You might also like
- PHINMA Education NetworkDocument7 pagesPHINMA Education NetworkMichelle Dona MirallesNo ratings yet
- John Mordechai Gottman, Lynn Fainsilber Katz, Carole Hooven - Meta-Emotion - How Families Communicate Emotionally-Routledge (1997) PDFDocument375 pagesJohn Mordechai Gottman, Lynn Fainsilber Katz, Carole Hooven - Meta-Emotion - How Families Communicate Emotionally-Routledge (1997) PDFRoxana Malan100% (1)
- Informative Speech OutlineDocument4 pagesInformative Speech OutlineMarsha AndersonNo ratings yet
- The Struggle To Be An All American Girl AnalysisDocument24 pagesThe Struggle To Be An All American Girl AnalysisPhilip Suitor100% (1)
- Communication TechniquesDocument10 pagesCommunication TechniquesNur Aleah MedtimbangNo ratings yet
- Silent Screams - Repressed Childhood TraumaDocument6 pagesSilent Screams - Repressed Childhood Traumaananya singhalNo ratings yet
- Psychiatric Nursing 1Document17 pagesPsychiatric Nursing 1Marichu BajadoNo ratings yet
- Therapeutic CommunicationDocument5 pagesTherapeutic CommunicationDishu100% (6)
- Psychiatric Nursing LectureDocument35 pagesPsychiatric Nursing Lectureɹǝʍdןnos95% (42)
- Doctor Patient RealationshipDocument9 pagesDoctor Patient RealationshipSara EamranNo ratings yet
- Form and Style in The Mood For LoveDocument4 pagesForm and Style in The Mood For LoveShannon LisloisNo ratings yet
- Fischer Hoffman ProcessDocument11 pagesFischer Hoffman ProcessNatalie Douglas100% (1)
- TRA Psychiatric NursingDocument10 pagesTRA Psychiatric NursingGil GanibanNo ratings yet
- Psychiatric NursingDocument9 pagesPsychiatric Nursingannbautista.infoNo ratings yet
- CommincationDocument31 pagesCommincationUrdu KahaniNo ratings yet
- Digital Notes On Psychiatric Nursing PDFDocument21 pagesDigital Notes On Psychiatric Nursing PDFEnna EstrellaNo ratings yet
- COMMUNICATION (Nursing)Document6 pagesCOMMUNICATION (Nursing)gracebel reyesNo ratings yet
- Psychiatric NursingDocument5 pagesPsychiatric NursingElla MejiaNo ratings yet
- Chapter 3 Module Therapeutic CommunicationDocument6 pagesChapter 3 Module Therapeutic CommunicationAriane-Gay Cristobal DuranNo ratings yet
- Ch.3 The InterviewDocument9 pagesCh.3 The InterviewJose R. MendozaNo ratings yet
- NEW WORD PsycheDocument66 pagesNEW WORD PsycheRalph FernandezNo ratings yet
- Ppt. The Patient Interview. VSCDocument33 pagesPpt. The Patient Interview. VSCKaye Zelen Lauta100% (1)
- CounselingDocument5 pagesCounselingIrene Demegillo Salonga100% (2)
- Counseling and Interviewing SkillDocument21 pagesCounseling and Interviewing SkillAdamu GudinaNo ratings yet
- 00 PsychDocument11 pages00 PsychAngel LuayonNo ratings yet
- 1.listening: - Listening Is An ActiveDocument4 pages1.listening: - Listening Is An Activesp2056251No ratings yet
- Assignment in Psychiatric Nursing: Submitted To: Ms. Jessica DG. Areja RN, RM Submitted By: Judith R. Dela CruzDocument11 pagesAssignment in Psychiatric Nursing: Submitted To: Ms. Jessica DG. Areja RN, RM Submitted By: Judith R. Dela Cruzjudith dela cruzNo ratings yet
- Therapeutic CommunicationDocument82 pagesTherapeutic CommunicationYvette Vallejo100% (2)
- Bacteria FDocument9 pagesBacteria FKrisha CafongtanNo ratings yet
- The Listening ProcessDocument7 pagesThe Listening ProcessAnderson M MiritiNo ratings yet
