You might also like
- Breast Cancer & The Importance Of Vegetables - Based On The Teachings Of Dr. Andrew Huberman: Harnessing Vegetables In The Fight Against Breast CancerFrom EverandBreast Cancer & The Importance Of Vegetables - Based On The Teachings Of Dr. Andrew Huberman: Harnessing Vegetables In The Fight Against Breast CancerNo ratings yet
- 1 s2.0 S0002916522004385 MainDocument11 pages1 s2.0 S0002916522004385 Maincarlos santamariaNo ratings yet
- Impact of Intensive Lifestyle Intervention On Gut Microbiota Composition in Type 2 Diabetes A Post-Hoc Analysis of A Randomized Clinical TrialDocument16 pagesImpact of Intensive Lifestyle Intervention On Gut Microbiota Composition in Type 2 Diabetes A Post-Hoc Analysis of A Randomized Clinical Trialvitoria.cristinaa62No ratings yet
- Nutrients: The Safe and Effective Use of Plant-Based Diets With Guidelines For Health ProfessionalsDocument29 pagesNutrients: The Safe and Effective Use of Plant-Based Diets With Guidelines For Health ProfessionalsProfessor João GuilhermeNo ratings yet
- Impact of Plant - Based Diet in Prevention of Non-Communicable DiseasesDocument7 pagesImpact of Plant - Based Diet in Prevention of Non-Communicable DiseasesIJRASETPublicationsNo ratings yet
- Nutrients 16 00419 v2Document22 pagesNutrients 16 00419 v2ela.sofiaNo ratings yet
- Nutrients: Vegan Diet and The Gut Microbiota Composition in Healthy AdultsDocument14 pagesNutrients: Vegan Diet and The Gut Microbiota Composition in Healthy AdultsMiguel HuangNo ratings yet
- Current Nutritional Therapies in Inflammatory Bowel Disease - Improving Clinical Remission Rates and Sustainability of Long-Term Dietary TherapiesDocument11 pagesCurrent Nutritional Therapies in Inflammatory Bowel Disease - Improving Clinical Remission Rates and Sustainability of Long-Term Dietary TherapiesAdriana SáNo ratings yet
- Review Article Vegetarian Diets, Low-Meat Diets and Health: A ReviewDocument8 pagesReview Article Vegetarian Diets, Low-Meat Diets and Health: A Review专治甲亢赵本山No ratings yet
- Dietary Plants, Gut Microbiota, and Obesity. Effects and Mechanisms-DikonversiDocument18 pagesDietary Plants, Gut Microbiota, and Obesity. Effects and Mechanisms-DikonversiIndri Dewi ListianiNo ratings yet
- Role of Dietary Edible Mushrooms in The Modulation of Gut MicrobiotaDocument12 pagesRole of Dietary Edible Mushrooms in The Modulation of Gut MicrobiotaMartinaNo ratings yet
- Health Benefits of Dietary FibreDocument3 pagesHealth Benefits of Dietary FibreBhimasen SorenNo ratings yet
- Estado Nutricional Adultos en Veganos y No VeganosDocument25 pagesEstado Nutricional Adultos en Veganos y No Veganossimon jaramilloNo ratings yet
- Literature ReviewDocument8 pagesLiterature Reviewvaibhav1504.vsNo ratings yet
- Pro y PrebioticosDocument21 pagesPro y PrebioticosIvan CLNo ratings yet
- Food Ingredients and Suplements - Is This The FutureDocument2 pagesFood Ingredients and Suplements - Is This The FutureDonato CignoliNo ratings yet
- Nutrigenomics Research: A ReviewDocument14 pagesNutrigenomics Research: A ReviewpuspitaNo ratings yet
- Probiotics: Complementary and Alternative Medicine: A New SeriesDocument3 pagesProbiotics: Complementary and Alternative Medicine: A New SeriesKarol CañasNo ratings yet
- Nutrients: Mediterranean Diet On Sleep: A Health AllianceDocument29 pagesNutrients: Mediterranean Diet On Sleep: A Health AllianceJIMENA CLAUDIA PANTOJA RICONo ratings yet
