You might also like
- Treatment Planning Single Maxillary Anterior Implants for DentistsFrom EverandTreatment Planning Single Maxillary Anterior Implants for DentistsNo ratings yet
- JOrofacSci4296-3244141 090041Document4 pagesJOrofacSci4296-3244141 090041Supriya ShuklaNo ratings yet
- ANTERIORPOINTOFREFERENCEDocument6 pagesANTERIORPOINTOFREFERENCEwaf51No ratings yet
- The Facar Concept: N Gowri, N Gopichander, E SolomonDocument6 pagesThe Facar Concept: N Gowri, N Gopichander, E SolomonankitaNo ratings yet
- Fundamentals For Orientation of Occlusal Plane inDocument4 pagesFundamentals For Orientation of Occlusal Plane innurqumirfanNo ratings yet
- Removable Prosthodontics: The Anterior Point of ReferenceDocument9 pagesRemovable Prosthodontics: The Anterior Point of Referenceayush srivastavaNo ratings yet
- SemiadjustablearticulatorDocument7 pagesSemiadjustablearticulatortanu shaikhNo ratings yet
- Holistic Approach To Full Mouth Rehab PDFDocument5 pagesHolistic Approach To Full Mouth Rehab PDFAna AlvaradoNo ratings yet
- Significance of Facebow TransferDocument5 pagesSignificance of Facebow Transfermedicalrecords211No ratings yet
- Headgear in Orthodontics and Dentofacial OrthopediDocument5 pagesHeadgear in Orthodontics and Dentofacial Orthopedisamira chatilaNo ratings yet
- Facebow Use in Clinical Prosthodontic Practice: KeywordsDocument3 pagesFacebow Use in Clinical Prosthodontic Practice: KeywordsVineela ChowdaryNo ratings yet
- Anterior Point of ReferenceDocument9 pagesAnterior Point of ReferenceAmitNo ratings yet
- Dental ArticulatorsDocument10 pagesDental ArticulatorsOmar Al-FatyanNo ratings yet
- Lateral Profile Pilot StudyDocument6 pagesLateral Profile Pilot StudyArushi AgarwalNo ratings yet
- Prediction in An Ortho Surgical Case: A ReportDocument7 pagesPrediction in An Ortho Surgical Case: A ReportMuhammad AleemNo ratings yet
- Premolar Extraction Affects Mandibular Kinematics: Alejandra Londoño Miguel Assis Cinzia Fornai Markus GrevenDocument9 pagesPremolar Extraction Affects Mandibular Kinematics: Alejandra Londoño Miguel Assis Cinzia Fornai Markus GrevenJORGE CARLOS MELGAR GUTIERREZNo ratings yet
- 199 PDFDocument7 pages199 PDFJordan BzNo ratings yet
- Transfer of Information For Esthetic and Functional Predictability in Severe Wear Cases.Document11 pagesTransfer of Information For Esthetic and Functional Predictability in Severe Wear Cases.jorefe12No ratings yet
- Mehrotra Et Al 2015 Evaluation of The Torque Control of The Maxillary Incisors in Lingual Orthodontics DuringDocument5 pagesMehrotra Et Al 2015 Evaluation of The Torque Control of The Maxillary Incisors in Lingual Orthodontics DuringThang Nguyen TienNo ratings yet
- Cordray QUINTINTLImpscpinorthocorrectionDocument11 pagesCordray QUINTINTLImpscpinorthocorrectionLAURA ESNEDA GIRALDO MEJIANo ratings yet
- CordrayQUINTINTLImpscpinorthocorrection PDFDocument11 pagesCordrayQUINTINTLImpscpinorthocorrection PDFLAURA ESNEDA GIRALDO MEJIANo ratings yet
- JIndianProsthodontSoc184321-4265876 115058Document8 pagesJIndianProsthodontSoc184321-4265876 115058Dr FarhatNo ratings yet
- Occlusal Consideration For Mandibular Implant OverdenturesDocument12 pagesOcclusal Consideration For Mandibular Implant OverdenturesFrancisca Dinamarca Lama100% (1)
- Sonego 2014Document6 pagesSonego 2014Isabella WilkeNo ratings yet
- Shroff Deep Bite MechanicaDocument8 pagesShroff Deep Bite MechanicaDominikaSkórkaNo ratings yet
- Significance of Facebow For Dental RestorationsDocument5 pagesSignificance of Facebow For Dental RestorationsMahmoud Ibrahem maanNo ratings yet
