You might also like
- Free Payroll Book PDFDocument27 pagesFree Payroll Book PDFGspr BoJoyNo ratings yet
- Blue Shield of California Shield Savings Plans A36813 2011Document2 pagesBlue Shield of California Shield Savings Plans A36813 2011DennisNo ratings yet
- Recruiting in JapanDocument29 pagesRecruiting in JapanRam100% (1)
- Private and Confidential: Application For Employment FormDocument4 pagesPrivate and Confidential: Application For Employment FormAlezec WangNo ratings yet
- Employee Engagement & Retention - Keeping The Right People - HR Toolkit - HrcouncilDocument6 pagesEmployee Engagement & Retention - Keeping The Right People - HR Toolkit - HrcouncilPayel Sinha Chowdhury DasNo ratings yet
- EMPLOYEE Recruitment and SelectionDocument9 pagesEMPLOYEE Recruitment and Selectionjaydee_atc5814No ratings yet
- Money Saving Tips - A White Paper: Techniques I've Actually Used: Thinking About Money, #2From EverandMoney Saving Tips - A White Paper: Techniques I've Actually Used: Thinking About Money, #2No ratings yet
- 38 - Nisda vs. Sea ServeDocument2 pages38 - Nisda vs. Sea ServeMigel DemdamNo ratings yet
- Department of TamilDocument404 pagesDepartment of TamilSaravanan Muniandi100% (1)
- Photon Benefits 2022 (August)Document7 pagesPhoton Benefits 2022 (August)sojithesouljaNo ratings yet
- 2023 FMCNA Medical Plan Cost ComparisonDocument2 pages2023 FMCNA Medical Plan Cost ComparisonCristal PeoplesNo ratings yet
- 2021 BAAG - Technologies - TalentDocument2 pages2021 BAAG - Technologies - TalentDalt RaNo ratings yet
- Blueoptimum Plus Ppo Plan: Benefit SummaryDocument4 pagesBlueoptimum Plus Ppo Plan: Benefit Summarylooksmart111No ratings yet
- Aetna 2014Document1 pageAetna 2014Vignesh EswaranNo ratings yet
- 2 VEBA Plan ComparisonDocument2 pages2 VEBA Plan ComparisonMitchell BigleyNo ratings yet
- Complete Employee Benefits Guide TemplateDocument38 pagesComplete Employee Benefits Guide TemplateAriyanta DanyNo ratings yet
- 2023 Open Enrollment Benefit Presenation - 11142022Document30 pages2023 Open Enrollment Benefit Presenation - 11142022margreen5No ratings yet
- Jo Say 2020 QuotesDocument6 pagesJo Say 2020 QuotessebastianNo ratings yet
- 2021 THNM Individual Health PlansDocument1 page2021 THNM Individual Health PlansSara SnowNo ratings yet
- Pick A Health Plan - HealthCare - GovDocument9 pagesPick A Health Plan - HealthCare - GovBruce henschelNo ratings yet
- BCBS Enrollment GuideDocument6 pagesBCBS Enrollment GuideAnonymous Lri40PrlkNo ratings yet
- USS Pre-Medicare PPO With RX PlanDocument3 pagesUSS Pre-Medicare PPO With RX PlanAnonymous w0egAgMouGNo ratings yet
- 2017 Employee Benefit Highlights - Support StaffDocument8 pages2017 Employee Benefit Highlights - Support StaffJohn AcardoNo ratings yet
- 2022 Steven Charles BAG - CODocument4 pages2022 Steven Charles BAG - COAlejuanchis Kamacho GarciaNo ratings yet
- Us Apple Plus Ppo Feb2019 en 1Document3 pagesUs Apple Plus Ppo Feb2019 en 1Lucas Coleta AlmeidaNo ratings yet
- Book1 (Version 1)Document1 pageBook1 (Version 1)agulabNo ratings yet