- Nutrition Basics How It Functions and Healthy GuidelinesDocument2 pagesNutrition Basics How It Functions and Healthy GuidelinesYasmine BournineNo ratings yet
- Nutrients 11 00947Document13 pagesNutrients 11 00947vinanugraha09No ratings yet
- Gut Microbiota-Targeted Diets Modulate Human Immune StatusDocument42 pagesGut Microbiota-Targeted Diets Modulate Human Immune StatussimasNo ratings yet
- Modulation of The Gastrointestinal Microbiome With Nondigestible Fermentable Carbohydrates To Improve Human HealthDocument35 pagesModulation of The Gastrointestinal Microbiome With Nondigestible Fermentable Carbohydrates To Improve Human HealthslothwonNo ratings yet
- Nutrients: Can Gut Microbiota Composition Predict Response To Dietary Treatments?Document15 pagesNutrients: Can Gut Microbiota Composition Predict Response To Dietary Treatments?Meisya Nur'ainiNo ratings yet
- DR MIKhanetal 2021Document14 pagesDR MIKhanetal 2021Meow Vendo PermutoNo ratings yet
- Tapsell Et Al. 2023Document17 pagesTapsell Et Al. 2023albertsalas1No ratings yet
- PIIS2475299124000118Document18 pagesPIIS2475299124000118Reeds LaurelNo ratings yet
- Campmans-Kuijpers 2021 IBDDocument34 pagesCampmans-Kuijpers 2021 IBDNovita ApramadhaNo ratings yet
- Nutrients 12 02474Document15 pagesNutrients 12 02474Robert StryjakNo ratings yet
- Medicina: Nutritional Status and The Influence of The Vegan Diet On The Gut Microbiota and Human HealthDocument15 pagesMedicina: Nutritional Status and The Influence of The Vegan Diet On The Gut Microbiota and Human HealthCem Tunaboylu (Student)No ratings yet
- Review: Dong D Wang, Frank B HuDocument11 pagesReview: Dong D Wang, Frank B HuNathannael MendoncaNo ratings yet
- Materi Dr. MayaDocument33 pagesMateri Dr. MayaNishi RuciNo ratings yet
- Review: Stephanie Jew, Suhad S. Abumweis, and Peter J.H. JonesDocument10 pagesReview: Stephanie Jew, Suhad S. Abumweis, and Peter J.H. JonesJosé OrtízNo ratings yet
- Nutrients 15 02591 v2Document29 pagesNutrients 15 02591 v2akumakuja graffelNo ratings yet
- Pulse Crop Effects On Gut Microbial Populations, Intestinal Function, and Adiposity in A Mouse Model of Diet-Induced Obesity John N. McginleyDocument40 pagesPulse Crop Effects On Gut Microbial Populations, Intestinal Function, and Adiposity in A Mouse Model of Diet-Induced Obesity John N. Mcginleyzora.mendez637100% (8)
- Nutrients: AbstractDocument18 pagesNutrients: AbstractLucasVasconcelosNo ratings yet
- High Animal Protein Diet and Gut Microbiota in Human HealthDocument14 pagesHigh Animal Protein Diet and Gut Microbiota in Human HealthAntonio Rodríguez SánchezNo ratings yet
- DietaDocument12 pagesDietaSilviaNo ratings yet
- Efficacy of The Autoimmune Protocol Diet For Inflammatory Bowel DiseaseDocument7 pagesEfficacy of The Autoimmune Protocol Diet For Inflammatory Bowel DiseaseNejc KovačNo ratings yet
- Fnut 09 741630Document10 pagesFnut 09 741630gabrielavk95No ratings yet
- 25909-Article Text-86090-1-18-20240313Document13 pages25909-Article Text-86090-1-18-20240313aliciajeumpaNo ratings yet
- Improving Diet Sustainability Through Evolution of Food Choices: Review of Epidemiological Studies On The Environmental Impact of DietsDocument16 pagesImproving Diet Sustainability Through Evolution of Food Choices: Review of Epidemiological Studies On The Environmental Impact of DietsJuan Jose Ramos SierraNo ratings yet
- Jurnal AlergiDocument7 pagesJurnal AlergiNursyamsuddin MoganaNo ratings yet