- Mock SurgeryDocument7 pagesMock SurgeryElegant Dental clinicNo ratings yet
- Vreugd 1997 Occlusal ConceptDocument9 pagesVreugd 1997 Occlusal ConceptjotapintorNo ratings yet
- Lec 8Document7 pagesLec 8Dr.Haider Saleem AbdullahNo ratings yet
- A Modified Steiners Analysis That Does Not RequirDocument8 pagesA Modified Steiners Analysis That Does Not RequirKanchit SuwanswadNo ratings yet
- 3differentiated Orthodontic Mechanics For Dental Midline CorrectionDocument6 pages3differentiated Orthodontic Mechanics For Dental Midline Correctionabad salcedoNo ratings yet
- Hanashima Et Al. - 2009 - A Study Regarding Occlusal Plane and Posterior Disocclusion-AnnotatedDocument8 pagesHanashima Et Al. - 2009 - A Study Regarding Occlusal Plane and Posterior Disocclusion-AnnotatedJonathan GIraldo Martinez100% (1)
- Conceptions and Misconceptions About Centric Relation: A Review of LiteratureDocument5 pagesConceptions and Misconceptions About Centric Relation: A Review of LiteratureSahana RangarajanNo ratings yet
- JIndianProsthodontSoc84225-2847937 075439Document3 pagesJIndianProsthodontSoc84225-2847937 075439avi pahwaNo ratings yet
- Coward 2002Document8 pagesCoward 2002Anusha KsNo ratings yet
- Biomechanics of TorqueDocument8 pagesBiomechanics of TorquehemaadriNo ratings yet
- Significance of Facebow For Dental RestorationsDocument5 pagesSignificance of Facebow For Dental RestorationsSahana RangarajanNo ratings yet
- Congenital Radioulnar SynostosisDocument5 pagesCongenital Radioulnar Synostosissandeep nemaNo ratings yet
- Guidelines For Treatment Planning of Mandibular Implant Overdenture PDFDocument6 pagesGuidelines For Treatment Planning of Mandibular Implant Overdenture PDFjoephinNo ratings yet
- Manipulacion Del TransductorDocument6 pagesManipulacion Del TransductororagnysNo ratings yet
- Abutment Options For The Restoration of The Malalinged Implant 2016 PDFDocument5 pagesAbutment Options For The Restoration of The Malalinged Implant 2016 PDFmarwa100% (1)
- 1 Bural2016 PDFDocument11 pages1 Bural2016 PDFPratik HodarNo ratings yet
- Philosophy and Physics of Mandibular Hinge Axis: A Review: International Journal of Scientific Research April 2014Document3 pagesPhilosophy and Physics of Mandibular Hinge Axis: A Review: International Journal of Scientific Research April 2014waf51No ratings yet
- Prosthodontics Horizontal Jaw Relation: Dr. Firas AbdulameerDocument6 pagesProsthodontics Horizontal Jaw Relation: Dr. Firas AbdulameerSahana RangarajanNo ratings yet
- IPIntJMedPaediatrOncol 9 2 77 82Document6 pagesIPIntJMedPaediatrOncol 9 2 77 82Laraduta AgustiniNo ratings yet
- Comparison of The Kois Dento-Facial Analyzer System With An EarboDocument20 pagesComparison of The Kois Dento-Facial Analyzer System With An Earbodrjorgefermin.iceoNo ratings yet
- 1 s2.0 S0901502713000374 MainDocument8 pages1 s2.0 S0901502713000374 MainVeerawit LukkanasomboonNo ratings yet
- Significance of Facebow For Dental Restorations: September 2014Document5 pagesSignificance of Facebow For Dental Restorations: September 2014AnuRaveendranNo ratings yet
- Removable Partial Denture Occlusion: John R. Ivanhoe, DDS, Kevin D. Plummer, DDSDocument17 pagesRemovable Partial Denture Occlusion: John R. Ivanhoe, DDS, Kevin D. Plummer, DDSAna MaríaNo ratings yet
- Bracket Positioning in Orthodontics - Past and PresentDocument8 pagesBracket Positioning in Orthodontics - Past and PresentArianaSzelsky6699No ratings yet
