You might also like
- Perkins Activity and Resource Guide Chapter 2 - Foundations of Learning Language, Cognition, and Social Relationships: Second Edition: Revised and UpdatedFrom EverandPerkins Activity and Resource Guide Chapter 2 - Foundations of Learning Language, Cognition, and Social Relationships: Second Edition: Revised and UpdatedNo ratings yet
- BBT For GEIDocument3 pagesBBT For GEIChris AtkinsonNo ratings yet
- A level Psychology Revision: Cheeky Revision ShortcutsFrom EverandA level Psychology Revision: Cheeky Revision ShortcutsRating: 5 out of 5 stars5/5 (1)
- Assessing Language Skills in Individuals With Autism Spectrum DisordersDocument66 pagesAssessing Language Skills in Individuals With Autism Spectrum Disordersruth shinyNo ratings yet
- 3. Informal Assessment for ChildrenDocument24 pages3. Informal Assessment for Childrenayesha kamalNo ratings yet
- Social/Emotional Development of ChildrenDocument3 pagesSocial/Emotional Development of Childrenlwood06No ratings yet
- Social DevelopmentDocument75 pagesSocial DevelopmentAjay SharmaNo ratings yet
- 5specialed ReferralDocument4 pages5specialed Referralapi-272175868No ratings yet
- Sped ReferralDocument4 pagesSped Referralapi-301878021No ratings yet
- ECCDDocument88 pagesECCDHazel HhetNo ratings yet
- Autism SpectrumDocument12 pagesAutism Spectrumapi-652957143No ratings yet
- Lesson 1Document25 pagesLesson 1Cany Rose MahinayNo ratings yet
- Functional Behaviour Assessment and Positive Behaviour Plan: Student: Tom DiegoDocument9 pagesFunctional Behaviour Assessment and Positive Behaviour Plan: Student: Tom Diegoapi-544801662No ratings yet
- Slides Social InteractionsDocument17 pagesSlides Social InteractionsFernandaNo ratings yet
- Module1 Lesson 1Document20 pagesModule1 Lesson 1Gretchen MacapobreNo ratings yet
- SelectivemutismDocument51 pagesSelectivemutismapi-317112547No ratings yet
- Accommodations MenuDocument28 pagesAccommodations Menuapi-313392868No ratings yet
- ASD PEDS Rating FormDocument1 pageASD PEDS Rating Formmichellezaira123No ratings yet
- Autism Spectrum Disorder (ASD) - CDS PresentationDocument35 pagesAutism Spectrum Disorder (ASD) - CDS PresentationRoslyn MillettNo ratings yet
- Therapuetic_intervention_referral_form (1)Document3 pagesTherapuetic_intervention_referral_form (1)swinky kalraNo ratings yet
- Behavior Management Final ExamDocument21 pagesBehavior Management Final Examapi-603442952No ratings yet
- 3033 Final TestDocument28 pages3033 Final TestSarah SuenNo ratings yet
- Child Development Milestones GuideDocument36 pagesChild Development Milestones GuideDesireeNo ratings yet
- KTKQ 76 UjDocument4 pagesKTKQ 76 Ujapi-564486256No ratings yet
- Responding To The Needs of Students With Autism Spectrum DisordersDocument62 pagesResponding To The Needs of Students With Autism Spectrum DisordersAnanya SenNo ratings yet
- Student Profile InsightsDocument6 pagesStudent Profile InsightsNarender Singh KasanaNo ratings yet
- Ce2-Pedia Bu FormatDocument7 pagesCe2-Pedia Bu FormatCharmaine Jerly NacarioNo ratings yet
- Topic 5 Lifespan DevelopmentDocument30 pagesTopic 5 Lifespan DevelopmentKaibin LowNo ratings yet
- Please Identify & Describe Behaviors You Are Concerned About in The Table BelowDocument7 pagesPlease Identify & Describe Behaviors You Are Concerned About in The Table BelowJamieNo ratings yet
- Early Features AutismDocument4 pagesEarly Features AutismMonica AlexandruNo ratings yet
- Relating Developmental StagesDocument4 pagesRelating Developmental StagesAngelica TraxnomaNo ratings yet
