You might also like
- HSB Sba FFFFFDocument17 pagesHSB Sba FFFFFshelly0% (1)
- Rauni Leena Luukanen Kilde There Is No DeathDocument2 pagesRauni Leena Luukanen Kilde There Is No Deathsisterrosetta75% (4)
- Abandonando A IgrejaDocument59 pagesAbandonando A IgrejaOsvaldo VungeNo ratings yet
- Misquitta 20202Document86 pagesMisquitta 20202kern tranhNo ratings yet
- Prediabetes - (Slide For Speaker)Document51 pagesPrediabetes - (Slide For Speaker)Maya Sari HalimNo ratings yet
- Discipline Report: Evans High School Columbia CountyDocument4 pagesDiscipline Report: Evans High School Columbia CountyJeremy TurnageNo ratings yet
- Market Pulse Q4 Report - Nielsen Viet Nam: Prepared by Nielsen Vietnam February 2017Document8 pagesMarket Pulse Q4 Report - Nielsen Viet Nam: Prepared by Nielsen Vietnam February 2017K57.CTTT BUI NGUYEN HUONG LYNo ratings yet
- Annex 1A SchoolCommunityDataTemplate SRESDocument19 pagesAnnex 1A SchoolCommunityDataTemplate SRESMA. CRISTINA SERVANDONo ratings yet
- Prof. Lesmana - The 4th Liv GI Fair PGC On Hepatitis C Evolution of DAA (Direct Acting Antiviral AgentDocument26 pagesProf. Lesmana - The 4th Liv GI Fair PGC On Hepatitis C Evolution of DAA (Direct Acting Antiviral AgentWenny NgawingNo ratings yet
- Children's Health Coverage and Care: Key IssuesDocument14 pagesChildren's Health Coverage and Care: Key IssuesNational Press FoundationNo ratings yet
- The Impact of Overconsumption of SugarDocument11 pagesThe Impact of Overconsumption of SugarHermilinda Orenze100% (5)
- 352 - Infographic Market Pulse Q1 2018 - 1525948613Document2 pages352 - Infographic Market Pulse Q1 2018 - 1525948613K57.CTTT BUI NGUYEN HUONG LYNo ratings yet
- Market Pulse Q1 - 18Document2 pagesMarket Pulse Q1 - 18Duy Nguyen Ho ThienNo ratings yet
- Vietnam Digital Landscape 2023Document119 pagesVietnam Digital Landscape 2023gis3d.bhsNo ratings yet
- Uganda:: Population Factors & National DevelopmentDocument42 pagesUganda:: Population Factors & National DevelopmentkasuleNo ratings yet
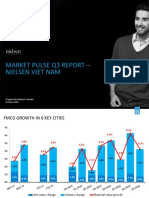
- Nielsen Market Pulse Q3 2017Document2 pagesNielsen Market Pulse Q3 2017K57.CTTT BUI NGUYEN HUONG LYNo ratings yet
- The Relationship Between Frequency of High-Sugar, Salt and Fat Food Consumption and The BMI in AdolescentsDocument8 pagesThe Relationship Between Frequency of High-Sugar, Salt and Fat Food Consumption and The BMI in Adolescentshisbullah smithNo ratings yet
- Launching The Credit Card in Asia PacificDocument10 pagesLaunching The Credit Card in Asia PacificNaveenParameswarNo ratings yet
- Safe Motherhood Project Updated PresentationDocument43 pagesSafe Motherhood Project Updated Presentationmohamedamiinhassan6No ratings yet
- ISDA 2012 Diabetic Foot GuidelinesDocument55 pagesISDA 2012 Diabetic Foot Guidelinessunil abrahamNo ratings yet
- Tobacco Control: Celebrating Extraordinary Progress While Preparing For Challenges AheadDocument35 pagesTobacco Control: Celebrating Extraordinary Progress While Preparing For Challenges AheadNational Press FoundationNo ratings yet
- Prediabetes S1 Burden.020118Document5 pagesPrediabetes S1 Burden.020118RameshKrishnanNo ratings yet
- 2016 Alcohol Risk Assessment - NHS Health CheckDocument55 pages2016 Alcohol Risk Assessment - NHS Health CheckGuadalupe TorradoNo ratings yet
- Nutritional Status of Filipino Adolescents, 10-19 Years OldDocument35 pagesNutritional Status of Filipino Adolescents, 10-19 Years OldCar OrdzNo ratings yet
- Germany: No Data Available No Data AvailableDocument1 pageGermany: No Data Available No Data AvailableJpr Kca MjtrNo ratings yet
- 01.1 Plan Lineal Canal, Cesar MarzoDocument3 pages01.1 Plan Lineal Canal, Cesar MarzoAlejandro MarquezNo ratings yet
- 1 - Overview of Diabetes CPG 2015Document26 pages1 - Overview of Diabetes CPG 2015Andi Pangeran AryaNo ratings yet
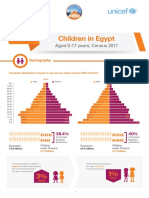
