212040 - QC1 1134uc 2022-11Đạt Trần TiếnNo ratings yet
- Assessment of Biochemical Tests in Liver Diseases: Prof. Mohamed Sharaf-EldinDocument46 pagesAssessment of Biochemical Tests in Liver Diseases: Prof. Mohamed Sharaf-EldinKomang YogatamaNo ratings yet
- HDHDHDocument22 pagesHDHDHraduben5403No ratings yet
- Management of Type 2 Diabetes Mellitus (4th Edition) 2009Document8 pagesManagement of Type 2 Diabetes Mellitus (4th Edition) 2009dranony100% (1)
- IJMLR121602Document4 pagesIJMLR121602sandeep raiNo ratings yet
- Diabetus MellitusDocument74 pagesDiabetus MellitusVincent SerNo ratings yet
- Jaundice 11.28.2018Document13 pagesJaundice 11.28.2018Emily EresumaNo ratings yet
- Obstetric HistoryDocument11 pagesObstetric Historyون توNo ratings yet
- Effects of Novel Dual GIP and GLP-1 Receptor Agonist Tirzepatide On Biomarkers of Nonalcoholic Steatohepatitis in Patients With Type 2 DiabetesDocument4 pagesEffects of Novel Dual GIP and GLP-1 Receptor Agonist Tirzepatide On Biomarkers of Nonalcoholic Steatohepatitis in Patients With Type 2 DiabetesAntonio SalemeNo ratings yet
- C5 Protein TherapeuticsDocument23 pagesC5 Protein TherapeuticsMohammad AwaisNo ratings yet
- Protein Therapeutics: Soma Mukherjee SMU, Chemistry 5 April'2011Document25 pagesProtein Therapeutics: Soma Mukherjee SMU, Chemistry 5 April'2011Mohammad AwaisNo ratings yet
- Analyzing Health Equity Using Household Survey DataDocument19 pagesAnalyzing Health Equity Using Household Survey DataMohammad AwaisNo ratings yet
- Happetoprotetive Effect of Ginger and CardamonDocument34 pagesHappetoprotetive Effect of Ginger and CardamonMohammad AwaisNo ratings yet
- MoclodemideDocument1 pageMoclodemideArnzz AgbulosNo ratings yet
- Sample CollectionDocument8 pagesSample CollectionwillowmaecayabyabNo ratings yet
- Elizabeth Perez ResumeDocument2 pagesElizabeth Perez Resumeapi-550438875No ratings yet
- Medical Monitor PDFDocument5 pagesMedical Monitor PDFFábio Vitor MartinsNo ratings yet
- Marijuana Legalization (Copypasta Pastiche)Document4 pagesMarijuana Legalization (Copypasta Pastiche)LeEminenceGriseNo ratings yet
- Case Study Baby HDocument6 pagesCase Study Baby HSharon Williams0% (1)
- Update On Antimicrobial Therapy in Management of Acute Odontogenic Infection in Oral and Maxillofacial SurgeryDocument9 pagesUpdate On Antimicrobial Therapy in Management of Acute Odontogenic Infection in Oral and Maxillofacial SurgeryMARISOL GALLEGO DUQUENo ratings yet
- US6136860Document5 pagesUS6136860Piyush KhetrapalNo ratings yet
- Geriatric Trauma: Florence A MDocument19 pagesGeriatric Trauma: Florence A MflorenceNo ratings yet
- 02 Chain of SurvivalDocument1 page02 Chain of SurvivalHatem FaroukNo ratings yet
- BoilDocument4 pagesBoilPipipopoNo ratings yet
- Men and Chlamydia ScreeningDocument28 pagesMen and Chlamydia ScreeningMen's Health ForumNo ratings yet
- What Is CardiomyopathyDocument8 pagesWhat Is CardiomyopathysakuraleeshaoranNo ratings yet
- Ganoderma Ganotherapeiathefivestagesofaction - GanotherapyDocument4 pagesGanoderma Ganotherapeiathefivestagesofaction - GanotherapysakisgalanNo ratings yet
- Beginning of The Year Clinic Reminders To ParentsDocument2 pagesBeginning of The Year Clinic Reminders To ParentsTuTitNo ratings yet
- 06 - Lec - Stress ReactionsDocument2 pages06 - Lec - Stress Reactionsericka abasNo ratings yet
- Laparoscopy AppendectomyDocument3 pagesLaparoscopy AppendectomyRoxiutaLNo ratings yet
- Bahasa Inggris Iii: 8. Explaining MedicationDocument11 pagesBahasa Inggris Iii: 8. Explaining MedicationErlangga PratamaNo ratings yet
- Illegal and Legal Substance Abuse Amongst Harm Reduction Program Users - A Case Study From CroatiaDocument18 pagesIllegal and Legal Substance Abuse Amongst Harm Reduction Program Users - A Case Study From CroatiamarijaNo ratings yet
- Galvanic Current: Avanianban Chakkarapani K 342 30.01.2015 11.00 Am To 12.00 PMDocument22 pagesGalvanic Current: Avanianban Chakkarapani K 342 30.01.2015 11.00 Am To 12.00 PMLoganathan ChandrasekarNo ratings yet
- Labeling of The Normal Newborn at Risk, High Risk, Sick Client - GARBOSA, RMDocument4 pagesLabeling of The Normal Newborn at Risk, High Risk, Sick Client - GARBOSA, RMRej Garbosa100% (1)
- Acute GlomerulonephritisDocument2 pagesAcute GlomerulonephritisdesaatibagosNo ratings yet
- NCP Poststreptococcal GlomerulonephritisDocument12 pagesNCP Poststreptococcal GlomerulonephritisScarlet ScarletNo ratings yet
- A Case Report On Wound Healing Activity of Cow GheeDocument4 pagesA Case Report On Wound Healing Activity of Cow GheeKishan PatelNo ratings yet