You might also like
- Marketing Plan of CostaDocument24 pagesMarketing Plan of CostaScarlet88% (26)
- Dermoscopy Pathology Correlation in MelanomaDocument8 pagesDermoscopy Pathology Correlation in MelanomaDaniela SerbanNo ratings yet
- (1970) Differential Binding of Alkylaing Fluorochrome in Human ChromosomesDocument5 pages(1970) Differential Binding of Alkylaing Fluorochrome in Human Chromosomesmaulia praditaNo ratings yet
- Davis.m.oprendek - Making Progress in Russian - OCRDocument536 pagesDavis.m.oprendek - Making Progress in Russian - OCRJames JonestNo ratings yet
- Lasers Surg Med - 2023 - AhnDocument11 pagesLasers Surg Med - 2023 - AhnBoeroNo ratings yet
- Five Parameters You Must Understand To Master Control of Your Laser:Light-Based DevicesDocument6 pagesFive Parameters You Must Understand To Master Control of Your Laser:Light-Based DevicesgeorgegozarileeNo ratings yet
- 5 Parameters To Master Laser Hair Removal PDFDocument6 pages5 Parameters To Master Laser Hair Removal PDFSuhair F DiebesNo ratings yet
- Macromolecules 1998, 31, 2, 456-461Document6 pagesMacromolecules 1998, 31, 2, 456-461elderwanNo ratings yet
- Ultrasonographic Assessment of Carpal Tunnel.5 PDFDocument9 pagesUltrasonographic Assessment of Carpal Tunnel.5 PDFShinta Marito SihombingNo ratings yet
- The Spectrum of Laser Skin Resurfacing Nonablative, FRACTIONAL and ABLATIVE LASER RESURFACINGDocument610 pagesThe Spectrum of Laser Skin Resurfacing Nonablative, FRACTIONAL and ABLATIVE LASER RESURFACINGBenazier Marcella BesmayaNo ratings yet
- Pigment Cell & Melanoma Research: DOI: 10.1111/pcmr.12535Document7 pagesPigment Cell & Melanoma Research: DOI: 10.1111/pcmr.12535dwyphyNo ratings yet
- 25.gonzalez2010 Skin Research and Tech PDFDocument4 pages25.gonzalez2010 Skin Research and Tech PDFJosé Luis Silva ManriquezNo ratings yet
- Optical Diagnosis Themed Issue: Miniaturisation For Chemistry, Physics, Biology, & BioengineeringDocument6 pagesOptical Diagnosis Themed Issue: Miniaturisation For Chemistry, Physics, Biology, & BioengineeringINFO100% (2)
- Sensitivity of The Human Circadian System To Short-Wavelength (420-nm) LightDocument8 pagesSensitivity of The Human Circadian System To Short-Wavelength (420-nm) LightTibor PappNo ratings yet
- Novel Dosimetry Methods: Introduction: Total Skin Electron Beam Therapy (TSEBT) Has Been Used ForDocument2 pagesNovel Dosimetry Methods: Introduction: Total Skin Electron Beam Therapy (TSEBT) Has Been Used ForVictorM.LópezGuadalupeNo ratings yet
- Braun PDFDocument13 pagesBraun PDFMihail Radu PatrascanuNo ratings yet
- Griffiths ScoreDocument5 pagesGriffiths ScoreAnanya MunjalNo ratings yet
- Efficacy and Safety of 1927 NM Fractional Thulium Fiber Laser For The Treatment of Melasma: A Retrospective Study of 100 PatientsDocument5 pagesEfficacy and Safety of 1927 NM Fractional Thulium Fiber Laser For The Treatment of Melasma: A Retrospective Study of 100 Patientsdl qiuNo ratings yet
- Freeman 1962Document5 pagesFreeman 1962Cata RodriguezNo ratings yet
- Dapsone Loaded IvasomesDocument11 pagesDapsone Loaded IvasomesTheva CharaanNo ratings yet
- The Minimal Erythema Dose (MED) Project: in Search of Consensus On PhototestingDocument2 pagesThe Minimal Erythema Dose (MED) Project: in Search of Consensus On PhototestingSantiago VargasNo ratings yet
- Lasers e HiperpigmentaçãoDocument6 pagesLasers e HiperpigmentaçãoRafael PioltineNo ratings yet