- 2575 PDFDocument4 pages2575 PDFAkshayaa BalajiNo ratings yet
- Schallhorn. A Study of The Arbitrary Center and The Kinematic Center of Rotation For Face-Bow Mountings. (1957)Document8 pagesSchallhorn. A Study of The Arbitrary Center and The Kinematic Center of Rotation For Face-Bow Mountings. (1957)Jose Enrique AvilaNo ratings yet
- A Fixed-Removable Type of Telescopic Prosthesis: A Clinical-ReportDocument4 pagesA Fixed-Removable Type of Telescopic Prosthesis: A Clinical-ReportNegrus StefanNo ratings yet
- 31 Choi DG, Bowley JF, Marx DB. Reliability of Ear Bow Arbitrary Face Bow Transfer Instrument. J Prosthet Dent 1999 Aug 82 (2) 150-6Document7 pages31 Choi DG, Bowley JF, Marx DB. Reliability of Ear Bow Arbitrary Face Bow Transfer Instrument. J Prosthet Dent 1999 Aug 82 (2) 150-6Ful WgNo ratings yet
- Weinberg2001 THERAPEUTIC BIOMECHANICS CONCEPTS AND CLINICAL PROCEDURES TO REDUCE IMPLANT LOADING. PART II - THERAPEUTIC DIFFERENTIAL LOADINGDocument9 pagesWeinberg2001 THERAPEUTIC BIOMECHANICS CONCEPTS AND CLINICAL PROCEDURES TO REDUCE IMPLANT LOADING. PART II - THERAPEUTIC DIFFERENTIAL LOADINGPablo Gutiérrez Da VeneziaNo ratings yet
- 05 Treatment PlannningDocument10 pages05 Treatment PlannningAjit SinhaNo ratings yet
- 7 Shreeprada Dash IJPHRDDecember 2018 IssueDocument7 pages7 Shreeprada Dash IJPHRDDecember 2018 IssueSahana RangarajanNo ratings yet
- Facebow Calliper ReviewDocument5 pagesFacebow Calliper ReviewFaheemuddin Muhammad100% (3)
- Removable Partial Denture OcclusionDocument17 pagesRemovable Partial Denture OcclusionJhuselle Patrice de MesaNo ratings yet
- A Plane of Orientation With An Extracranial AnteriorDocument5 pagesA Plane of Orientation With An Extracranial AnteriorkerolossalahNo ratings yet
- A CLINICAL STUDY OF THlE CONDYLE PATHDocument9 pagesA CLINICAL STUDY OF THlE CONDYLE PATHkerolossalahNo ratings yet
- Silicone Key Device For Maxilla Orientation and Occlusal PlaneDocument5 pagesSilicone Key Device For Maxilla Orientation and Occlusal PlanekerolossalahNo ratings yet
- A Cephalometric Analysis Assessing The Validity of Camper'sDocument11 pagesA Cephalometric Analysis Assessing The Validity of Camper'skerolossalahNo ratings yet
- Development of Prosthodontic Craniofacial StandardsDocument1 pageDevelopment of Prosthodontic Craniofacial StandardskerolossalahNo ratings yet
- A Comparative Study of The Occlusal Plane in DentulousDocument9 pagesA Comparative Study of The Occlusal Plane in DentulouskerolossalahNo ratings yet
- PA SystemDocument1 pagePA SystemSherif SalamaNo ratings yet
- Fundraising Guide For Rescue TeamsDocument5 pagesFundraising Guide For Rescue TeamsDecisions For HeroesNo ratings yet
- Milk Production Trend - Dairy Development - Outlook PDFDocument10 pagesMilk Production Trend - Dairy Development - Outlook PDFrubel_nsuNo ratings yet
- Rocna and Vulcan Anchor DimensionsDocument2 pagesRocna and Vulcan Anchor DimensionsJoseph PintoNo ratings yet
- Ψηφιακός Γραμματισμός ΣταΟπτικοακουστικά Μέσα Σε Διαδικτυακά Περιβάλλοντα ΜάθησηςDocument19 pagesΨηφιακός Γραμματισμός ΣταΟπτικοακουστικά Μέσα Σε Διαδικτυακά Περιβάλλοντα ΜάθησηςSofos LoisosNo ratings yet
- Reference Data Types in JavaDocument3 pagesReference Data Types in Javaeyn batallaNo ratings yet
- Master Teacher Developmental Plan Real2021 2022Document6 pagesMaster Teacher Developmental Plan Real2021 2022Roygvib Clemente MontañoNo ratings yet
- JVC HR-S6970AA Service ManualDocument61 pagesJVC HR-S6970AA Service ManualPriyantha GanegodaNo ratings yet
