You might also like
- Genital Herpes: Clinical PracticeDocument9 pagesGenital Herpes: Clinical PracticeIsabellaRuthNo ratings yet
- Emerging Infectious Disease Agents and Their Potential Threat To Transfusion Safety.Document29 pagesEmerging Infectious Disease Agents and Their Potential Threat To Transfusion Safety.Pritha BhuwapaksophonNo ratings yet
- Bo Kazha NovaDocument8 pagesBo Kazha NovaYudha Baskara ArdhaputraNo ratings yet
- Coronavirus Uncovered: What You Need to Know to Be ProtectedFrom EverandCoronavirus Uncovered: What You Need to Know to Be ProtectedNo ratings yet
- EeeeDocument2 pagesEeeegugicevdzoceNo ratings yet
- Psychiatry of Pandemics: A Mental Health Response to Infection OutbreakFrom EverandPsychiatry of Pandemics: A Mental Health Response to Infection OutbreakDamir HuremovićNo ratings yet
- Mycology-Virology: Reflection Paper JournalDocument6 pagesMycology-Virology: Reflection Paper JournaljeffdelacruzNo ratings yet
- Paper 1 de Discusión Semana 2Document13 pagesPaper 1 de Discusión Semana 2Jairo GuachamínNo ratings yet
- Movie Review by Fahim AhmedDocument11 pagesMovie Review by Fahim AhmedMasud KhanNo ratings yet
- International Journal of Infectious Diseases: James Pellerin, Michael B. EdmondDocument4 pagesInternational Journal of Infectious Diseases: James Pellerin, Michael B. EdmondTea LeafNo ratings yet
- Sexually Transmitted DiseasesDocument9 pagesSexually Transmitted DiseasesOdane LawrenceNo ratings yet
- Sexually Transmitted Diseases Autosaved - Docx 22222Document5 pagesSexually Transmitted Diseases Autosaved - Docx 22222Badang Casio JoeyNo ratings yet
- SyphilisDocument115 pagesSyphilisabel semuNo ratings yet
- The Most Important Lessons Learned: Late-Stage PandemicDocument9 pagesThe Most Important Lessons Learned: Late-Stage PandemicAnita DewiNo ratings yet
- Epidemiology at Barcelona: The Headline You Won't Read - Oral Sex Really Is Low RiskDocument9 pagesEpidemiology at Barcelona: The Headline You Won't Read - Oral Sex Really Is Low RiskcarolelisNo ratings yet
- Herpes Fact SheetDocument2 pagesHerpes Fact SheetRebecca RichardsonNo ratings yet
- Insurge Intelligence Support UsDocument22 pagesInsurge Intelligence Support UsCarolina TitoNo ratings yet
- Dr. Sole's STD LectureDocument76 pagesDr. Sole's STD Lecturef3er3No ratings yet
- A Primer On Monkeypox Virus For.7Document7 pagesA Primer On Monkeypox Virus For.7OMARNo ratings yet
- AIDS and Sexual Morality - What Is The Connection - Issue 4 - Philosophy NowDocument5 pagesAIDS and Sexual Morality - What Is The Connection - Issue 4 - Philosophy NowKomkor GuyNo ratings yet
- Running Head: Herpes Simplex Virus 1Document9 pagesRunning Head: Herpes Simplex Virus 1AnneElizabethNo ratings yet
- 119 FullDocument14 pages119 FullClarestaNo ratings yet
- Honors 221 Term Paper 1Document5 pagesHonors 221 Term Paper 1api-725270319No ratings yet
- Herpes Virus Association Press Release (RV Golding) 2014Document2 pagesHerpes Virus Association Press Release (RV Golding) 2014HIV Justice NetworkNo ratings yet
- Herpes SimplexDocument12 pagesHerpes SimplexRay MaudyNo ratings yet
- Estrés y Riesgo de IctusDocument12 pagesEstrés y Riesgo de IctusAndrés SantanaNo ratings yet
- Genital Herpes and Its Management: Clinical ReviewDocument5 pagesGenital Herpes and Its Management: Clinical ReviewBayu Surya DanaNo ratings yet
- 1101 AIDS&SelenoEnzymes1Document5 pages1101 AIDS&SelenoEnzymes1JOSH USHERNo ratings yet
- Definition of AIDSDocument6 pagesDefinition of AIDSromeo riveraNo ratings yet
- Caso 43 - Artigo 2 - Clinical Management of Herpes Simplex Virus InfectionsDocument9 pagesCaso 43 - Artigo 2 - Clinical Management of Herpes Simplex Virus InfectionsBernardo ZuccoNo ratings yet