- Ruozi-2009-AFM Phase Imaging of Soft-Hydrated SamplesDocument9 pagesRuozi-2009-AFM Phase Imaging of Soft-Hydrated Samplespablo hervellaNo ratings yet
- Onlinefirst Yurteri Laha2021Document3 pagesOnlinefirst Yurteri Laha2021greyoffice9No ratings yet
- 2019 Melasma - A Critical Analysis of Clinical Trials Investigating Treatment Modalities Published in The Past 10 YearsDocument6 pages2019 Melasma - A Critical Analysis of Clinical Trials Investigating Treatment Modalities Published in The Past 10 Yearsyezafig4001No ratings yet
- Mercury T3 SubclassificationDocument8 pagesMercury T3 SubclassificationMariana Sanches NavasNo ratings yet
- JRPR 41 4 339Document5 pagesJRPR 41 4 339brandonzhen02No ratings yet
- Systematic Review of Laser Therapy in Xanthelasma PalpebrarumDocument9 pagesSystematic Review of Laser Therapy in Xanthelasma PalpebrarumАркадий ЖивицаNo ratings yet
- 1 s2.0 S0892199721001879 MainDocument8 pages1 s2.0 S0892199721001879 MainAbdelkbir WsNo ratings yet
- Methods: Construction of A Workflow For Genome-Wide Variation Analysis of Formalin Fixed Paraffin Embedded Tumor SamplesDocument1 pageMethods: Construction of A Workflow For Genome-Wide Variation Analysis of Formalin Fixed Paraffin Embedded Tumor SamplesZelha NilNo ratings yet
- Near-Infrared Reflectance Analysis Sleeper Among Spectroscopic TechniquesDocument12 pagesNear-Infrared Reflectance Analysis Sleeper Among Spectroscopic TechniquesFabio OliveiraNo ratings yet
- Accurate Classification of Difficult Intubation By.15Document10 pagesAccurate Classification of Difficult Intubation By.15jjmoralesbNo ratings yet
- Classification of Benign and Malignant Tumour Using SVM: J.Saranya.Document6 pagesClassification of Benign and Malignant Tumour Using SVM: J.Saranya.Ajin Nelson NvNo ratings yet
- Melasma 56 Pacientes CoreanosDocument10 pagesMelasma 56 Pacientes CoreanosSuzana PoloncaNo ratings yet
- Simulating Drug Concentrations in PDMSDocument11 pagesSimulating Drug Concentrations in PDMSGüneş Sinan GürelNo ratings yet
- AI Breast ScreeningDocument2 pagesAI Breast ScreeningChan Chee HouNo ratings yet
- Detection and Monitoring of Neurotransmitters - A Spectroscopic AnalysisDocument12 pagesDetection and Monitoring of Neurotransmitters - A Spectroscopic AnalysisJESUS RAUL BELTRAN RAMIREZNo ratings yet
- Oral Tranexamic Acid For The Treatment of Melasma: Karn D, KC S, Amatya A, Razouria EA, Timalsina MDocument4 pagesOral Tranexamic Acid For The Treatment of Melasma: Karn D, KC S, Amatya A, Razouria EA, Timalsina Mangela pavaNo ratings yet
- In Vivo Visualization of Hyaluronic Acid Injection by High Spatial Resolution T Parametric Magnetic Resonance ImagesDocument5 pagesIn Vivo Visualization of Hyaluronic Acid Injection by High Spatial Resolution T Parametric Magnetic Resonance Imagesspinor01238No ratings yet
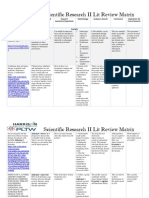
- Lit Matrix 2019Document4 pagesLit Matrix 2019api-387603251No ratings yet
- Piele 3Document5 pagesPiele 3Georgiana BunghiuzNo ratings yet
- An Explainable Machine Learning Model For Early Detection of Parkinson's Disease Using LIME On DaTSCAN ImageryDocument11 pagesAn Explainable Machine Learning Model For Early Detection of Parkinson's Disease Using LIME On DaTSCAN Imageryh4md4nNo ratings yet
- 2008 Shields Faf MelanomaDocument7 pages2008 Shields Faf MelanomapalomaNo ratings yet
- The Role Laser and IPLDocument12 pagesThe Role Laser and IPLisma drNo ratings yet
- Skin Notes For The MCATDocument18 pagesSkin Notes For The MCATsylNo ratings yet