- B - 21 Raider (6th Gen Fighter)Document2 pagesB - 21 Raider (6th Gen Fighter)AbhijeetNo ratings yet
- Case-Friedland Timbers CompanyDocument2 pagesCase-Friedland Timbers Companytalented guy0% (1)
- Prs-021-0025 - C. Melchers - Coca Cola Naga ProjectDocument2 pagesPrs-021-0025 - C. Melchers - Coca Cola Naga ProjectMiko Christopher OroyanNo ratings yet
- "Cryptochart - Cryptocurrency Price Tracker": East West College of ManagementDocument66 pages"Cryptochart - Cryptocurrency Price Tracker": East West College of ManagementSriharsha S ANo ratings yet
- Oil and Gas - Black Gold!Document32 pagesOil and Gas - Black Gold!tabithapangNo ratings yet
- List of Homoeopathic Medicines, Combinations & Their UsesDocument29 pagesList of Homoeopathic Medicines, Combinations & Their Usesgirish261187% (55)
- Unit 1 Paragraph To EssayDocument55 pagesUnit 1 Paragraph To EssayFrida BrNo ratings yet
- System InformationDocument547 pagesSystem Informationesmerova6735No ratings yet
- SosDocument6 pagesSosVikramNo ratings yet
- 03-Part C3-3 Spec Corrosion ProtectionDocument14 pages03-Part C3-3 Spec Corrosion ProtectionThandabantu MagengeleleNo ratings yet
- What Is OLAP? Cube, Operations & Types in Data WarehouseDocument7 pagesWhat Is OLAP? Cube, Operations & Types in Data WarehouseGabrielAlexandruNo ratings yet
- GateKeeping TheoryDocument7 pagesGateKeeping TheoryFarah100% (1)
- Srinivas Ponraj: Career ObjectiveDocument2 pagesSrinivas Ponraj: Career ObjectiveSrinivasNo ratings yet
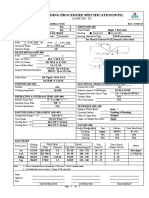
- Welding Procedure Specification (WPS) : (Asme Sec. Ix)Document1 pageWelding Procedure Specification (WPS) : (Asme Sec. Ix)Ahmed Lepda100% (1)
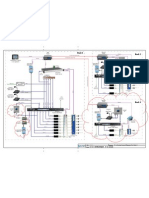
- LM5 RIOL Lite DatasheetDocument12 pagesLM5 RIOL Lite DatasheetStilux VoltNo ratings yet
- Business Partner Application Form: Bintang Arif Kurniawan 08119002384Document1 pageBusiness Partner Application Form: Bintang Arif Kurniawan 08119002384Bintang ArifNo ratings yet
- Cat Oxsilan InternetDocument49 pagesCat Oxsilan InternetAnonymous 1vuTwJVDjYNo ratings yet
- Orca Share Media1676505355563 7031773118863093717Document42 pagesOrca Share Media1676505355563 7031773118863093717Charls Aron ReyesNo ratings yet
- BCA Syllabus 2016-17 CBCS RevisedDocument83 pagesBCA Syllabus 2016-17 CBCS Revisedmalliknl50% (2)
- Sibunag River Development Project: Industry Sector: Business Type: Location TypeDocument4 pagesSibunag River Development Project: Industry Sector: Business Type: Location Typeemma gallosNo ratings yet
- Wound Repair and RegenerationDocument8 pagesWound Repair and RegenerationdrsamnNo ratings yet
- Process-to-Process Delivery: Udp and TCP: (Chapter 23)Document41 pagesProcess-to-Process Delivery: Udp and TCP: (Chapter 23)Giri Tharan RockNo ratings yet
- To Pixar and Beyond: My Unlikely Journey with Steve Jobs to Make Entertainment HistoryFrom EverandTo Pixar and Beyond: My Unlikely Journey with Steve Jobs to Make Entertainment HistoryRating: 4.5 out of 5 stars4.5/5 (260)
- 2022 Adobe® Premiere Pro Guide For Filmmakers and YouTubersFrom Everand2022 Adobe® Premiere Pro Guide For Filmmakers and YouTubersRating: 5 out of 5 stars5/5 (1)
- Learn Power BI: A beginner's guide to developing interactive business intelligence solutions using Microsoft Power BIFrom EverandLearn Power BI: A beginner's guide to developing interactive business intelligence solutions using Microsoft Power BIRating: 5 out of 5 stars5/5 (1)