- Dengue (Lancet)Document16 pagesDengue (Lancet)Roberth Mero100% (1)
- Sexually Transmitted DiseasesDocument64 pagesSexually Transmitted DiseasesClinton BradleyNo ratings yet
- Montesinos 1990Document10 pagesMontesinos 1990Samuel AraújoNo ratings yet
- Herpes JurnalDocument6 pagesHerpes Jurnalags.suryono102No ratings yet
- Biological and Chemical Hazards of Forensic Skeletal AnalysisDocument9 pagesBiological and Chemical Hazards of Forensic Skeletal AnalysisOskar GomezNo ratings yet
- Types of Sexually Transmitted InfectionsDocument4 pagesTypes of Sexually Transmitted InfectionsWarren ConsultaNo ratings yet
- HIV in ColoradoDocument54 pagesHIV in ColoradorichardslsuNo ratings yet
- 2019 Viral, Bacterial, and Fungal Infections of The Oral Mucosa Types, Incidence, Predisposing Factors, Diagnostic Algorithms, and ManagementDocument29 pages2019 Viral, Bacterial, and Fungal Infections of The Oral Mucosa Types, Incidence, Predisposing Factors, Diagnostic Algorithms, and ManagementalyssaNo ratings yet
- Jurnal 14Document3 pagesJurnal 14Putri Intan SolehahNo ratings yet
- Text Book of Microbiology (221-330)Document110 pagesText Book of Microbiology (221-330)Jamila ridaNo ratings yet
- Library Research in ImmunologyDocument22 pagesLibrary Research in ImmunologyCimini, Le MauriceNo ratings yet
- Monkey Pox Fact SheetDocument3 pagesMonkey Pox Fact SheetMalcolm M. LeeNo ratings yet
- Stop-Holocaust EMADocument3 pagesStop-Holocaust EMAwebtrekker UKNo ratings yet
- Aspectos Biológicos, Terapeuticos en Mujeres Con VIH Comparado A Hombres AIDS ReviewDocument8 pagesAspectos Biológicos, Terapeuticos en Mujeres Con VIH Comparado A Hombres AIDS ReviewIsmaelJoséGonzálezGuzmánNo ratings yet
- AIDS Is Not InfectiousDocument18 pagesAIDS Is Not Infectiousbadboy6.868510No ratings yet
- ContagionDocument9 pagesContagionMasud KhanNo ratings yet
- Who Risk Assessment Human Infections With Influenza A (H7N9) Virus 13 April 2013Document3 pagesWho Risk Assessment Human Infections With Influenza A (H7N9) Virus 13 April 2013kbl27No ratings yet
- COVID Is The-Virus-That-Does-Not-ExistDocument41 pagesCOVID Is The-Virus-That-Does-Not-ExistHansley Templeton Cook100% (2)
- Stds and Hiv Fact Sheet PressDocument2 pagesStds and Hiv Fact Sheet Pressapi-261528774No ratings yet
- 11,12,13Document14 pages11,12,13Hedya Nadhrati SururaNo ratings yet
- Nej MCP 2108502Document9 pagesNej MCP 2108502Marialejandra GuevaraNo ratings yet
- J9 How Little We Know Herpes ZosterDocument4 pagesJ9 How Little We Know Herpes ZosterNur Adha AtjoNo ratings yet
- Condom Eff TimeDocument6 pagesCondom Eff TimeDavid SantosNo ratings yet
- Nejmcp 2108502Document9 pagesNejmcp 2108502Manuel GilNo ratings yet
- The Cruel Hoax Called Herpes GenetalisDocument48 pagesThe Cruel Hoax Called Herpes GenetalisPeter M. Randall0% (1)
- Health 8: Issues and Problems Related To Human SexualityDocument14 pagesHealth 8: Issues and Problems Related To Human SexualityAizel Mae Consas /Amado HernandezNo ratings yet
- Reflection Paper #3Document2 pagesReflection Paper #3Marc Jalen ReladorNo ratings yet
- MSDS PC DURON 15W40 - Ingles PDFDocument6 pagesMSDS PC DURON 15W40 - Ingles PDFaliosk8799No ratings yet
- Noro Virus - Analytical MicrobiologyDocument12 pagesNoro Virus - Analytical Microbiologykolita kamal100% (1)
- M103 BioethicsDocument37 pagesM103 BioethicsQuerubin DandoyNo ratings yet
- Baremos Sexual Desire Inventory MEN WomenDocument1 pageBaremos Sexual Desire Inventory MEN WomenGabriNo ratings yet
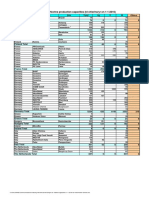
- Installed Chlorine Production Capacities (KT Chlorine/yr On 1-1-2016)Document2 pagesInstalled Chlorine Production Capacities (KT Chlorine/yr On 1-1-2016)keo landNo ratings yet