- Microorganisms 10 00452 v2Document15 pagesMicroorganisms 10 00452 v2V.EricSson BaPtisTaNo ratings yet
- Nutrients 15 00332 v2Document17 pagesNutrients 15 00332 v2koehler.thereseNo ratings yet
- Diet-Microbiota Interactions in Inflammatory Bowel DiseaseDocument17 pagesDiet-Microbiota Interactions in Inflammatory Bowel DiseaseIsabella María GantivarNo ratings yet
- Nutrients 12 01921 PDFDocument26 pagesNutrients 12 01921 PDFdianamsaucedoNo ratings yet
- Nutrients 14 00379Document5 pagesNutrients 14 00379jhonatan mataNo ratings yet
- Nutrients 14 00892Document23 pagesNutrients 14 00892TRABAJOS DR. MÜSEL TABARESNo ratings yet
- Ous Salah 2020Document25 pagesOus Salah 2020Syahriphona FitrianiNo ratings yet
- Nutrients 14 00023 v5Document38 pagesNutrients 14 00023 v5Andrés ZapataNo ratings yet
- Interindividual Variability in Gut Microbiota and Host Response To Dietary InterventionsDocument22 pagesInterindividual Variability in Gut Microbiota and Host Response To Dietary InterventionsDiogoNo ratings yet
- Aliment Pharmacol Ther - 2020 - Caenepeel - Review Article How The Intestinal Microbiota May Reflect DisDocument16 pagesAliment Pharmacol Ther - 2020 - Caenepeel - Review Article How The Intestinal Microbiota May Reflect DisarifsyahsulaimanbbNo ratings yet
- Potential Health Bene Fits of Combining Yogurt and Fruits Based On Their Probiotic and Prebiotic PropertiesDocument10 pagesPotential Health Bene Fits of Combining Yogurt and Fruits Based On Their Probiotic and Prebiotic PropertiesMaja CosmoNo ratings yet
- 1 s2.0 S0002916523463034 MainDocument13 pages1 s2.0 S0002916523463034 Maincarlos santamariaNo ratings yet
- Dietary Assessment Methods in Epidemiologic Studies: Epidemiology and HealthDocument8 pagesDietary Assessment Methods in Epidemiologic Studies: Epidemiology and Healthsuhada.akmalNo ratings yet
- Personalised Nutrition: Updates, Gaps and Next Steps: EditorialDocument5 pagesPersonalised Nutrition: Updates, Gaps and Next Steps: EditorialMeisya Nur'ainiNo ratings yet
- Nutrients: Nutrients, Infectious and Inflammatory DiseasesDocument9 pagesNutrients: Nutrients, Infectious and Inflammatory DiseasesAnggita Widya YonitaNo ratings yet
- EMBO Mol Med - 2021 - Allen - Metabolomics Insights Into Plant Based DietsDocument2 pagesEMBO Mol Med - 2021 - Allen - Metabolomics Insights Into Plant Based Dietsgipanef547No ratings yet
- Assessment of Nutrient Intake and Physical Activity Pattern in Vegetarian Geriatric Population, Aged 60-70 YearsDocument7 pagesAssessment of Nutrient Intake and Physical Activity Pattern in Vegetarian Geriatric Population, Aged 60-70 YearsIJAR JOURNALNo ratings yet
- Widespread Protein Lysine Acetylation in Gut Microbiome and Its Alterations in Patients With Crohn's DiseaseDocument12 pagesWidespread Protein Lysine Acetylation in Gut Microbiome and Its Alterations in Patients With Crohn's DiseaseMartinaNo ratings yet
- Safety, Clinical Response, and Microbiome Findings Following Fecal Microbiota Transplant in Children With Inflammatory Bowel DiseaseDocument12 pagesSafety, Clinical Response, and Microbiome Findings Following Fecal Microbiota Transplant in Children With Inflammatory Bowel DiseaseMartinaNo ratings yet
- Fecal Microbiota Transplant For Crohn Disease - ADocument8 pagesFecal Microbiota Transplant For Crohn Disease - AMartinaNo ratings yet
- Microbiome in Sjögren's Syndrome - Here We AreDocument2 pagesMicrobiome in Sjögren's Syndrome - Here We AreMartinaNo ratings yet