- Communication Is A Dynamic Process. It Involves These Three ElementsDocument13 pagesCommunication Is A Dynamic Process. It Involves These Three ElementsRakesh KumarNo ratings yet
- Therapeutic CommunicationDocument20 pagesTherapeutic CommunicationRiccyNo ratings yet
- Presentasi Kuliah Konsep Dasar Komunikasi ProfesionalDocument30 pagesPresentasi Kuliah Konsep Dasar Komunikasi ProfesionalTessa Amanda SavetriNo ratings yet
- Nurse - Client RelationshipDocument88 pagesNurse - Client RelationshipShara SampangNo ratings yet
- Therapeutic Communicatio N and Nurse - Patient RelationshipDocument58 pagesTherapeutic Communicatio N and Nurse - Patient RelationshipSharmila Hemalatha100% (1)
- Midterm ReviewDocument4 pagesMidterm Reviewkittycat16100% (1)
- Therapeutic Communication and Nurse - Patient RelationshipDocument58 pagesTherapeutic Communication and Nurse - Patient RelationshipMelbin W MNo ratings yet
- Communication Skills 2014Document40 pagesCommunication Skills 2014Em KayNo ratings yet
- Midterm - Chapter 2Document22 pagesMidterm - Chapter 2rodamel gundanNo ratings yet
- The Clinical Setting - SFH Iss16Document22 pagesThe Clinical Setting - SFH Iss16elliot100% (1)
- Psychosocial IntegrityDocument48 pagesPsychosocial IntegritypopotaNo ratings yet
- Basic Concepts of Psychiatric NursingDocument52 pagesBasic Concepts of Psychiatric NursingRommel G. SantiagoNo ratings yet
- Communication: NCM 117 A Lec / W2 / AkbaDocument4 pagesCommunication: NCM 117 A Lec / W2 / AkbaAngeli Kristiana AlejandrinoNo ratings yet
- Week9TherapeuticCommunication OUTLINEDocument3 pagesWeek9TherapeuticCommunication OUTLINEEmman MagtibayNo ratings yet
- Therapeutic CommunicationDocument3 pagesTherapeutic CommunicationChora BaguiyacNo ratings yet
- Psych ReviewerDocument12 pagesPsych ReviewerJoan LeonenNo ratings yet
- THERAPEUTIC COMMUNICATION AND NURSE ManagementDocument12 pagesTHERAPEUTIC COMMUNICATION AND NURSE ManagementJyothi Singh Suryavanshi100% (1)
- Lec 2Document2 pagesLec 2Anthony BalacanoNo ratings yet
- Therapeutic Communication Is Defined As TheDocument4 pagesTherapeutic Communication Is Defined As TheAlexa Abidin OldenborgNo ratings yet
- Session 4 - Steps of Health AssessmentDocument63 pagesSession 4 - Steps of Health AssessmentCres Padua Quinzon100% (2)
- Interviewing Patient For Health HistoryDocument11 pagesInterviewing Patient For Health HistoryAeshel TabuzoNo ratings yet
- Communication Skills: Prof. Aparna KanchanDocument38 pagesCommunication Skills: Prof. Aparna KanchanaparnaskiniNo ratings yet
- Definition of IPC (With Answer)Document2 pagesDefinition of IPC (With Answer)EJ LagatNo ratings yet
- 04 - Nondirective Listening SkillsDocument9 pages04 - Nondirective Listening SkillsLauren HerreraNo ratings yet
- NP5 ReviewerDocument6 pagesNP5 ReviewerClarence BravioNo ratings yet
- 31 Therapeutic Communication Techniques With Elderly and Children2Document42 pages31 Therapeutic Communication Techniques With Elderly and Children2Ab Staholic BoiiNo ratings yet
- Pre-Orientation Phase: Anisa A. JamitoDocument23 pagesPre-Orientation Phase: Anisa A. JamitoBella DonnaNo ratings yet
- Therapeutic Communication Techniques PresentationDocument17 pagesTherapeutic Communication Techniques Presentationamal abdulrahmanNo ratings yet