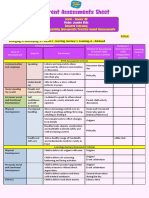
- Senior KG - Parent Assessment SheetDocument1 pageSenior KG - Parent Assessment SheetVikas PawarNo ratings yet
- Preschoolers' Socio-Emotional DevelopmentDocument5 pagesPreschoolers' Socio-Emotional Developmentエルミタ ジョイ ファティマNo ratings yet
- FBAParent InterviewDocument7 pagesFBAParent InterviewJamieNo ratings yet
- Other DisabilitiesDocument42 pagesOther DisabilitiesRica MarquezNo ratings yet
- Comments: Vocab-o-GramsDocument2 pagesComments: Vocab-o-GramsRahul Roll no. 563No ratings yet
- Adhd Parent PacketDocument8 pagesAdhd Parent PacketLisa HernandezNo ratings yet
- EDUC211Document4 pagesEDUC211Maricel Viloria SabaratNo ratings yet
- Selective Mutism: Summary of Issues, Websites, & BibliographyDocument9 pagesSelective Mutism: Summary of Issues, Websites, & BibliographyIbtisam Marohombsar AlontoNo ratings yet
- Dir 101Document59 pagesDir 101rafaelfrizzocallegaroNo ratings yet
- PSY 3410 Autism Spectrum Disorders & Intellectual DisabilityDocument38 pagesPSY 3410 Autism Spectrum Disorders & Intellectual Disabilityncastro1319No ratings yet
- Pervasive Developmental DisordersDocument11 pagesPervasive Developmental Disordersapi-3797941No ratings yet
- ASERT 1332 Teaching Joint Attention Skills in Young Learners Wtih ASDDocument27 pagesASERT 1332 Teaching Joint Attention Skills in Young Learners Wtih ASDneldyNo ratings yet
- PDF For ECS 235Document10 pagesPDF For ECS 235Amie McCormickNo ratings yet
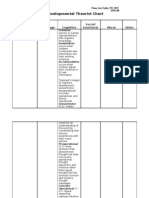
- Theorist-Chart Fall 2010Document11 pagesTheorist-Chart Fall 2010ianptaylorNo ratings yet
- Disabilities Categories and IDEA Docx-1 Matrix Assignment Due 11Document30 pagesDisabilities Categories and IDEA Docx-1 Matrix Assignment Due 11Denise BryantNo ratings yet
- Lecture Class2 Vygotsky Language DevelopmentDocument42 pagesLecture Class2 Vygotsky Language DevelopmentKEZIA SAMSONNo ratings yet
- Report in Prof Ed 10 Chapter 5Document25 pagesReport in Prof Ed 10 Chapter 5Kin TrinidadNo ratings yet
- Basic FBA Process for Reducing Off-Topic Questions in ClassDocument46 pagesBasic FBA Process for Reducing Off-Topic Questions in ClassFai AlamriNo ratings yet
- Case Study of A Child Age 10Document22 pagesCase Study of A Child Age 10api-610745533No ratings yet
- SPM P 3 5 Anos Home PDFDocument2 pagesSPM P 3 5 Anos Home PDFkateb dienelNo ratings yet
- Sett LeeDocument2 pagesSett Leeapi-401705180No ratings yet
- Social DevelopmentDocument3 pagesSocial DevelopmentAshley Co TingNo ratings yet
- DCRDocument2 pagesDCRapi-547693363No ratings yet
- Paediatric Intake Form Modern OT 2018Document6 pagesPaediatric Intake Form Modern OT 2018SefNo ratings yet
- 3310 Study Guide For Exam 2Document2 pages3310 Study Guide For Exam 2ana mooreNo ratings yet
- Play AND Autism: Marisa Lobo Biddappa M.A. M.PhilDocument46 pagesPlay AND Autism: Marisa Lobo Biddappa M.A. M.Philtamara badrovNo ratings yet
- CHARM IE Guide QuestionsDocument6 pagesCHARM IE Guide QuestionsCharmaine Jerly NacarioNo ratings yet
- Management of Autism Spectrum DisordersDocument47 pagesManagement of Autism Spectrum Disorderskeihoina keihoina100% (1)
- Typical and Atypical Development ListDocument2 pagesTypical and Atypical Development ListKenneth EchonNo ratings yet
- MiniBWCVBlendingPunchPack 1Document18 pagesMiniBWCVBlendingPunchPack 1Usamah HussainNo ratings yet
- Narrative 3HR Handout MichiganDocument21 pagesNarrative 3HR Handout MichiganUsamah HussainNo ratings yet