- How to Create Cpn Numbers the Right way: A Step by Step Guide to Creating cpn Numbers LegallyFrom EverandHow to Create Cpn Numbers the Right way: A Step by Step Guide to Creating cpn Numbers LegallyRating: 4 out of 5 stars4/5 (27)
- Excel Essentials: A Step-by-Step Guide with Pictures for Absolute Beginners to Master the Basics and Start Using Excel with ConfidenceFrom EverandExcel Essentials: A Step-by-Step Guide with Pictures for Absolute Beginners to Master the Basics and Start Using Excel with ConfidenceNo ratings yet
- Blender 3D Basics Beginner's Guide Second EditionFrom EverandBlender 3D Basics Beginner's Guide Second EditionRating: 5 out of 5 stars5/5 (1)
- Skulls & Anatomy: Copyright Free Vintage Illustrations for Artists & DesignersFrom EverandSkulls & Anatomy: Copyright Free Vintage Illustrations for Artists & DesignersNo ratings yet
- The Designer’s Guide to Figma: Master Prototyping, Collaboration, Handoff, and WorkflowFrom EverandThe Designer’s Guide to Figma: Master Prototyping, Collaboration, Handoff, and WorkflowNo ratings yet
- Blender 3D for Jobseekers: Learn professional 3D creation skills using Blender 3D (English Edition)From EverandBlender 3D for Jobseekers: Learn professional 3D creation skills using Blender 3D (English Edition)No ratings yet
- YouTube Growth Mastery: How to Start & Grow A Successful Youtube Channel. Get More Views, Subscribers, Hack The Algorithm, Make Money & Master YouTubeFrom EverandYouTube Growth Mastery: How to Start & Grow A Successful Youtube Channel. Get More Views, Subscribers, Hack The Algorithm, Make Money & Master YouTubeRating: 3 out of 5 stars3/5 (3)
- Tableau Your Data!: Fast and Easy Visual Analysis with Tableau SoftwareFrom EverandTableau Your Data!: Fast and Easy Visual Analysis with Tableau SoftwareRating: 4.5 out of 5 stars4.5/5 (4)
- Data Points: Visualization That Means SomethingFrom EverandData Points: Visualization That Means SomethingRating: 4 out of 5 stars4/5 (14)
- Portfolio and Investment Analysis with SAS: Financial Modeling Techniques for OptimizationFrom EverandPortfolio and Investment Analysis with SAS: Financial Modeling Techniques for OptimizationRating: 3 out of 5 stars3/5 (1)
- Photoshop: A Step by Step Ultimate Beginners’ Guide to Mastering Adobe Photoshop in 1 WeekFrom EverandPhotoshop: A Step by Step Ultimate Beginners’ Guide to Mastering Adobe Photoshop in 1 WeekNo ratings yet
- Animation for Beginners: Getting Started with Animation FilmmakingFrom EverandAnimation for Beginners: Getting Started with Animation FilmmakingRating: 3 out of 5 stars3/5 (1)
- Windows 11 for Beginners: The Complete Step-by-Step User Guide to Learn and Take Full Use of Windows 11 (A Windows 11 Manual with Useful Tips & Tricks)From EverandWindows 11 for Beginners: The Complete Step-by-Step User Guide to Learn and Take Full Use of Windows 11 (A Windows 11 Manual with Useful Tips & Tricks)Rating: 5 out of 5 stars5/5 (1)
- Excel 2024: Mastering Charts, Functions, Formula and Pivot Table in Excel 2024 as a Beginner with Step by Step GuideMastering Charts, Functions, Formula and Pivot Table in Excel 2024 as a Beginner with Step by Step GuideFrom EverandExcel 2024: Mastering Charts, Functions, Formula and Pivot Table in Excel 2024 as a Beginner with Step by Step GuideMastering Charts, Functions, Formula and Pivot Table in Excel 2024 as a Beginner with Step by Step GuideNo ratings yet
- Mastering YouTube Automation: The Ultimate Guide to Creating a Successful Faceless ChannelFrom EverandMastering YouTube Automation: The Ultimate Guide to Creating a Successful Faceless ChannelNo ratings yet