- Carl Rogers-Psychotherapy 7 CounslingDocument18 pagesCarl Rogers-Psychotherapy 7 CounslingDebbie Marie BaisNo ratings yet
- Therapeutic Communication Techniques PresentationDocument17 pagesTherapeutic Communication Techniques Presentationmaeca101100% (2)
- Counselling BasicsDocument26 pagesCounselling BasicsMohamed Ibrahim SirajNo ratings yet
- Active Listening SkillsDocument58 pagesActive Listening SkillsNorjetalexis Maningo Cabrera100% (1)
- Oren Klaff’s Pitch Anything: An Innovative Method for Presenting, Persuading, and Winning the Deal | SummaryFrom EverandOren Klaff’s Pitch Anything: An Innovative Method for Presenting, Persuading, and Winning the Deal | SummaryRating: 3.5 out of 5 stars3.5/5 (11)
- Transpersonal Dynamics: The Relational Field, Depth Work and the UnconsciousFrom EverandTranspersonal Dynamics: The Relational Field, Depth Work and the UnconsciousNo ratings yet
- 25 Lessons in Hypnotism - Being the Most Perfect, Complete, Easily Learned and Comprehensive Course in the World.: Embracing the Science of Magnetic Healing, Telepathy, Mind Reading, Clairvoyant Hypnosis, Mesmerism, Animal Magnetism, thought transference, Personal Magnetism and Kindred Sciences.From Everand25 Lessons in Hypnotism - Being the Most Perfect, Complete, Easily Learned and Comprehensive Course in the World.: Embracing the Science of Magnetic Healing, Telepathy, Mind Reading, Clairvoyant Hypnosis, Mesmerism, Animal Magnetism, thought transference, Personal Magnetism and Kindred Sciences.Rating: 3.5 out of 5 stars3.5/5 (3)
- Secrets of Dark Psychology: Recognizing the manipulatorsFrom EverandSecrets of Dark Psychology: Recognizing the manipulatorsRating: 5 out of 5 stars5/5 (1)
- Session 13 Psychiatric Emergencies - Rape, ChildDocument1 pageSession 13 Psychiatric Emergencies - Rape, ChildMichelle Dona MirallesNo ratings yet
- Fluid and Electrolytes BalanceDocument6 pagesFluid and Electrolytes BalanceMichelle Dona MirallesNo ratings yet
- 9 Hypertension UpdatedDocument23 pages9 Hypertension UpdatedMichelle Dona MirallesNo ratings yet
- PHINMA Education NetworkDocument3 pagesPHINMA Education NetworkMichelle Dona MirallesNo ratings yet
- Rev Enrol ProcDocument2 pagesRev Enrol ProcMichelle Dona MirallesNo ratings yet
- Terazosin Drug Study Group 4Document3 pagesTerazosin Drug Study Group 4Michelle Dona MirallesNo ratings yet
- Drug Study For CefuroximeDocument4 pagesDrug Study For CefuroximeMichelle Dona MirallesNo ratings yet
- Name of Drug Mechanism of Action Contraindication Side Effects Adverse Effects Nursing ResponsibilitiesDocument2 pagesName of Drug Mechanism of Action Contraindication Side Effects Adverse Effects Nursing ResponsibilitiesMichelle Dona MirallesNo ratings yet
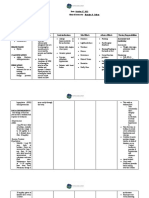
- Assessment Diagnosis Inference Planning Intervention Rationale EvaluationDocument2 pagesAssessment Diagnosis Inference Planning Intervention Rationale EvaluationMichelle Dona MirallesNo ratings yet
- Term 2 UtsDocument5 pagesTerm 2 UtsMichelle Dona MirallesNo ratings yet
- Uts Reviewer FinalDocument21 pagesUts Reviewer FinalMichelle Dona MirallesNo ratings yet
- Gen005 Sas 1 6Document15 pagesGen005 Sas 1 6Michelle Dona MirallesNo ratings yet
- Biochem Term 2Document28 pagesBiochem Term 2Michelle Dona MirallesNo ratings yet
