You might also like
- Towards Healthcare EmancipationDocument437 pagesTowards Healthcare EmancipationAnton SorinNo ratings yet
- D Di2Document5 pagesD Di2ARIF AHAMMED P100% (1)
- ChorioretinitisDocument13 pagesChorioretinitisrada tri rosi kurniaNo ratings yet
- Family Guide To Homeopathy EN UK PDFDocument215 pagesFamily Guide To Homeopathy EN UK PDFsumarum60% (5)
- Vaccination Requirement International Students 022019Document2 pagesVaccination Requirement International Students 022019KryzNo ratings yet
- USC Immunization Checklist FormDocument2 pagesUSC Immunization Checklist FormbuiiiilderNo ratings yet
- Student Immunization Form 2017-2018Document2 pagesStudent Immunization Form 2017-2018Yashu SharmaNo ratings yet
- DTP, Dtap, DT, TD or TdapDocument2 pagesDTP, Dtap, DT, TD or TdapAziz DuishevvNo ratings yet
- Immunization Form For Students 2019-20 FINAL 2Document2 pagesImmunization Form For Students 2019-20 FINAL 2Rex ChanNo ratings yet
- CSU Health Form Final Update 8 2015Document2 pagesCSU Health Form Final Update 8 2015Jenna Louise TothNo ratings yet
- Immunization Report PDFDocument2 pagesImmunization Report PDFJag UnathNo ratings yet
- 耶鲁大学 免疫表格immunization Form 2021-7-30Document2 pages耶鲁大学 免疫表格immunization Form 2021-7-30Chris HahaNo ratings yet
- San Diego Unified COVID-19 Vaccination RoadmapDocument17 pagesSan Diego Unified COVID-19 Vaccination RoadmapDillon DavisNo ratings yet
- Univ of Florida ImmunisationDocument2 pagesUniv of Florida ImmunisationPavan Kumar MangipudiNo ratings yet
- PDPG25 CardDocument2 pagesPDPG25 CardThe DominionNo ratings yet
- Immunization Record PART I: To Be Completed by The Student. Please Print or TypeDocument3 pagesImmunization Record PART I: To Be Completed by The Student. Please Print or Typeruhayl khanNo ratings yet
- 2019 - 2020 - Boston Immunization - Hult Immunization FormDocument4 pages2019 - 2020 - Boston Immunization - Hult Immunization FormOscar RomainvilleNo ratings yet
- D Dimer in COVID 19 A Guide With Pitfalls.3Document1 pageD Dimer in COVID 19 A Guide With Pitfalls.3Daniela Mihaela ConstantinNo ratings yet
- Immunization InstructionsDocument2 pagesImmunization InstructionsAli SadeqiNo ratings yet
- Immunization Verification Form 2018Document2 pagesImmunization Verification Form 2018Jawad JamilNo ratings yet
- Covid-19 Vaccination Card (Web)Document2 pagesCovid-19 Vaccination Card (Web)ScribdTranslationsNo ratings yet
- Kindergarten UsirDocument2 pagesKindergarten UsirsoloskojNo ratings yet
- A22M0163DR - ArponDocument7 pagesA22M0163DR - ArponAnton CornelNo ratings yet
- Immunize Form 07282022Document3 pagesImmunize Form 07282022Bishworaj WaibaNo ratings yet
- Baby Shots EngDocument2 pagesBaby Shots Engsunmo8217No ratings yet
- Immunization FormsDocument6 pagesImmunization FormsNadya IrsalinaNo ratings yet
- Immun RecordDocument2 pagesImmun RecordNonofYaNo ratings yet
- J.T. (Cefalozin) Drug StudyDocument2 pagesJ.T. (Cefalozin) Drug StudyAngelica Marie MacaslingNo ratings yet
- 1419-1182 DDIMER-enDocument2 pages1419-1182 DDIMER-enamor kermayaNo ratings yet
- Immunisation Compliance Form 1 2018 Version 5 FinalDocument2 pagesImmunisation Compliance Form 1 2018 Version 5 FinalAnthony Farquhar WuNo ratings yet
- Rhodes Immunization RecordDocument5 pagesRhodes Immunization RecordDr.P.S.N RajuNo ratings yet