- Children (English)Document6 pagesChildren (English)Nancy NashaatNo ratings yet
- Central Region Political Opinion Poll - October 2021Document23 pagesCentral Region Political Opinion Poll - October 2021The Star Kenya100% (1)
- Nutritional Status of Filipino Pre-School Children (2-5 Years Old)Document20 pagesNutritional Status of Filipino Pre-School Children (2-5 Years Old)Car OrdzNo ratings yet
- Nielsen Market Pulse Q3 2016Document8 pagesNielsen Market Pulse Q3 2016K57.CTTT BUI NGUYEN HUONG LYNo ratings yet
- Colorectal Cancer Screening in Alberta ...Document23 pagesColorectal Cancer Screening in Alberta ...cydolusNo ratings yet
- Columna1 Columna2 Columna3 Tasa de Desempleo Tasa de InflacionDocument7 pagesColumna1 Columna2 Columna3 Tasa de Desempleo Tasa de Inflacionjorge eliecer ibarguen palaciosNo ratings yet
- RPS Tax HistoryDocument2 pagesRPS Tax HistoryinforumdocsNo ratings yet
- DJA - AA - PEN 06.july.2021 ArtiDocument16 pagesDJA - AA - PEN 06.july.2021 ArtiAngga AnugrawanNo ratings yet
- 19-26 JanDocument93 pages19-26 Jansaadsebti01No ratings yet
- HTN Slide Deck NewDocument27 pagesHTN Slide Deck NewChristy BerryNo ratings yet
- Discipline Report: Harlem High School Columbia CountyDocument4 pagesDiscipline Report: Harlem High School Columbia CountyJeremy TurnageNo ratings yet
- DR Dolgoff Handout 2010Document8 pagesDR Dolgoff Handout 2010min babyNo ratings yet
- WFM Bfing Experience 2022Document14 pagesWFM Bfing Experience 2022api-625120170No ratings yet
- Sri Lanka: No Data Available No Data AvailableDocument1 pageSri Lanka: No Data Available No Data AvailablePragith WijeratnamNo ratings yet
- Project S2 Result ThuyAnhDocument3 pagesProject S2 Result ThuyAnhHồng NhungNo ratings yet
- Diabetic Retinopathy Screening Module PDFDocument96 pagesDiabetic Retinopathy Screening Module PDFpet_al2001No ratings yet
- Aspen Hill Planning Area: Montgomery County, MD. 2005 Census Update SurveyDocument42 pagesAspen Hill Planning Area: Montgomery County, MD. 2005 Census Update SurveyM-NCPPCNo ratings yet
- Diabetic Retinopathy Screening ModuleDocument96 pagesDiabetic Retinopathy Screening ModuleSehaRizaNo ratings yet
- Aspen Hill Planning Area: Montgomery County, MD. 2005 Census Update SurveyDocument2 pagesAspen Hill Planning Area: Montgomery County, MD. 2005 Census Update SurveyM-NCPPCNo ratings yet
- Aspen Hill Planning Area: Montgomery County, MD. 2005 Census Update SurveyDocument44 pagesAspen Hill Planning Area: Montgomery County, MD. 2005 Census Update SurveyM-NCPPCNo ratings yet
- Use of e Cigarettes Among Young People in Great Britain 2022Document14 pagesUse of e Cigarettes Among Young People in Great Britain 2022Susan CapellanNo ratings yet
- Axis Bank InvestmentDocument32 pagesAxis Bank Investment22satendraNo ratings yet
- Word MGG 2Document3 pagesWord MGG 2Nova LucyanaNo ratings yet
- FactsDocument2 pagesFactsrogibogiNo ratings yet
- Nutritional Status of Filipino Infants and Young Children 0-23 MonthsDocument24 pagesNutritional Status of Filipino Infants and Young Children 0-23 MonthsCar OrdzNo ratings yet
- Nielsen Market Pulse Q2 2018Document6 pagesNielsen Market Pulse Q2 2018K57.CTTT BUI NGUYEN HUONG LYNo ratings yet
- Kensington / University Boulevard Sector Plan: Montgomery County, MD. 2005 Census Update SurveyDocument2 pagesKensington / University Boulevard Sector Plan: Montgomery County, MD. 2005 Census Update SurveyM-NCPPCNo ratings yet
- Consumer Attitudes Toward Organically Grown LettuceDocument6 pagesConsumer Attitudes Toward Organically Grown LettuceGopalan KathiravanNo ratings yet
- Luchie See - NCHFD-MicronutrientDocument53 pagesLuchie See - NCHFD-MicronutrientSophie RoseNo ratings yet
- Hasil Pengolahan Data YuniDocument8 pagesHasil Pengolahan Data YunizulfadliNo ratings yet
- Breakfast Intake Among Children and Adolescents: United States, 2015-2018Document8 pagesBreakfast Intake Among Children and Adolescents: United States, 2015-2018Ánh NguyễnNo ratings yet