- Stone Age), This Era Is Marked by The Use of Tools by Our Early Human Ancestors (Who Evolved Around 300,000 B.C.)Document7 pagesStone Age), This Era Is Marked by The Use of Tools by Our Early Human Ancestors (Who Evolved Around 300,000 B.C.)Michelle Dona MirallesNo ratings yet
- HowtoBeaMasterofChi PDFDocument70 pagesHowtoBeaMasterofChi PDFahashmi73No ratings yet
- 13 Cancer Nursing Care PlansDocument32 pages13 Cancer Nursing Care Plansmikscribd0143No ratings yet
- Jameson. Modernism As Ideology. 2002Document37 pagesJameson. Modernism As Ideology. 2002Jess and MariaNo ratings yet
- Test-Disc - 28 QuestionsDocument4 pagesTest-Disc - 28 QuestionsScribdTranslationsNo ratings yet
- Counseling Is A Helping Profession That Caters To The Needs of Individuals or Group of IndividualsDocument3 pagesCounseling Is A Helping Profession That Caters To The Needs of Individuals or Group of IndividualsLyra Mae Cananea SubsubanNo ratings yet
- Socioemotional Development in Middle and Late ChildhoodDocument19 pagesSocioemotional Development in Middle and Late ChildhoodNerlyn Gallego ParNo ratings yet
- Hakomi SimplyfiedDocument24 pagesHakomi SimplyfiedJesús Palacios Serna100% (2)
- The World in Revolt A Psychological Study of Our Times - Gustave Le Bon 1921Document268 pagesThe World in Revolt A Psychological Study of Our Times - Gustave Le Bon 1921fillerdealerNo ratings yet
- Bipolar Disorder and Anxiety Disorder PDFDocument13 pagesBipolar Disorder and Anxiety Disorder PDFLisandrea BrownNo ratings yet
- 12 Chakra SystemDocument8 pages12 Chakra Systemsomewhereone100% (1)
- Lunenburg, Fred C. Goal-Setting Theoryof Motivation IJMBA V15 N1 2011Document6 pagesLunenburg, Fred C. Goal-Setting Theoryof Motivation IJMBA V15 N1 2011Chirag Sheth0% (1)
- Mrr3 Ged101 AgustinDocument2 pagesMrr3 Ged101 AgustinSeth Jarl G. AgustinNo ratings yet
- MBA Assignment - Business CommunicationDocument26 pagesMBA Assignment - Business CommunicationSumanth Kumar Sura VenkataNo ratings yet
- Art AppreciationDocument3 pagesArt AppreciationELAIZA MAE DELA CRUZNo ratings yet
- Peeyush - Mittal - Banasthali - PHD Final SynopsisDocument16 pagesPeeyush - Mittal - Banasthali - PHD Final SynopsisPeeyush MittalNo ratings yet
- Journal of Research in Personality: Ryan T. Howell, Masha Ksendzova, Eric Nestingen, Claudio Yerahian, Ravi IyerDocument14 pagesJournal of Research in Personality: Ryan T. Howell, Masha Ksendzova, Eric Nestingen, Claudio Yerahian, Ravi IyerLoredana LaviniaNo ratings yet
- SchizphreniaDocument151 pagesSchizphreniaAyaBasilioNo ratings yet
- The Power of Positive ThinkingDocument2 pagesThe Power of Positive Thinkinghelsil01No ratings yet
- Music, Posthumanism and NietzscheDocument26 pagesMusic, Posthumanism and NietzscheRadoslavNo ratings yet
- Đề Số 1 - Mega Anh 2020 Siêu Tốc Luyện Đề THPT Quốc GiaDocument22 pagesĐề Số 1 - Mega Anh 2020 Siêu Tốc Luyện Đề THPT Quốc GiaThái Quỳnh PhạmNo ratings yet
- Mood DisordersDocument43 pagesMood DisordersmulugetaNo ratings yet
- Bachevalier2006 Orbitofrontal-ADocument21 pagesBachevalier2006 Orbitofrontal-AOni BlenginoNo ratings yet
- Improving Mental Health Through ExerciseDocument6 pagesImproving Mental Health Through ExercisenaddieNo ratings yet
- Case Study Child DevelopmentDocument13 pagesCase Study Child Developmentapi-242483208No ratings yet