You might also like
- Shear Wave ElastographyDocument8 pagesShear Wave ElastographySyed JameelNo ratings yet
- Techniques To Lower CT Dose: by Patricia Zoltowski, Clinical Educator, CT Global MarketingDocument3 pagesTechniques To Lower CT Dose: by Patricia Zoltowski, Clinical Educator, CT Global MarketingekajuliantaraNo ratings yet
- Basics of GlaucomaDocument12 pagesBasics of GlaucomaJatinderBaliNo ratings yet
- Ge Signa LX 1 5tDocument2 pagesGe Signa LX 1 5tFaye WilliamsNo ratings yet
- 9485 R0 NuNec Surgical Technique 8-30-16Document24 pages9485 R0 NuNec Surgical Technique 8-30-16BobNo ratings yet
- ACNS (09B) Guidelines On Visual Evoked PotentialsDocument20 pagesACNS (09B) Guidelines On Visual Evoked PotentialsmonihhmmNo ratings yet
- Appli Pleno IshizakaDocument5 pagesAppli Pleno IshizakaFazaia KckNo ratings yet
- Summit Tecnica Quirurgica 1Document28 pagesSummit Tecnica Quirurgica 1alma mariaNo ratings yet
- Guideline 9BDocument20 pagesGuideline 9BMaryam ZangenehNo ratings yet
- Keratometry: Kerato Cornea Metry MeasurementDocument12 pagesKeratometry: Kerato Cornea Metry MeasurementMarlya AlenaNo ratings yet
- Use of eFAST in Patients With Injury To The Thorax or AbdomenDocument4 pagesUse of eFAST in Patients With Injury To The Thorax or Abdomenalejandro montesNo ratings yet
- Guideline 9BDocument20 pagesGuideline 9BLulu SupergirlNo ratings yet
- Te 1667 WebDocument3 pagesTe 1667 WebeguleamrNo ratings yet
- Vertigo SelvarajanDocument41 pagesVertigo SelvarajanKarthik KarthikNo ratings yet
- Csi Plan Writeup Portion Turn in PDFDocument13 pagesCsi Plan Writeup Portion Turn in PDFapi-481226212No ratings yet
- The Use of Force Plate Posturography in The Assessment of Postural Instability 2016 Gait PostureDocument6 pagesThe Use of Force Plate Posturography in The Assessment of Postural Instability 2016 Gait PostureDefprimalNo ratings yet
- Etter 1963Document3 pagesEtter 1963Elsya PutriNo ratings yet
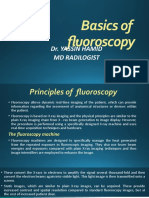
- Basics of FlourosDocument35 pagesBasics of FlourosFamousmanNo ratings yet
- Biopsy Guide Operator Manual - English - UM - 2373241-100 - 000Document16 pagesBiopsy Guide Operator Manual - English - UM - 2373241-100 - 000Wilmer ValderramaNo ratings yet
- Csi Treatment Plan WriteupDocument17 pagesCsi Treatment Plan Writeupapi-632529930No ratings yet
- Basic of CBCT ImagingDocument7 pagesBasic of CBCT ImagingIndah VitasariNo ratings yet
- Biometry by Suryakant Jha and Wangchuk Doma PDFDocument5 pagesBiometry by Suryakant Jha and Wangchuk Doma PDFJavier Andrés Pinochet SantoroNo ratings yet
- Errores de Posicionamiento en Un OrtopantomografoDocument14 pagesErrores de Posicionamiento en Un OrtopantomografoVicenteNo ratings yet
- Practical Guidance in Echocardiographic Assessment of Global Longitudinal StrainDocument4 pagesPractical Guidance in Echocardiographic Assessment of Global Longitudinal StrainMathew McCarthyNo ratings yet
- Design and Analysis of HSC-BPPV Diagnostic ManeuveDocument11 pagesDesign and Analysis of HSC-BPPV Diagnostic ManeuveSelinay YAȘANo ratings yet
- Week 8 Lab 7 Knee and Tibia and FibulaDocument12 pagesWeek 8 Lab 7 Knee and Tibia and FibulamaddisonaturnerNo ratings yet
- Assessment of Corneal Biomechanics, Tonometry and Pachymetry With The Corvis ST in MyopiaDocument10 pagesAssessment of Corneal Biomechanics, Tonometry and Pachymetry With The Corvis ST in Myopiavergarajaviera548No ratings yet
- An in Vitro Comparison of The Accuracy of MeasurementsDocument4 pagesAn in Vitro Comparison of The Accuracy of Measurementsgileno pagamentosNo ratings yet
- Recommendations On The Use of Ultrasound Guidance For Adult Lumbar Puncture: A Position Statement of The Society of Hospital MedicineDocument12 pagesRecommendations On The Use of Ultrasound Guidance For Adult Lumbar Puncture: A Position Statement of The Society of Hospital MedicineSandrita ArmijosNo ratings yet
- Trollbyte Plus ManualDocument12 pagesTrollbyte Plus ManualSava xNo ratings yet
- Automated Romberg Testing in Patients With Benign Paroxysmal Positional Vertigo and Healthy SubjectsDocument9 pagesAutomated Romberg Testing in Patients With Benign Paroxysmal Positional Vertigo and Healthy SubjectsDjumadi AkbarNo ratings yet