- The Microbiome and Hepatocellular CarcinomaDocument29 pagesThe Microbiome and Hepatocellular CarcinomaMartinaNo ratings yet
- A Microbiome Foundation For The Study of Crohn's DiseaseDocument4 pagesA Microbiome Foundation For The Study of Crohn's DiseaseMartinaNo ratings yet
- A Comparative Proteomic Analysis of Erinacine A's Inhibition of Gastric Cancer Cell Viability and InvasivenessDocument14 pagesA Comparative Proteomic Analysis of Erinacine A's Inhibition of Gastric Cancer Cell Viability and InvasivenessMartinaNo ratings yet
- The Relationship Between Fecal Bile Acids and Microbiome CounityDocument12 pagesThe Relationship Between Fecal Bile Acids and Microbiome CounityMartinaNo ratings yet
- Iron Fortification Adversely Affects The Gut ..Document12 pagesIron Fortification Adversely Affects The Gut ..MartinaNo ratings yet
- Assessment of Complementary Feeding of Canadian Infants - Effects On Microbiome & Oxidative Stress, A Randomized Controlled TrialDocument12 pagesAssessment of Complementary Feeding of Canadian Infants - Effects On Microbiome & Oxidative Stress, A Randomized Controlled TrialMartinaNo ratings yet
- Decreased Fecal Calprotectin Levels in Cystic Fibrosis Patients After Antibiotic Treatment For Respiratory ExacerbationDocument3 pagesDecreased Fecal Calprotectin Levels in Cystic Fibrosis Patients After Antibiotic Treatment For Respiratory ExacerbationMartinaNo ratings yet
- Molecules: Ffects of Rich in B-Glucans Edible MushroomsDocument25 pagesMolecules: Ffects of Rich in B-Glucans Edible Mushroomsharry potterNo ratings yet
- Fecal Calprotectin and Fecal Indole Predict Outcome of FecalDocument4 pagesFecal Calprotectin and Fecal Indole Predict Outcome of FecalMartinaNo ratings yet
- Blastocystis Gut MicrobiomeDocument18 pagesBlastocystis Gut MicrobiomeFreddy FranklinNo ratings yet
- The Gut Microbiome As A Target For IBD Treatment - Are We There YetDocument12 pagesThe Gut Microbiome As A Target For IBD Treatment - Are We There YetMartinaNo ratings yet
- Carbohydrate (HC), Mediterranean (MD) and Western (WD) Diets. HC WasDocument2 pagesCarbohydrate (HC), Mediterranean (MD) and Western (WD) Diets. HC WasMartinaNo ratings yet
- Izab 277Document10 pagesIzab 277MartinaNo ratings yet
- Polysaccharides From Natural Resources Exhibit Great Potential in The Treatment of Ulcerative Colitis - A ReviewDocument12 pagesPolysaccharides From Natural Resources Exhibit Great Potential in The Treatment of Ulcerative Colitis - A ReviewMartinaNo ratings yet
- Health Benefits of Edible Mushroom Polysaharidesand Associated Gut Microbiota RegulationDocument19 pagesHealth Benefits of Edible Mushroom Polysaharidesand Associated Gut Microbiota RegulationMartinaNo ratings yet
- Molecules: Ffects of Rich in B-Glucans Edible MushroomsDocument25 pagesMolecules: Ffects of Rich in B-Glucans Edible Mushroomsharry potterNo ratings yet
- Microbiome Risk Profiles As Biomarkers For Inflammatory and Metabolic DisordersDocument15 pagesMicrobiome Risk Profiles As Biomarkers For Inflammatory and Metabolic DisordersMartinaNo ratings yet
- Hericium Erinaceus, An Amazing Medicinal MushroomDocument24 pagesHericium Erinaceus, An Amazing Medicinal MushroomMartinaNo ratings yet
- The Researchers To Design, Research, and Develop New Drugs ForDocument19 pagesThe Researchers To Design, Research, and Develop New Drugs ForMartinaNo ratings yet