- MacArthur-Bates Communicative Development Inventories (CDIs)Document9 pagesMacArthur-Bates Communicative Development Inventories (CDIs)Ali AsadNo ratings yet
- WPSMusicians 15Document6 pagesWPSMusicians 15Usamah HussainNo ratings yet
- Language ResourcesDocument13 pagesLanguage ResourcesUsamah HussainNo ratings yet
- Stroke Recovery and Rehabilitation 2nd Edition - (Chapter 3 Pathophysiology and Management of Acute Stroke)Document13 pagesStroke Recovery and Rehabilitation 2nd Edition - (Chapter 3 Pathophysiology and Management of Acute Stroke)Usamah HussainNo ratings yet
- MiniBWCVBlendingPunchPack 1Document18 pagesMiniBWCVBlendingPunchPack 1Usamah HussainNo ratings yet
- Laura MartinDocument167 pagesLaura MartinUsamah Hussain50% (2)
- v18 SREBR CH2 NETDocument29 pagesv18 SREBR CH2 NETUsamah HussainNo ratings yet
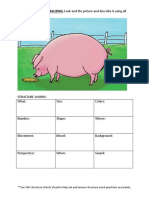
- Your Structure Words!: VISUALIZING AND VERBALIZING: Look and The Picture and Describe It Using AllDocument4 pagesYour Structure Words!: VISUALIZING AND VERBALIZING: Look and The Picture and Describe It Using AllUsamah HussainNo ratings yet
- English ModulesDocument376 pagesEnglish ModulesUsamah HussainNo ratings yet
- Nihms 617023Document12 pagesNihms 617023Usamah HussainNo ratings yet
- Phonological Analysis ProjectDocument16 pagesPhonological Analysis ProjectUsamah HussainNo ratings yet
- OrtonGillinghamToolkitFreebieWordFlashCardsforClosedSyllables 1Document11 pagesOrtonGillinghamToolkitFreebieWordFlashCardsforClosedSyllables 1Usamah HussainNo ratings yet
- ChecklistDocument2 pagesChecklistUsamah HussainNo ratings yet
- Speech Language Concerns Teacher HandoutDocument12 pagesSpeech Language Concerns Teacher HandoutUsamah HussainNo ratings yet
- Adult Placement - Campbelltown Hospital ReflectionsDocument2 pagesAdult Placement - Campbelltown Hospital ReflectionsUsamah HussainNo ratings yet
- Prevalência Do Desvio Fonológico em Crianças Da Cidade de Salvador, BahiaDocument6 pagesPrevalência Do Desvio Fonológico em Crianças Da Cidade de Salvador, BahiaUsamah HussainNo ratings yet
- Rosenshine Principle of InstructionDocument9 pagesRosenshine Principle of InstructionJimmy SiowNo ratings yet
- PB Price Guide 2020-21 v2.1 PDFDocument111 pagesPB Price Guide 2020-21 v2.1 PDFUsamah HussainNo ratings yet
- Teaching Hierarchy of Problem Solving Skills To Children With Learning DisabilitiesDocument5 pagesTeaching Hierarchy of Problem Solving Skills To Children With Learning DisabilitiesUsamah HussainNo ratings yet
- How To Include Your Child's Interests: Join in By..Document8 pagesHow To Include Your Child's Interests: Join in By..Usamah Hussain100% (5)
- How to Connect with Clients and Capture Meaningful MomentsDocument25 pagesHow to Connect with Clients and Capture Meaningful MomentsUsamah HussainNo ratings yet
- Attention and Listening Activities For ChildrenDocument5 pagesAttention and Listening Activities For ChildrenUsamah HussainNo ratings yet
- ICF 2020 HandoutsDocument75 pagesICF 2020 HandoutsUsamah HussainNo ratings yet
- Language Development: DR Sue KermondDocument45 pagesLanguage Development: DR Sue KermondUsamah HussainNo ratings yet
- Attention and Listening Activities For ChildrenDocument5 pagesAttention and Listening Activities For ChildrenUsamah HussainNo ratings yet
- Cueing Hierarchy VisualDocument1 pageCueing Hierarchy VisualUsamah HussainNo ratings yet
- The Role of Branding in PublicDocument16 pagesThe Role of Branding in PublicUsamah HussainNo ratings yet
- GlossophobiaDocument24 pagesGlossophobiarasel0% (1)
- 3.0 Speaking SkillsDocument41 pages3.0 Speaking SkillsKumutha ShiniNo ratings yet