- 12 - Objective RefractionDocument11 pages12 - Objective RefractionSumon SarkarNo ratings yet
- Eang2015 PDFDocument4 pagesEang2015 PDFHoun SophatNo ratings yet
- Cephalometric RadiographyDocument8 pagesCephalometric Radiographymkhaddas100% (3)
- Prosound - Alpha 6 - E-Catalogue PDFDocument6 pagesProsound - Alpha 6 - E-Catalogue PDFzoheb baigNo ratings yet
- Elastq Shear Imaging Liver WhitepaperDocument8 pagesElastq Shear Imaging Liver WhitepaperGOMEDICAGSNo ratings yet
- (White Paper) RS85 S-Shearwave Imaging Breast - 0306 - FinalDocument9 pages(White Paper) RS85 S-Shearwave Imaging Breast - 0306 - Finalultrasound tomNo ratings yet
- 1 s2.0 S0016510703025082 MainDocument8 pages1 s2.0 S0016510703025082 MainJosé Moreira Lima NetoNo ratings yet
- Esaote - GI - QElaXto 2D Quick Guide - Final - v2Document3 pagesEsaote - GI - QElaXto 2D Quick Guide - Final - v2vinh nguyễn phướcNo ratings yet
- Auto Couch Height Positioning Compensation - Making SUREExposure A Smarter Dose Reduction ToolDocument5 pagesAuto Couch Height Positioning Compensation - Making SUREExposure A Smarter Dose Reduction ToolAbdalhakeem AlturkyNo ratings yet
- Elastography Quick Guide-Breast and ThyroidDocument12 pagesElastography Quick Guide-Breast and ThyroiduyabmantriNo ratings yet
- CBCT in Endodontics: Presented By: DR - Saloni PG Student Dept. of Cons and EndoDocument83 pagesCBCT in Endodontics: Presented By: DR - Saloni PG Student Dept. of Cons and Endosaloni singhNo ratings yet
- Clinical Instrumentation in Contact Lens PracticeDocument1 pageClinical Instrumentation in Contact Lens PracticeRael Rodrigues Dos SantosNo ratings yet
- Group 1 Froggle Bunwich Lab Activity 2Document10 pagesGroup 1 Froggle Bunwich Lab Activity 2Belyn CancioNo ratings yet
- Vacora IFU MultilingueDocument84 pagesVacora IFU MultilingueJose QuiscaNo ratings yet
- Control Systems Engineering 5 (1) - 4Document1 pageControl Systems Engineering 5 (1) - 4ANo ratings yet
- Can We Perform CT of The Appendix With Less Than 1 MSV? A De-Escalating Dose-Simulation StudyDocument9 pagesCan We Perform CT of The Appendix With Less Than 1 MSV? A De-Escalating Dose-Simulation StudyKostiantyn BiriukovNo ratings yet
- An Important Technique - Use of The Microscope: VCE BiologyDocument18 pagesAn Important Technique - Use of The Microscope: VCE BiologyC CdNo ratings yet
- The Impact of Focal Spot Size On Clinical ImagesDocument11 pagesThe Impact of Focal Spot Size On Clinical ImagesSOHON SINHA MAHAPATRANo ratings yet
- Clinical Oncology AssignmentDocument18 pagesClinical Oncology Assignmentapi-631272802No ratings yet
- Csi Write UpDocument15 pagesCsi Write Upapi-632827798No ratings yet
- Understands: It Your EverydayDocument8 pagesUnderstands: It Your EverydayCándido GuzmánNo ratings yet
- Scope Guide Quick Reference GuideDocument2 pagesScope Guide Quick Reference GuideJulia HammoudNo ratings yet
- Week 7 Lab 6 Feet and AnkleDocument13 pagesWeek 7 Lab 6 Feet and AnklemaddisonaturnerNo ratings yet
- Diagnostic of CyclodeviationDocument4 pagesDiagnostic of CyclodeviationRozalinaNo ratings yet
- Wiku Andotopo - Tips and Tricks Us Color Doppler in Human Rep (Drwiku)Document14 pagesWiku Andotopo - Tips and Tricks Us Color Doppler in Human Rep (Drwiku)Denny LukasNo ratings yet
- R3 Poly US STDocument24 pagesR3 Poly US STAgung TristyantoNo ratings yet
- Op XG 3dready XG 3D Patient PositioningDocument1 pageOp XG 3dready XG 3D Patient PositioningROGERQUIROZNo ratings yet
- Appleton School Student Health ReportDocument21 pagesAppleton School Student Health ReportJonathan KrauseNo ratings yet
- Color Me Happy Coloring BookDocument36 pagesColor Me Happy Coloring BookSabrina Shortt100% (1)
- The PILOT - January 2022Document24 pagesThe PILOT - January 2022RSCA Redwood ShoresNo ratings yet
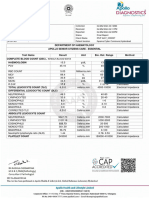
- Apollo247 250313622 Labreport 220 1709549589491Document4 pagesApollo247 250313622 Labreport 220 1709549589491mariarubyjohn18No ratings yet
- Alvin ApplicationDocument7 pagesAlvin ApplicationAlvin NovencidoNo ratings yet
- Fulfilling Your Sexual PotentialDocument11 pagesFulfilling Your Sexual PotentialDorothy Hayden0% (1)
- Final ReportDocument27 pagesFinal ReportHanan KemalNo ratings yet