- Clinical and Physiological Perspectives of βGlucans in The Past, Present, and FutureDocument48 pagesClinical and Physiological Perspectives of βGlucans in The Past, Present, and FutureQualityMattersNo ratings yet
- Recent Developments in Hericium Erinaceus Polysaccharides - Extraction, Purifacion, Structur Characterist and Biology ActivityDocument21 pagesRecent Developments in Hericium Erinaceus Polysaccharides - Extraction, Purifacion, Structur Characterist and Biology ActivityMartinaNo ratings yet
- A Review of The Effects of Natural Compounds, Medical Plants, Mushrooms On Thegut Microbiota and Colitis and CancerDocument8 pagesA Review of The Effects of Natural Compounds, Medical Plants, Mushrooms On Thegut Microbiota and Colitis and CancerMartinaNo ratings yet
- Internal Connections Between Dietary Intake and Gut Microbiota Homeostasis in Disease Progression of Ulcerative Colitis - A ReviewDocument12 pagesInternal Connections Between Dietary Intake and Gut Microbiota Homeostasis in Disease Progression of Ulcerative Colitis - A ReviewMartinaNo ratings yet
- The Researchers To Design, Research, and Develop New Drugs ForDocument19 pagesThe Researchers To Design, Research, and Develop New Drugs ForMartinaNo ratings yet
- The Role of Gut Microbiota Biomodulators On Mucosal Imuniti and Intestinal InflamationDocument24 pagesThe Role of Gut Microbiota Biomodulators On Mucosal Imuniti and Intestinal InflamationMartinaNo ratings yet
- A Review of Mushrooms in Human Nutrition and HealthDocument14 pagesA Review of Mushrooms in Human Nutrition and HealthBegoña MartinezNo ratings yet
- Income Tax Law & Practice Code: BBA-301 Unit - 2: Ms. Manisha Sharma Asst. ProfessorDocument32 pagesIncome Tax Law & Practice Code: BBA-301 Unit - 2: Ms. Manisha Sharma Asst. ProfessorVasu NarangNo ratings yet
- Skott Marsi Art Basel Sponsorship DeckDocument11 pagesSkott Marsi Art Basel Sponsorship DeckANTHONY JACQUETTENo ratings yet
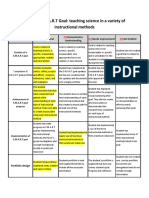
- Smart Goals Rubric 2Document2 pagesSmart Goals Rubric 2api-338549230100% (2)
- Some People Say That Having Jobs Can Be of Great Benefit To TeensDocument2 pagesSome People Say That Having Jobs Can Be of Great Benefit To Teensmaia sulavaNo ratings yet
- Peri Komponentu Katalogas Pastoliams 2015 enDocument372 pagesPeri Komponentu Katalogas Pastoliams 2015 enLim Yew KwangNo ratings yet
- Rtcclient Tool Quick Guide: Date Jan. 25, 2011Document3 pagesRtcclient Tool Quick Guide: Date Jan. 25, 2011curzNo ratings yet
- Class 1Document19 pagesClass 1Rahul BharadwajNo ratings yet
- Door LockDocument102 pagesDoor LockNicolás BozzoNo ratings yet
- Safety Data Sheet: Armohib Ci-28Document21 pagesSafety Data Sheet: Armohib Ci-28SJHEIK AbdullahNo ratings yet
- LGC CasesDocument97 pagesLGC CasesJeshe BalsomoNo ratings yet
- Request For Refund or Test Date Transfer FormDocument2 pagesRequest For Refund or Test Date Transfer FormAhmed Hamdy100% (1)
- Picket Fence LabDocument3 pagesPicket Fence Labapi-236349398No ratings yet
- LogisticsDocument5 pagesLogisticsHương LýNo ratings yet
- Fruit and Vegetable Wash TdsDocument1 pageFruit and Vegetable Wash TdsEsheshNo ratings yet
- Case Study-Hain Celestial: Student Name Institution Affiliation DateDocument5 pagesCase Study-Hain Celestial: Student Name Institution Affiliation DategeofreyNo ratings yet
- 01 04 2018Document55 pages01 04 2018sagarNo ratings yet