- Informal Speech and Language Assessment GuideDocument13 pagesInformal Speech and Language Assessment GuideGiannina Nicole Cepeda CastilloNo ratings yet
- Speech Sound DisorderDocument2 pagesSpeech Sound DisorderVindo PurbaNo ratings yet
- Signature Assignment 440Document7 pagesSignature Assignment 440api-326311209No ratings yet
- Causes and Coping Strategies of Stuttering Students in Speaking EnglishDocument28 pagesCauses and Coping Strategies of Stuttering Students in Speaking EnglishdaltheaalvadeanneNo ratings yet
- Stammering For Dummies: A Self Help Manual From The Indian Stammering AssociationDocument30 pagesStammering For Dummies: A Self Help Manual From The Indian Stammering AssociationSatyendraSrivastava100% (1)
- Neurogenic Stuttering. PDF /KUNNAMPALLIL GEJODocument33 pagesNeurogenic Stuttering. PDF /KUNNAMPALLIL GEJOKUNNAMPALLIL GEJO JOHN67% (3)
- Assignment TC 111Document3 pagesAssignment TC 111Carla LedinioNo ratings yet
- Cummings L. (Ed.) - The Cambridge Handbook of Communication Disorders-CUP (2013)Document718 pagesCummings L. (Ed.) - The Cambridge Handbook of Communication Disorders-CUP (2013)erlitaNo ratings yet
- Paediatrics MCQsDocument5 pagesPaediatrics MCQsbalarajuuk100% (1)
- Unit 8Document18 pagesUnit 8Santosh AgrayNo ratings yet
- Essay On InventionDocument3 pagesEssay On Inventionafabggede100% (3)
- Rubric For Oral Presentation For STA150Document4 pagesRubric For Oral Presentation For STA150flower boomNo ratings yet
- Communication DisordersDocument5 pagesCommunication DisordersChristienne MoniqueNo ratings yet
- Helping Your Child With Unclear Speech MergedDocument7 pagesHelping Your Child With Unclear Speech MergedAeindrayNo ratings yet
- Cognitive Behavior Therapy For Adults Who Stutter: A Tutorial For Speech-Language PathologistsDocument14 pagesCognitive Behavior Therapy For Adults Who Stutter: A Tutorial For Speech-Language PathologistsPedroNo ratings yet
- COMMUNICATIONDocument57 pagesCOMMUNICATIONMadarang Agustin HulitaNo ratings yet
- Communication Disorders: SymptomsDocument3 pagesCommunication Disorders: SymptomsNoor Ul Hudda MemonNo ratings yet
- Behaviour Problems in Children and HomoeopathyDocument6 pagesBehaviour Problems in Children and HomoeopathyHomoeopathic Pulse100% (1)
- Pharcare Human Dev.Document23 pagesPharcare Human Dev.Gracelyn GatusNo ratings yet
- BholiDocument24 pagesBholiJohny Sins100% (1)
- From The Brain To The MouthDocument187 pagesFrom The Brain To The MouthShaugat AshrafNo ratings yet
- Kings Speech AssignmentDocument8 pagesKings Speech Assignmentapi-294798019100% (1)
- Chapter One-Introduction..NewDocument50 pagesChapter One-Introduction..NewDagiNo ratings yet
- Anglicist-01-01-2012-03.Rhima Puspita Darmadie PDFDocument7 pagesAnglicist-01-01-2012-03.Rhima Puspita Darmadie PDFZehanfarah DibaNo ratings yet
- Fluency Young: Shaping Stutterers WithDocument10 pagesFluency Young: Shaping Stutterers WithvbNo ratings yet
- Genetic Epidemiology of Stuttering Among School Children in The State of Tamil Nadu, IndiaDocument11 pagesGenetic Epidemiology of Stuttering Among School Children in The State of Tamil Nadu, IndiaDai ArhexNo ratings yet
- Introduction To Communication Sciences and Disorders (Weismer) - Rehabilita ShopDocument411 pagesIntroduction To Communication Sciences and Disorders (Weismer) - Rehabilita ShopRomian ValenciaNo ratings yet
- Review Socio-Behavioral Theories and Case StudiesDocument5 pagesReview Socio-Behavioral Theories and Case StudiesMikha DacayananNo ratings yet