- Immunization BlankDocument2 pagesImmunization Blankjeremy.sNo ratings yet
- 3500 (Safty Reporting)Document2 pages3500 (Safty Reporting)api-3810976No ratings yet
- BCCDC Adult Record CardDocument2 pagesBCCDC Adult Record CardYoj SaraNo ratings yet
- Vaccination ReportDocument1 pageVaccination Reportdennis gamisNo ratings yet
- Vaccines - Pharm NotesDocument1 pageVaccines - Pharm NotesErin YoungNo ratings yet
- Instructions For Completion of UA Immunization FormDocument4 pagesInstructions For Completion of UA Immunization FormJ StockmanNo ratings yet
- Guidelines DVT PrimaryDocument2 pagesGuidelines DVT PrimaryRAMARNo ratings yet
- Guidance For Treatment of Covid-19 in Adults and Children: Patient PopulationDocument7 pagesGuidance For Treatment of Covid-19 in Adults and Children: Patient PopulationonkarratheeNo ratings yet
- Screening QuestionnaireDocument2 pagesScreening QuestionnaireKarina RojasNo ratings yet
- covidVaccinationCard 1643563Document1 pagecovidVaccinationCard 1643563Kelvin ChinNo ratings yet
- TB Takeda Dengue Vaccine (TDV - Tak-003) 002 - 2020Document15 pagesTB Takeda Dengue Vaccine (TDV - Tak-003) 002 - 2020rozadinoNo ratings yet
- CUB - Immunisation FormDocument2 pagesCUB - Immunisation FormArcane BeingNo ratings yet
- Ceftriaxone PDFDocument3 pagesCeftriaxone PDFLauren JalandoniNo ratings yet
- CHN Lab - M1Document5 pagesCHN Lab - M1Kristine KimNo ratings yet
- James Madison University Immunization FormDocument1 pageJames Madison University Immunization FormMiguel EspirituNo ratings yet
- CHS Recommended VaccinesDocument1 pageCHS Recommended Vaccineslonzell.brantleyNo ratings yet
- Sindrome Nefrotico Carta El EditorDocument2 pagesSindrome Nefrotico Carta El EditorGerardo de Gyves AvilaNo ratings yet
- Adobe Scan Jun 24, 2021Document2 pagesAdobe Scan Jun 24, 2021Camila Fernandez SandovalNo ratings yet
- Summary Document For Interim Clinical ConsiderationsDocument2 pagesSummary Document For Interim Clinical Considerationssaurabh pandey0% (1)
- Fact Sheet For Health Workers: Paediatric Formulation of Pfizer-Biontech Covid-19 Vaccine, Bnt162B2Document3 pagesFact Sheet For Health Workers: Paediatric Formulation of Pfizer-Biontech Covid-19 Vaccine, Bnt162B2marie-eve guyNo ratings yet
- Name of Drug and Classification Ass.Document7 pagesName of Drug and Classification Ass.Nathalie kate petallarNo ratings yet
- Vaccination Requirements of IFMSA Exchange Progam in Israel-9.15Document2 pagesVaccination Requirements of IFMSA Exchange Progam in Israel-9.15Niko DobrilovicNo ratings yet
- Immunization History FormDocument1 pageImmunization History FormMohammad ShoiabNo ratings yet
- Ins DD en D Dimer Rev.07 150604Document3 pagesIns DD en D Dimer Rev.07 150604Aniket DubeyNo ratings yet
- Booster VaxCardDocument1 pageBooster VaxCardmarialagajino05No ratings yet
- Immunization Record: Form Is Due at OrientationDocument3 pagesImmunization Record: Form Is Due at OrientationCasey JonesNo ratings yet
- Drug Study FormatDocument3 pagesDrug Study Format17melrosefloresNo ratings yet
- Adult Schedule 6x4 5Document2 pagesAdult Schedule 6x4 5dr_ritamNo ratings yet
- Drug Study FormatDocument5 pagesDrug Study FormatVannesa TarifaNo ratings yet
- Varilrix Detail Aid DraftDocument5 pagesVarilrix Detail Aid DraftpheverishNo ratings yet