- Goran BULDIOSKI THINK TANKS IN CENTRAL AND EASTERN EUROPE AND THE QUALITY OF THEIR POLICY RESEARCHDocument31 pagesGoran BULDIOSKI THINK TANKS IN CENTRAL AND EASTERN EUROPE AND THE QUALITY OF THEIR POLICY RESEARCHCentre for Regional Policy Research and Cooperation StudiorumNo ratings yet
- A Brief On "The Purvanchal Expressway"Document4 pagesA Brief On "The Purvanchal Expressway"Ajay SinghNo ratings yet
- Questionnaire For National Security Positions: Purpose of This FormDocument36 pagesQuestionnaire For National Security Positions: Purpose of This Formadad1lqNo ratings yet
- Warm Mix Asphalt: "National Perspective"Document46 pagesWarm Mix Asphalt: "National Perspective"Royhan RizkyNo ratings yet
- G1 - Introduction Generator ProtectionDocument21 pagesG1 - Introduction Generator ProtectionOoi Ban JuanNo ratings yet
- The Object-Z Specification Language: Software Verification Research Centre University of QueenslandDocument155 pagesThe Object-Z Specification Language: Software Verification Research Centre University of QueenslandJulian Garcia TalanconNo ratings yet
- IT2840D 3640D Copier Operation ManualDocument516 pagesIT2840D 3640D Copier Operation ManualChristopher CollinsNo ratings yet
- Flight Eticket - PdfaaaDocument3 pagesFlight Eticket - PdfaaaIgnacio Gonzalez PastranoNo ratings yet
- Selenium Question and AnswerDocument35 pagesSelenium Question and AnswerManas Jha50% (2)
- CHP For AjmerDocument343 pagesCHP For AjmerHarsh Shah33% (3)
- Paving The Path To Narrowband 5G With Lte Internet of Things (Iot)Document16 pagesPaving The Path To Narrowband 5G With Lte Internet of Things (Iot)Matt ValroseNo ratings yet
- 08147-416H - LEGEND - Wahl - Fact Sheets - 5StarSeries - GBDocument1 page08147-416H - LEGEND - Wahl - Fact Sheets - 5StarSeries - GBChristian ParedesNo ratings yet
- Evolution of Human Resource ManagementDocument13 pagesEvolution of Human Resource Managementmsk_1407No ratings yet
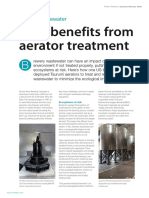
- Beer Benefits From Aerator TreatmentDocument2 pagesBeer Benefits From Aerator TreatmentSam MurrayNo ratings yet
- Instant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookFrom EverandInstant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookRating: 3.5 out of 5 stars3.5/5 (2)
- Body Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomFrom EverandBody Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomRating: 4 out of 5 stars4/5 (1)
- The Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyFrom EverandThe Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyNo ratings yet
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisFrom EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisRating: 3 out of 5 stars3/5 (2)
- Summary of Mary Claire Haver's The Galveston DietFrom EverandSummary of Mary Claire Haver's The Galveston DietRating: 5 out of 5 stars5/5 (1)
- Forever Strong: A New, Science-Based Strategy for Aging WellFrom EverandForever Strong: A New, Science-Based Strategy for Aging WellNo ratings yet
- Gut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)From EverandGut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Rating: 4 out of 5 stars4/5 (378)
- The Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingFrom EverandThe Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingRating: 4 out of 5 stars4/5 (3)
- Metabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeFrom EverandMetabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeNo ratings yet