- Daftar Pegawai PKM Ibun Februari 2023Document3 pagesDaftar Pegawai PKM Ibun Februari 2023syauqiNo ratings yet
- OHS-PR-09-03-F07 JOB SAFE PROCEDURE (15) Stringing Pulling Conductor and OPGW-JSPDocument18 pagesOHS-PR-09-03-F07 JOB SAFE PROCEDURE (15) Stringing Pulling Conductor and OPGW-JSPmohammed tofiqNo ratings yet
- 2 Risk Assessment Template - Situation 1Document10 pages2 Risk Assessment Template - Situation 1Menol KulathungaNo ratings yet
- Banksman Barricades and SignsDocument15 pagesBanksman Barricades and SignsAmirNo ratings yet
- LMMU September 2022 ADVERT - 1Document9 pagesLMMU September 2022 ADVERT - 1FredroNo ratings yet
- Cse 485 - L9 PDFDocument62 pagesCse 485 - L9 PDFRakesh PatelNo ratings yet
- Final Announcement KOPAPDI XVIII Semarang 2022Document25 pagesFinal Announcement KOPAPDI XVIII Semarang 2022Ayu Ika PuspitaNo ratings yet
- Demo Request Form - ECOBAG - PSADocument12 pagesDemo Request Form - ECOBAG - PSAAllyssa BuenaventuraNo ratings yet
- VersaSonic-SDS-1 05 22Document2 pagesVersaSonic-SDS-1 05 22Construccion MantenimientoNo ratings yet
- Result RBT 0.5 Part Test 5 JEE Main Class 12thDocument7 pagesResult RBT 0.5 Part Test 5 JEE Main Class 12thdibakarde72No ratings yet
- The Essential Guide To Brain Tumors PDFDocument43 pagesThe Essential Guide To Brain Tumors PDFA Farid WajdyNo ratings yet
- Pediatric Iga Nephropathy in Europe: Review ArticleDocument7 pagesPediatric Iga Nephropathy in Europe: Review ArticleAmabelle PanganibanNo ratings yet
- InterviewDocument2 pagesInterviewMarjorie DuranNo ratings yet
- Tau AngleDocument5 pagesTau AngleMSHNo ratings yet
- Factors Affecting Adherence To Infant Immunization University of Thephilippines ManilaDocument1 pageFactors Affecting Adherence To Infant Immunization University of Thephilippines Manilaheidi leeNo ratings yet
- Melkisedek O. Nubatonis: Jurnal Info KesehatanDocument18 pagesMelkisedek O. Nubatonis: Jurnal Info KesehatanAtika DelianaNo ratings yet
- User - S - Manual Thermometer PDFDocument22 pagesUser - S - Manual Thermometer PDFjuanNo ratings yet
- Panic Disorder OverviewDocument8 pagesPanic Disorder OverviewVasaviNo ratings yet
- M788 SDSDocument15 pagesM788 SDSYusuf Emre ÇABUKOĞLUNo ratings yet
- BCL2L12 Gene Expression of Human Prostate Adenocarcinoma Cell Line inDocument7 pagesBCL2L12 Gene Expression of Human Prostate Adenocarcinoma Cell Line inDanyal KhanNo ratings yet
- BG4 Maint Training Manual Rev1 2019Document163 pagesBG4 Maint Training Manual Rev1 2019zeeshan muneerNo ratings yet
- Whipple Procedure: Procedure at A GlanceDocument4 pagesWhipple Procedure: Procedure at A GlanceAze Andrea PutraNo ratings yet
- Nursing Care Plan For Schizophrenic PatientsDocument6 pagesNursing Care Plan For Schizophrenic PatientsHARVEY SELIMNo ratings yet
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Rating: 3 out of 5 stars3/5 (1)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (4)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeFrom EverandThe Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeRating: 4.5 out of 5 stars4.5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (39)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 4.5 out of 5 stars4.5/5 (83)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 4 out of 5 stars4/5 (5)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- I Shouldn't Feel This Way: Name What’s Hard, Tame Your Guilt, and Transform Self-Sabotage into Brave ActionFrom EverandI Shouldn't Feel This Way: Name What’s Hard, Tame Your Guilt, and Transform Self-Sabotage into Brave ActionNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (170)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (267)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesFrom EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesRating: 4.5 out of 5 stars4.5/5 (1412)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (44)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (256)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (46)
- Summary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (61)
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (39)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet