You might also like
- Best Hashtag Guide For Your Instagram PDFDocument10 pagesBest Hashtag Guide For Your Instagram PDFhow toNo ratings yet
- Pastor S HandbookDocument183 pagesPastor S HandbookLarry SheltonNo ratings yet
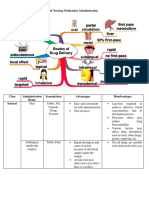
- Different Routes of Nursing Medication AdministrationDocument13 pagesDifferent Routes of Nursing Medication AdministrationRonica MendozaNo ratings yet
- 5 General Principles in TraumaDocument10 pages5 General Principles in TraumaMyrtle Yvonne RagubNo ratings yet
- 1 - Presentation Skill FDocument43 pages1 - Presentation Skill FSyed Abubakar Shah100% (1)
- Manual CT General ElectricDocument68 pagesManual CT General ElectricgegsNo ratings yet
- Summative Exam 4 Sets Inquiry, Investigation and ImmersionDocument7 pagesSummative Exam 4 Sets Inquiry, Investigation and ImmersionAruel Delim100% (4)
- Dounis Interview PDFDocument15 pagesDounis Interview PDFNilson Marcos SoaresNo ratings yet
- Safe Injection and Infusion PracticesDocument32 pagesSafe Injection and Infusion Practicesniraj_sd75% (4)
- Drug Therapy Protocols:: PropofolDocument3 pagesDrug Therapy Protocols:: PropofolEmilyne Joy Mendoza CabayaNo ratings yet
- Knet Open ERP ProposalDocument13 pagesKnet Open ERP ProposalRianov Aja100% (1)
- Intraosseous Vascular Access: E-Learning ResourceDocument20 pagesIntraosseous Vascular Access: E-Learning ResourcenikenauliaputriNo ratings yet
- Nursing CS Electronic-Fetal-Monitoring 03Document1 pageNursing CS Electronic-Fetal-Monitoring 03Jazzmine GuraNo ratings yet
- Ez IoDocument21 pagesEz IoTadesse FentaNo ratings yet
- Intraosseous Devices: Michael W. DayDocument10 pagesIntraosseous Devices: Michael W. DayFarbodNo ratings yet
- Black Yellow Modern Business LetterheadDocument3 pagesBlack Yellow Modern Business LetterheadSalinda TennakoonNo ratings yet
- US-ED02-0050-0119 - Plum 360 woMN SU - GU Training Guide - SW15.11 and Higher - FinalDocument17 pagesUS-ED02-0050-0119 - Plum 360 woMN SU - GU Training Guide - SW15.11 and Higher - FinalgtsantosNo ratings yet
- Administration of Drugs: Studenta:Vornices Olivia Grupa: F1903Document16 pagesAdministration of Drugs: Studenta:Vornices Olivia Grupa: F1903Eugeniu UrsuNo ratings yet
- Routes of Drug Administration The Route of Administration Is Determined Primarily by The Properties of The DrugDocument6 pagesRoutes of Drug Administration The Route of Administration Is Determined Primarily by The Properties of The DrugNouman AsgharNo ratings yet
- Instructions For Use: Nobelactive® ImplantDocument3 pagesInstructions For Use: Nobelactive® ImplantmaxNo ratings yet
- E.S L2-Route of Drug AdministrationDocument28 pagesE.S L2-Route of Drug AdministrationLeen AlhussainNo ratings yet
- Parenteral PreparationDocument23 pagesParenteral PreparationPauline TayabanNo ratings yet
- Inducing Anesthesia - Veterinary Anesthesia Update - VINDocument7 pagesInducing Anesthesia - Veterinary Anesthesia Update - VINmariano marianoNo ratings yet
- PALS Vascular Access Procedures 201309101448412889Document21 pagesPALS Vascular Access Procedures 201309101448412889Mary Janine Joy RimanoNo ratings yet
- Intraosseous Infusion: by Chisupa EricDocument20 pagesIntraosseous Infusion: by Chisupa EricericNo ratings yet
- Paediatric Total Intravenous Anaesthesia BJA 2016Document5 pagesPaediatric Total Intravenous Anaesthesia BJA 2016RicardoNo ratings yet
- Artifacts Quick GuideDocument8 pagesArtifacts Quick GuidermdeloneyNo ratings yet
- Bougie, Stylets, AECsDocument11 pagesBougie, Stylets, AECsThếHuânNo ratings yet
- Prevention of Postoperative Complications of CDocument1 pagePrevention of Postoperative Complications of CChinedu H. DuruNo ratings yet
- Midwifery Pharmacology-2Document2 pagesMidwifery Pharmacology-2georgeloto12No ratings yet
- Rigid Endoscope User ManualDocument2 pagesRigid Endoscope User Manualأحمد العريقيNo ratings yet
- ICU Devices and ProceduresDocument19 pagesICU Devices and Proceduresdyosa 4No ratings yet
- Route of Administration PDFDocument45 pagesRoute of Administration PDFBurhan MubasharNo ratings yet
- A Patient-Classification System For Invisalign Cases: Doug Crosby, DDS, Ms Jessica LeeDocument5 pagesA Patient-Classification System For Invisalign Cases: Doug Crosby, DDS, Ms Jessica LeeShatabdi A ChakravartyNo ratings yet
- Fatih Atug and Raju ThomasDocument3 pagesFatih Atug and Raju ThomasYacine Tarik AizelNo ratings yet
- Веб-страница 2Document1 pageВеб-страница 2Zalina IvanovaNo ratings yet
- Ifu1001 en Us 01Document4 pagesIfu1001 en Us 01B ByrdNo ratings yet
- 155 Anaesthesia For Transurethral Resection of The Prostate (TURP) PDFDocument8 pages155 Anaesthesia For Transurethral Resection of The Prostate (TURP) PDFDwiyanti OktaviaNo ratings yet
- Treat Smart: Procedure-Oriented Solution For Optimal Patient OutcomeDocument7 pagesTreat Smart: Procedure-Oriented Solution For Optimal Patient Outcomevanxuong90No ratings yet
- Medical Abbreviaton Related-To Medication Administration JuvenFajardoBSN1BDocument9 pagesMedical Abbreviaton Related-To Medication Administration JuvenFajardoBSN1Bclint xavier odangoNo ratings yet
- 010303B TCCC-MP Tactical Field Care #2 IG 160603Document45 pages010303B TCCC-MP Tactical Field Care #2 IG 160603herralainNo ratings yet
- Uc201202475en VC Usbrochure2Document8 pagesUc201202475en VC Usbrochure2luiz fernandoNo ratings yet
- Nutrition Lec 10 Diet Surgical Conditions Burns PDFDocument2 pagesNutrition Lec 10 Diet Surgical Conditions Burns PDFbaekho's laughNo ratings yet
- Prone Position Ventilation in Critical Care: IndicationsDocument3 pagesProne Position Ventilation in Critical Care: Indicationsolam batorNo ratings yet
- Uraian Tugas Dan Wewenang Dokter Spesialis AnestesiDocument4 pagesUraian Tugas Dan Wewenang Dokter Spesialis Anestesisri wuryantoNo ratings yet
- Explain 4Document21 pagesExplain 4CHACHACHACHAAAAANo ratings yet
- 4.MEDICAL AND SURGICAL MANAGEMENT (Table 3)Document5 pages4.MEDICAL AND SURGICAL MANAGEMENT (Table 3)SONY MANDAPNo ratings yet
- Alsoprov Slides AsstvaginaldelDocument45 pagesAlsoprov Slides Asstvaginaldelm90No ratings yet
- JAMBALOS JERALDEEN BSN 4 2 DRUG STUDY FormatDocument3 pagesJAMBALOS JERALDEEN BSN 4 2 DRUG STUDY FormatJeraldeen JambalosNo ratings yet
- FAMILY PLANNING - CEU Medicine Lecture Trans (Gynecology)Document7 pagesFAMILY PLANNING - CEU Medicine Lecture Trans (Gynecology)Ian Christopher RochaNo ratings yet
- POST OP BrunnerDocument7 pagesPOST OP Brunnerjamie carpioNo ratings yet
- Routes of AdministrationDocument5 pagesRoutes of AdministrationYousifNo ratings yet
- Cebu Doctors' University College of Nursing Mandaue City, Cebu NCM 109 Theory Postnatal ComplicationsDocument47 pagesCebu Doctors' University College of Nursing Mandaue City, Cebu NCM 109 Theory Postnatal ComplicationsJanica Rose Maloloy-onNo ratings yet
- Emergency Room AssessmentDocument3 pagesEmergency Room AssessmentJULIANNE BEA ACADEMIA BABIERANo ratings yet
- 9 Direct From The Battlefield IgDocument16 pages9 Direct From The Battlefield Igherbert roganNo ratings yet
- Implan Kelompok 2bDocument12 pagesImplan Kelompok 2bVivi KusdiantiNo ratings yet
- 5910JFP Article5Web PDFDocument6 pages5910JFP Article5Web PDFYunita Maharani BurhanNo ratings yet
- EM IOS EZ-IO Recommended Anesthetic Template MC-000554rev3Document6 pagesEM IOS EZ-IO Recommended Anesthetic Template MC-000554rev3EMS HondurasNo ratings yet
- Adjustment Guidelines Removables Orthothondics 1 PDFDocument2 pagesAdjustment Guidelines Removables Orthothondics 1 PDFالحارث اسعد عليNo ratings yet
- Noting Unusualities, Especially The Signs of Respiratory DistressDocument5 pagesNoting Unusualities, Especially The Signs of Respiratory Distressbellie017No ratings yet
- Clinical Scenario 10 SummaryDocument1 pageClinical Scenario 10 SummaryMarios GhobrialNo ratings yet
- Patient Information Leaflet: (Etonogestrel)Document4 pagesPatient Information Leaflet: (Etonogestrel)A VHRSENo ratings yet
- Assess Ment Nursing Diagnos IS Plannin G Nursing Interve Ntion Rationa LE Evaluat IONDocument2 pagesAssess Ment Nursing Diagnos IS Plannin G Nursing Interve Ntion Rationa LE Evaluat IONStephany Dela CruzNo ratings yet
- Butson-2015-Intercostal Catheter InsertionDocument3 pagesButson-2015-Intercostal Catheter InsertionSara JacobsNo ratings yet
- Enteral Nutrition 2020-2021Document65 pagesEnteral Nutrition 2020-2021ﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞNo ratings yet
- MED 6PRMrtNGYrePPaIRVzBiHMnSZ852QCmf5Ft5NrVmoSb23fVx102xbWkZNQsL OriginalDocument24 pagesMED 6PRMrtNGYrePPaIRVzBiHMnSZ852QCmf5Ft5NrVmoSb23fVx102xbWkZNQsL Originalpps g69No ratings yet
- Mte 10Document10 pagesMte 10VipinNo ratings yet
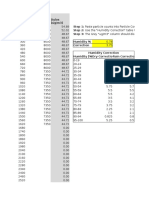
- Dylos Conversion Education - Cehs.health - Umt.eduDocument117 pagesDylos Conversion Education - Cehs.health - Umt.eduMCNo ratings yet
- Module 1 2nd Quarter d11Document5 pagesModule 1 2nd Quarter d11Abbie RañosaNo ratings yet
- Eaton Hydroline TS CylinderDocument8 pagesEaton Hydroline TS CylinderHanzil HakeemNo ratings yet
- Unit - IDocument86 pagesUnit - IZeeshanMirzaNo ratings yet
- Diesel Engine 6R 1000/om 936: IndustrialDocument2 pagesDiesel Engine 6R 1000/om 936: IndustrialAdrian NNo ratings yet
- Tivoli MessagesDocument851 pagesTivoli Messagesjackiexie3813No ratings yet
- EVANGELISM Church PlantingDocument9 pagesEVANGELISM Church PlantingLeon LwambaNo ratings yet
- Worksheet ExerciseDocument2 pagesWorksheet Exerciseshaan shekharNo ratings yet
- PSA Wellness ProgramDocument39 pagesPSA Wellness ProgramFrannie PastorNo ratings yet
- Hf1016414 Hoffman VentiladorDocument4 pagesHf1016414 Hoffman VentiladorMoises AlvarezNo ratings yet
- Module of Instruction: Qualification Unit of Competency Code Module Title Module DescriptorDocument4 pagesModule of Instruction: Qualification Unit of Competency Code Module Title Module DescriptorYeng Lugtu0% (1)
- Power, Promise, Potential, and Posibilities of ParksDocument2 pagesPower, Promise, Potential, and Posibilities of ParksRizza Joy Sariego EsplanaNo ratings yet
- A Charge of A Light BrigadeDocument26 pagesA Charge of A Light Brigadeniluka welagedaraNo ratings yet
- Industrial Visit Report On:-: Jss Mahavidhyapeetha, MysoreDocument14 pagesIndustrial Visit Report On:-: Jss Mahavidhyapeetha, MysoreSiddhantSinghNo ratings yet
- A Guide To Business PHD ApplicationsDocument24 pagesA Guide To Business PHD ApplicationsSampad AcharyaNo ratings yet
- What Is ReactDocument40 pagesWhat Is Reacthabtamu fentewNo ratings yet
- Resultant of Concurrent Force System - Engineering Mechanics ReviewDocument2 pagesResultant of Concurrent Force System - Engineering Mechanics Reviewimrancenakk0% (2)
- Consultant ListDocument9 pagesConsultant ListFitsum DojuNo ratings yet
- St. Pauls 2020 SongbookDocument93 pagesSt. Pauls 2020 SongbooknorthernautumnNo ratings yet
- 3483-Article Text-8498-2-10-20201015Document15 pages3483-Article Text-8498-2-10-20201015Nawzi kagimboNo ratings yet
- Gloria Bay 2020-2021 CVDocument3 pagesGloria Bay 2020-2021 CVapi-280646481No ratings yet
- Datum, Positioning Dan Photo Udara: B. Sulistijo, PHD Email:Budis@Mining - Itb.Ac - Id Private:0812 202 1017Document50 pagesDatum, Positioning Dan Photo Udara: B. Sulistijo, PHD Email:Budis@Mining - Itb.Ac - Id Private:0812 202 1017Hary laksanaNo ratings yet