- Paint Specification - Package ADocument53 pagesPaint Specification - Package AMohammedNo ratings yet
- Funda Practice QuestionsDocument2 pagesFunda Practice QuestionsMikaella CondeNo ratings yet
- WDR22 Booklet 1Document74 pagesWDR22 Booklet 1Khánh Hoàng NamNo ratings yet
- Autism Spectrum DisorderDocument7 pagesAutism Spectrum DisorderAbhishek GuptaNo ratings yet
- Critique PaperDocument2 pagesCritique PaperDaisy Mae GujolNo ratings yet
- PhysicsinOrthodontics04 17 21SLJMRDocument43 pagesPhysicsinOrthodontics04 17 21SLJMRYaser JasNo ratings yet
- Virtue EthicsDocument76 pagesVirtue EthicsMusfira Zubair100% (3)
- Hourglass Sculpt: With Lilly SabriDocument6 pagesHourglass Sculpt: With Lilly SabriRukhsana ShahNo ratings yet
- Textbook of Physiotherapy in Surgical Conditions (PDF) (UniteBTTTdVRG)Document271 pagesTextbook of Physiotherapy in Surgical Conditions (PDF) (UniteBTTTdVRG)lejizix85% (27)
- Food DayDocument15 pagesFood DaydigdagNo ratings yet
- Cardiorespiratory SystemDocument19 pagesCardiorespiratory SystemEmanuel JheadNo ratings yet
- Master Thesis Product ManagementDocument7 pagesMaster Thesis Product Managementjjvveqvcf100% (2)
- Biochemical Mechanism of Vitamin A in VisionDocument3 pagesBiochemical Mechanism of Vitamin A in VisionAurelia HernandezNo ratings yet
- 2NF - Grand Case Presentation Written OutputDocument99 pages2NF - Grand Case Presentation Written OutputKyra Bianca R. FamacionNo ratings yet
- MD3 Peer TutoringDocument3 pagesMD3 Peer Tutoringdragtoss2No ratings yet
- Standardized Recipes Provides Many Benefits To School Food Service Operations. These Benefits IncludeDocument26 pagesStandardized Recipes Provides Many Benefits To School Food Service Operations. These Benefits IncludeJessel TorotoroNo ratings yet
- Goodwill Magazine For WebsiteDocument23 pagesGoodwill Magazine For WebsiteMARK ANTHONY ALCANTARANo ratings yet
- Kecemasan Ibu Hamil Tentang Pelayanan Antenatal Care Di Era Pandemi Covid-19Document6 pagesKecemasan Ibu Hamil Tentang Pelayanan Antenatal Care Di Era Pandemi Covid-19Nova RizkenNo ratings yet
- De Luyen Thi HSG 6Document5 pagesDe Luyen Thi HSG 6maiNo ratings yet
- MSC Counselling and PsychotherapyDocument71 pagesMSC Counselling and PsychotherapyGenesis TallyacademyNo ratings yet
- A Novel Krill Herd Based Random Forest Algorithm For Monitoring Patient HealthDocument19 pagesA Novel Krill Herd Based Random Forest Algorithm For Monitoring Patient Health胡浩No ratings yet
- Bitter Melon Bioactive Composition and Health Benefits A Review - Tan Et Al. 2015Document23 pagesBitter Melon Bioactive Composition and Health Benefits A Review - Tan Et Al. 2015Fatima HerreraNo ratings yet
- Technical Note 002 2009 Ggtps Submission of GMP ApplicationDocument3 pagesTechnical Note 002 2009 Ggtps Submission of GMP ApplicationElaine NascimentoNo ratings yet
- PRICE LIST Kalbe (Enseval)Document7 pagesPRICE LIST Kalbe (Enseval)YogaMurtiNo ratings yet
- Educational Researcher: An Educational Psychology Success Story: Social Interdependence Theory and Cooperative LearningDocument16 pagesEducational Researcher: An Educational Psychology Success Story: Social Interdependence Theory and Cooperative LearningdhenagrNo ratings yet
- The Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeFrom EverandThe Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeRating: 4.5 out of 5 stars4.5/5 (140)
- Summary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDFrom EverandSummary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDRating: 4.5 out of 5 stars4.5/5 (167)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- Rewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryFrom EverandRewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryRating: 4.5 out of 5 stars4.5/5 (157)
- Somatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionFrom EverandSomatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionNo ratings yet
- My Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesFrom EverandMy Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesRating: 5 out of 5 stars5/5 (70)
- An Autobiography of Trauma: A Healing JourneyFrom EverandAn Autobiography of Trauma: A Healing JourneyRating: 5 out of 5 stars5/5 (2)
- Don't Panic: Taking Control of Anxiety AttacksFrom EverandDon't Panic: Taking Control of Anxiety AttacksRating: 4 out of 5 stars4/5 (12)
- The Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeFrom EverandThe Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeRating: 4.5 out of 5 stars4.5/5 (49)
- Heal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaFrom EverandHeal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaRating: 4.5 out of 5 stars4.5/5 (56)
- How to Be Miserable: 40 Strategies You Already UseFrom EverandHow to Be Miserable: 40 Strategies You Already UseRating: 4.5 out of 5 stars4.5/5 (57)
- Rapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreFrom EverandRapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreRating: 5 out of 5 stars5/5 (17)
- Summary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisFrom EverandSummary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (5)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (39)
- The Worry Trick: How Your Brain Tricks You into Expecting the Worst and What You Can Do About ItFrom EverandThe Worry Trick: How Your Brain Tricks You into Expecting the Worst and What You Can Do About ItRating: 4.5 out of 5 stars4.5/5 (107)
- Brain Inflamed: Uncovering the Hidden Causes of Anxiety, Depression, and Other Mood Disorders in Adolescents and TeensFrom EverandBrain Inflamed: Uncovering the Hidden Causes of Anxiety, Depression, and Other Mood Disorders in Adolescents and TeensRating: 5 out of 5 stars5/5 (2)
- Redefining Anxiety: What It Is, What It Isn't, and How to Get Your Life BackFrom EverandRedefining Anxiety: What It Is, What It Isn't, and How to Get Your Life BackRating: 4.5 out of 5 stars4.5/5 (152)
- BORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONFrom EverandBORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONRating: 4.5 out of 5 stars4.5/5 (24)
- The Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouFrom EverandThe Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouNo ratings yet
- Winning the War in Your Mind: Change Your Thinking, Change Your LifeFrom EverandWinning the War in Your Mind: Change Your Thinking, Change Your LifeRating: 5 out of 5 stars5/5 (559)
- A Profession Without Reason: The Crisis of Contemporary Psychiatry—Untangled and Solved by Spinoza, Freethinking, and Radical EnlightenmentFrom EverandA Profession Without Reason: The Crisis of Contemporary Psychiatry—Untangled and Solved by Spinoza, Freethinking, and Radical EnlightenmentNo ratings yet
- I Don't Want to Talk About It: Overcoming the Secret Legacy of Male DepressionFrom EverandI Don't Want to Talk About It: Overcoming the Secret Legacy of Male DepressionRating: 4.5 out of 5 stars4.5/5 (106)
- Binaural Beats: Activation of pineal gland – Stress reduction – Meditation – Brainwave entrainment – Deep relaxationFrom EverandBinaural Beats: Activation of pineal gland – Stress reduction – Meditation – Brainwave entrainment – Deep relaxationRating: 5 out of 5 stars5/5 (9)
- Anxious for Nothing: Finding Calm in a Chaotic WorldFrom EverandAnxious for Nothing: Finding Calm in a Chaotic WorldRating: 4.5 out of 5 stars4.5/5 (1245)