- Points To Remember in Cold Chain ManagementDocument6 pagesPoints To Remember in Cold Chain Managementpaul arvie violetaNo ratings yet
- Good Health in the Tropics: Advice to Travellers and SettlersFrom EverandGood Health in the Tropics: Advice to Travellers and SettlersNo ratings yet
- TB PDFDocument66 pagesTB PDFKyaw Zin HtetNo ratings yet
- 3RD Quarter Exam in Mapeh 8Document3 pages3RD Quarter Exam in Mapeh 8Arnold LinaoNo ratings yet
- ID Doctors - Application FormDocument6 pagesID Doctors - Application FormGeorgeNo ratings yet
- Pharma Items - Pricelist - Nov 2021Document12 pagesPharma Items - Pricelist - Nov 2021habat albarakah-phgNo ratings yet
- Lampiran Diagnosa Peer Review Puskesmas GondangDocument14 pagesLampiran Diagnosa Peer Review Puskesmas Gondangyugo purwoNo ratings yet
- Dna PDFDocument1 pageDna PDFAhmed SobhNo ratings yet
- 3, Patient Safety - Dr. Santoso S., Spa, MarsDocument55 pages3, Patient Safety - Dr. Santoso S., Spa, Marsendang wildayaniNo ratings yet
- Tuberculosis RegisterDocument91 pagesTuberculosis Registerscribduser0123No ratings yet
- Carga Horária Mensal 04 Códigos Das Habilidades Objetos de ConhecimentosDocument8 pagesCarga Horária Mensal 04 Códigos Das Habilidades Objetos de ConhecimentosRX7 FFNo ratings yet
- African Swine Fever in The PhilippinesDocument5 pagesAfrican Swine Fever in The PhilippinesCathy Baysan Olegario CanoNo ratings yet
- Cap MRDocument4 pagesCap MRKit BarcelonaNo ratings yet
- Oie PDFDocument634 pagesOie PDFFerdinand Prayogo Cahyo SantosoNo ratings yet
- Germ TheoryDocument8 pagesGerm TheoryrasunraNo ratings yet
- Tuberculosis For Dec 1Document23 pagesTuberculosis For Dec 1Tony Rose Reataza-BaylonNo ratings yet
- Laporan Bulanan Hasil Imunisasi Rutin Bayi Dan Batita Bulan: JanuariDocument9 pagesLaporan Bulanan Hasil Imunisasi Rutin Bayi Dan Batita Bulan: JanuariNUR AFIAHNo ratings yet
- Pharmaceutical Reimbursement Access Manager in Austin TX Resume Brian BucklesDocument2 pagesPharmaceutical Reimbursement Access Manager in Austin TX Resume Brian BucklesBrian Buckles100% (1)
- Hiv & Aids Awareness ProgramDocument8 pagesHiv & Aids Awareness ProgramKenzie WalshNo ratings yet
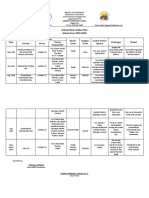
- School Clinic Action Plan 2019Document4 pagesSchool Clinic Action Plan 2019Jenelyn Apinado100% (3)
- Io Rag99972495641165940Document3 pagesIo Rag99972495641165940洛韵漓No ratings yet
- Atrophic Rhinitis: Current ReviewsDocument6 pagesAtrophic Rhinitis: Current ReviewsPrayudo Mahendra PutraNo ratings yet
- Preventing Pink Eye (Conjunctivitis) - CDCDocument2 pagesPreventing Pink Eye (Conjunctivitis) - CDCShaheer ZahidNo ratings yet
- Training On Pfizer Vaccine ManagementDocument132 pagesTraining On Pfizer Vaccine ManagementClaudia YuniarNo ratings yet
- Caseous Lymphadenitis (CL) in Goats and SheepDocument4 pagesCaseous Lymphadenitis (CL) in Goats and SheepMorad ImadNo ratings yet
- COVID Spike Protein Are Induced by Cutting Edge: Circulating Exosomes WithDocument7 pagesCOVID Spike Protein Are Induced by Cutting Edge: Circulating Exosomes WithewewewNo ratings yet
- March Rqs COMPILED BY DR. STRANGEDocument89 pagesMarch Rqs COMPILED BY DR. STRANGEghassan100% (1)
- Zika (1) InfografiaDocument2 pagesZika (1) Infografiaandrea lula da silvaNo ratings yet