- Intermittent Fasting Basics for Women: The Complete Guide to Safe and Effective Weight Loss with Intermittent FastingFrom EverandIntermittent Fasting Basics for Women: The Complete Guide to Safe and Effective Weight Loss with Intermittent FastingRating: 5 out of 5 stars5/5 (12)
- Sugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthFrom EverandSugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthRating: 4 out of 5 stars4/5 (6)
- The Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonFrom EverandThe Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonRating: 3.5 out of 5 stars3.5/5 (33)
- The Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyFrom EverandThe Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyRating: 4.5 out of 5 stars4.5/5 (2)
- Eat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouFrom EverandEat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouNo ratings yet
- The Diet Trap Solution: Train Your Brain to Lose Weight and Keep It Off for GoodFrom EverandThe Diet Trap Solution: Train Your Brain to Lose Weight and Keep It Off for GoodNo ratings yet
- The Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthFrom EverandThe Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthNo ratings yet
- Secrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainFrom EverandSecrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainRating: 3.5 out of 5 stars3.5/5 (38)
- The Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsFrom EverandThe Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsRating: 4 out of 5 stars4/5 (49)
- Find Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeFrom EverandFind Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeRating: 4 out of 5 stars4/5 (3)
- Keto Friendly Recipes: Easy Keto For Busy PeopleFrom EverandKeto Friendly Recipes: Easy Keto For Busy PeopleRating: 3.5 out of 5 stars3.5/5 (2)
- How Not to Die by Michael Greger MD, Gene Stone - Book Summary: Discover the Foods Scientifically Proven to Prevent and Reverse DiseaseFrom EverandHow Not to Die by Michael Greger MD, Gene Stone - Book Summary: Discover the Foods Scientifically Proven to Prevent and Reverse DiseaseRating: 4.5 out of 5 stars4.5/5 (83)
- The End of Craving: Recovering the Lost Wisdom of Eating WellFrom EverandThe End of Craving: Recovering the Lost Wisdom of Eating WellRating: 4.5 out of 5 stars4.5/5 (80)
- Rapid Weight Loss Hypnosis: Deep Sleep Your Way to Rapid Weight Loss, Healing Your Body and Self Esteem with Guided Meditations and Positive AffirmationsFrom EverandRapid Weight Loss Hypnosis: Deep Sleep Your Way to Rapid Weight Loss, Healing Your Body and Self Esteem with Guided Meditations and Positive AffirmationsRating: 5 out of 5 stars5/5 (7)
- How to Be Well: The 6 Keys to a Happy and Healthy LifeFrom EverandHow to Be Well: The 6 Keys to a Happy and Healthy LifeRating: 5 out of 5 stars5/5 (1)
- Happy Gut: The Cleansing Program to Help You Lose Weight, Gain Energy, and Eliminate PainFrom EverandHappy Gut: The Cleansing Program to Help You Lose Weight, Gain Energy, and Eliminate PainRating: 3.5 out of 5 stars3.5/5 (6)
- Proteinaholic: How Our Obsession with Meat Is Killing Us and What We Can Do About ItFrom EverandProteinaholic: How Our Obsession with Meat Is Killing Us and What We Can Do About ItRating: 4.5 out of 5 stars4.5/5 (19)
- Foods That Cause You to Lose Weight: The Negative Calorie EffectFrom EverandFoods That Cause You to Lose Weight: The Negative Calorie EffectRating: 3 out of 5 stars3/5 (5)