- Tratamiento de Transtornos de Ansiedad Con Terapia de Exposición A Realidad VirtualDocument4 pagesTratamiento de Transtornos de Ansiedad Con Terapia de Exposición A Realidad VirtualOmar AlvarezNo ratings yet
- Evaluation of Plasma Skin Regeneration Technology in Low-Energy Full-Facial RejuvenationDocument7 pagesEvaluation of Plasma Skin Regeneration Technology in Low-Energy Full-Facial RejuvenationCarolina Hoch FariasNo ratings yet
- Jurnal 2Document11 pagesJurnal 2Putri AprilianiNo ratings yet
- Evaluation of Malignant Potential and Surgical Resectability by Using MR Imaging With MR CholangiographyDocument11 pagesEvaluation of Malignant Potential and Surgical Resectability by Using MR Imaging With MR CholangiographyFernando TeixeiraNo ratings yet
- Prediction of Sublayer Depth in Turbid Media Using Spatially Offset Raman SpectrosDocument7 pagesPrediction of Sublayer Depth in Turbid Media Using Spatially Offset Raman SpectrosMax Jordan DooleyNo ratings yet
- Vadim Moskvin 2004 Phys. Med. Biol. 49 003Document18 pagesVadim Moskvin 2004 Phys. Med. Biol. 49 003SUBHANo ratings yet
- Treatment of Xanthelasma Palpebrarum Using PulsedDocument3 pagesTreatment of Xanthelasma Palpebrarum Using PulsedАркадий ЖивицаNo ratings yet
- Modos Raman Sensibles A La Morfología Del Pigmento de La Malaria HemozoínaDocument7 pagesModos Raman Sensibles A La Morfología Del Pigmento de La Malaria HemozoínaIngrid ToleNo ratings yet
- Comparative Efficacy IPL Vs PDLDocument7 pagesComparative Efficacy IPL Vs PDLAnonymous 77IwVByMONo ratings yet
- 蔡政穆-Near infrared spectrum simulation applied to human skin for diagnosisDocument11 pages蔡政穆-Near infrared spectrum simulation applied to human skin for diagnosisData KiswaraNo ratings yet
- Dexmedetomidine Clearance Decreases With Increasing Drug Exposure Implications For Current Dosing Regimens and Target-Controlled Infusion Models Assuming Linear PharmacokineticsDocument14 pagesDexmedetomidine Clearance Decreases With Increasing Drug Exposure Implications For Current Dosing Regimens and Target-Controlled Infusion Models Assuming Linear PharmacokineticsyanaqguzovaNo ratings yet
- CW - Rejuvenation - 2013 - Skin Rejuvenation by Micronnedle Fractional Radiofrequency and A Human Stem Cell Conditioned Medium in Asian SkinDocument9 pagesCW - Rejuvenation - 2013 - Skin Rejuvenation by Micronnedle Fractional Radiofrequency and A Human Stem Cell Conditioned Medium in Asian SkinLillian Floresta HajuNo ratings yet
- Dermatology: Practical & ConceptualDocument2 pagesDermatology: Practical & ConceptualAini MuzayyanaNo ratings yet
- Annals of The New York Academy of Sciences - 2017 - Volz - Pitfalls in Using Fluorescence Tagging of NanomaterialsDocument13 pagesAnnals of The New York Academy of Sciences - 2017 - Volz - Pitfalls in Using Fluorescence Tagging of NanomaterialsbardiyaamrajiNo ratings yet
- 10 1001@jamadermatol 2018 1175Document2 pages10 1001@jamadermatol 2018 1175yalocim666No ratings yet
- RetrieveDocument12 pagesRetrieveChavarry Bustamante RebecaNo ratings yet
- Wood's Light in Dermatology: ReviewDocument12 pagesWood's Light in Dermatology: Reviewsonaljain14143No ratings yet
- Applications of Wood's Lamp Technology To Detect Skin Infections in Resource-Constrained SettingsDocument8 pagesApplications of Wood's Lamp Technology To Detect Skin Infections in Resource-Constrained Settingssonaljain14143No ratings yet