- Discipline Report: Evans Middle School Columbia CountyDocument4 pagesDiscipline Report: Evans Middle School Columbia CountyJeremy TurnageNo ratings yet
- Childhood Obesity: Causes and Consequences, Prevention and Management.From EverandChildhood Obesity: Causes and Consequences, Prevention and Management.No ratings yet
- Methods For Determining Time of Death - Maeda B - For Sci Med Pathol 2016Document35 pagesMethods For Determining Time of Death - Maeda B - For Sci Med Pathol 2016Txemari100% (1)
- Oyster Meat F.S.Document25 pagesOyster Meat F.S.mxviolet67% (3)
- ELE-3COP-361: Title - Application of Raybraid and Instalite Braid To Hand Laid CablesDocument3 pagesELE-3COP-361: Title - Application of Raybraid and Instalite Braid To Hand Laid Cablesmurat degirmenciNo ratings yet
- Stok Per 31 Mei 23Document19 pagesStok Per 31 Mei 23ernaliaNo ratings yet
- Oposa VS FactoranDocument22 pagesOposa VS FactoranMinnie chanNo ratings yet
- Jamapediatrics Sung 2020 Oi 200026Document9 pagesJamapediatrics Sung 2020 Oi 200026Chong ArthinantNo ratings yet
- SimethiconeDocument1 pageSimethiconeDivine Dela PenaNo ratings yet
- Mouth WashDocument28 pagesMouth WashDr ajayNo ratings yet
- Transference and Countertransference in Communication Between Doctor and PatientDocument14 pagesTransference and Countertransference in Communication Between Doctor and PatientAlina Topor Psi-Medical100% (1)
- Malegnantdx 3Document16 pagesMalegnantdx 3Ahmad KaramNo ratings yet
- Noninvasive Strategies For Management of Respiratory Problems in NeonatesDocument12 pagesNoninvasive Strategies For Management of Respiratory Problems in NeonatesGaby RiveraNo ratings yet
- CHUYÊN ĐỀ CỤM TỪ - P6 - VIMDocument3 pagesCHUYÊN ĐỀ CỤM TỪ - P6 - VIMLý Gia HânNo ratings yet
- HOK Canada Education BrochureDocument68 pagesHOK Canada Education BrochureHOKNo ratings yet
- Influence of A Physical Exercise Programme On VO2max in Adults With Cardiovascular Risk Factors PDFDocument7 pagesInfluence of A Physical Exercise Programme On VO2max in Adults With Cardiovascular Risk Factors PDFMAURO ALBERTO OTÁLORA ANTOLINEZNo ratings yet
- Material Safety Data SheetDocument13 pagesMaterial Safety Data SheetDhyta_Anne_Hudge_497No ratings yet
- Dwnload Full Administrative Medical Assisting 8th Edition French Solutions Manual PDFDocument35 pagesDwnload Full Administrative Medical Assisting 8th Edition French Solutions Manual PDFalanlocvs3c100% (15)
- SynopsisDocument9 pagesSynopsisjoy parimalaNo ratings yet
- Ehs 019 Houston Contactor Safety ProcedureDocument17 pagesEhs 019 Houston Contactor Safety ProcedureSayed AbbasNo ratings yet
- July'23 Trauma-Informed TrainingDocument11 pagesJuly'23 Trauma-Informed TrainingezazpsychologistNo ratings yet
- Principles of Fasting in Ayurveda: Sandip T. Gaikwad, Pradnya Gaikwad and Vikas SaxenaDocument6 pagesPrinciples of Fasting in Ayurveda: Sandip T. Gaikwad, Pradnya Gaikwad and Vikas SaxenaAdi W. BuwanaNo ratings yet
- Aquaculture PaperDocument11 pagesAquaculture Paperapi-339322911No ratings yet
- 9.9 Differential Pressure TransmittersDocument99 pages9.9 Differential Pressure TransmittersorazioconiglioNo ratings yet
- 4HB0 02 Que 20120307Document16 pages4HB0 02 Que 20120307muhajireenNo ratings yet
- TNPSC142013 - 341107537 ApplicationDocument3 pagesTNPSC142013 - 341107537 ApplicationGautham PandianNo ratings yet
- Environmental Monitoring ProgramDocument8 pagesEnvironmental Monitoring Programmonik manuelNo ratings yet
- Sukhdeep Sachdev - Mediworld July-Aug 2019Document7 pagesSukhdeep Sachdev - Mediworld July-Aug 2019Leader Healthcare Power CafeNo ratings yet
- Bone and Connective TissueDocument20 pagesBone and Connective TissueKarka PalmaNo ratings yet
- Iitb Sus ReportDocument65 pagesIitb Sus ReportSaharshNo ratings yet
- Project ProposalDocument37 pagesProject ProposalGlyrine PunzalanNo ratings yet