- Journal Pre-Proof: Journal of The American Academy of DermatologyDocument6 pagesJournal Pre-Proof: Journal of The American Academy of Dermatologysonaljain14143No ratings yet
- Basement Membrane ZoneDocument54 pagesBasement Membrane Zonesonaljain14143No ratings yet
- Kotak Securities - Fundamental Analysis Book 1 - IntroductionDocument8 pagesKotak Securities - Fundamental Analysis Book 1 - IntroductionRajesh Bellamkonda0% (1)
- Vibratory Sieve Shaker AS 200 Control: General InformationDocument11 pagesVibratory Sieve Shaker AS 200 Control: General InformationSupriyo PNo ratings yet
- How To Segment Industrial MarketsDocument11 pagesHow To Segment Industrial MarketsPriyabrata Sahoo100% (1)
- Government of India: Form GST REG-06Document3 pagesGovernment of India: Form GST REG-06Allin ExportersNo ratings yet
- NWS 2023 December NewsletterDocument14 pagesNWS 2023 December NewsletternationalwatercolorsocietyNo ratings yet
- Self Declaration Shop PDFDocument2 pagesSelf Declaration Shop PDFSudhir Kotkar0% (2)
- Week 1 6 Black Schedule DLDocument5 pagesWeek 1 6 Black Schedule DLapi-456880356No ratings yet
- Beck PDFDocument1 pageBeck PDFWulan Purwanty100% (1)
- 2020 MSM Lab ManualDocument31 pages2020 MSM Lab Manualdhruv dabhiNo ratings yet
- Parts Number Filter KomatsuDocument1 pageParts Number Filter KomatsuSilvia Gosal100% (1)
- SS CPP 02 Physics Chemistry Mathematics 2020Document32 pagesSS CPP 02 Physics Chemistry Mathematics 2020incognitosigmaextraNo ratings yet
- Raising The Flag of ModernismDocument30 pagesRaising The Flag of ModernismJohn GreenNo ratings yet
- WCC Communication en-USDocument1,098 pagesWCC Communication en-USRiyas ANo ratings yet
- Ola Cabs & Electric Scooter - Bhavish AggarwalDocument7 pagesOla Cabs & Electric Scooter - Bhavish AggarwalAyushi ThakurNo ratings yet
- Rahul PrajapatiDocument9 pagesRahul PrajapatiAdv Tarun PantNo ratings yet
- Science Assessment TaskDocument4 pagesScience Assessment TaskNabiha SyedaNo ratings yet
- Folding Paint Booth: Technology Workshop Craft Home Food Play Outside CostumesDocument8 pagesFolding Paint Booth: Technology Workshop Craft Home Food Play Outside Costumesleotostes2011No ratings yet
- Access Specifiers, Constructors and Methods Exercise: Cognizant Technology SolutionsDocument6 pagesAccess Specifiers, Constructors and Methods Exercise: Cognizant Technology SolutionsKamal WaliaNo ratings yet
- MTTL - Corporate PresentationDocument22 pagesMTTL - Corporate PresentationMaulik RavalNo ratings yet
- Fabrik and Custom Joomla User Registration Forms2Document25 pagesFabrik and Custom Joomla User Registration Forms2Nasiru Abdullahi BabatsofoNo ratings yet
- Chapter 3 Principle of AccountingDocument11 pagesChapter 3 Principle of AccountingAbrha Giday50% (2)
- DFD Caverns PromoDocument10 pagesDFD Caverns PromoPhilippe LouisNo ratings yet
- Johannes 1 To 3 Solution Period 1: © Corporate Finance InstituteDocument4 pagesJohannes 1 To 3 Solution Period 1: © Corporate Finance InstitutePirvuNo ratings yet
- 7 Albano VS CaDocument4 pages7 Albano VS CaJasper LimNo ratings yet
- Differentiated Instruction and Learning Centers PortfolioDocument21 pagesDifferentiated Instruction and Learning Centers Portfolioapi-88644317No ratings yet
- Acou6tics Manual PDFDocument38 pagesAcou6tics Manual PDFRyan FoglemanNo ratings yet
- Case Digest Case 65 Mariano Rodriguez vs. Porfirio BelgicaDocument5 pagesCase Digest Case 65 Mariano Rodriguez vs. Porfirio BelgicaSantiagoJr S XiaoNo ratings yet
- Chapter 3Document25 pagesChapter 3Xuan Mai ĐàmNo ratings yet