- Aetna Open Choice Ppo: Plan DetailsDocument2 pagesAetna Open Choice Ppo: Plan DetailsSnake Diet RyanNo ratings yet
- Plan ComparisonDocument2 pagesPlan ComparisonSahil JindalNo ratings yet
- Blue Cross Select BronzeDocument6 pagesBlue Cross Select Bronzeapi-285960909No ratings yet
- Benefit Highlights: AARP Medicare Advantage Choice (PPO)Document3 pagesBenefit Highlights: AARP Medicare Advantage Choice (PPO)EstherNo ratings yet
- What You Pay in The PPO PlanDocument2 pagesWhat You Pay in The PPO Plannathan wongNo ratings yet
- FY 2022-2023 Instruction Partners Benefits OverviewDocument16 pagesFY 2022-2023 Instruction Partners Benefits OverviewSendhil RevuluriNo ratings yet
- Thomas PPO Thomas HMO Claire EPO Claire HMO: in Network. in NetworkDocument1 pageThomas PPO Thomas HMO Claire EPO Claire HMO: in Network. in Networkanas fassiNo ratings yet
- 2023 Talent BAAGDocument3 pages2023 Talent BAAGThi HanNo ratings yet
- Benefits Overview 2018Document5 pagesBenefits Overview 2018Joby JoNo ratings yet
- LTIM - USA Employees Benefits Overview - 2024Document20 pagesLTIM - USA Employees Benefits Overview - 2024Ramesh Kumar KNo ratings yet
- KP - Plan Summary Medical - PPODocument3 pagesKP - Plan Summary Medical - PPOshanegbaker51No ratings yet
- Medical Insurance: January 1, 2023 - December 31, 2023Document4 pagesMedical Insurance: January 1, 2023 - December 31, 2023Andrés BaqueroNo ratings yet
- Summary of 2022 Benefit Changes: MedicalDocument5 pagesSummary of 2022 Benefit Changes: MedicalChinnu SalimathNo ratings yet
- M2A1 US Census Data SearchDocument6 pagesM2A1 US Census Data SearchragcajunNo ratings yet
- Plan ComparisonDocument4 pagesPlan Comparisontth79hj4dvNo ratings yet
- UserDocument5 pagesUserAldieno PribadiNo ratings yet
- Anthem® Blue Cross Your Plan: Snap, Inc: Custom Classic PPO 500/20/20 Your Network: Prudent Buyer PPODocument9 pagesAnthem® Blue Cross Your Plan: Snap, Inc: Custom Classic PPO 500/20/20 Your Network: Prudent Buyer PPOSamson FungNo ratings yet
- TransPhos MedicalDocument3 pagesTransPhos Medicalres6250No ratings yet
- Isoa Hea OMPASS - 2016 - 2017 PDFDocument13 pagesIsoa Hea OMPASS - 2016 - 2017 PDFSharif M Mizanur RahmanNo ratings yet
- 2010 UnitedHealthcare Benefits SummaryDocument1 page2010 UnitedHealthcare Benefits Summaryapi-27017317No ratings yet
- Kaiser Permanente Compare Plans CA 2011 KPIFDocument1 pageKaiser Permanente Compare Plans CA 2011 KPIFDennis AlexanderNo ratings yet
- Medical Comparison Chart 2020Document3 pagesMedical Comparison Chart 2020hollingermikeNo ratings yet
- 2020 Ankura Benefits GuideDocument20 pages2020 Ankura Benefits GuidegpperkNo ratings yet
- Schedule of BenefitsDocument7 pagesSchedule of BenefitsMaddy CruzNo ratings yet
- 76962CT0010006-01 en USDocument98 pages76962CT0010006-01 en USKathy ApergisNo ratings yet
- Employee Benefits-Wellness Guide 2023-24Document30 pagesEmployee Benefits-Wellness Guide 2023-24shanzeh2609No ratings yet
- WWW - Healthcare.gov/sbc-Glossary: Important Questions Answers Why This MattersDocument10 pagesWWW - Healthcare.gov/sbc-Glossary: Important Questions Answers Why This MattersRohitKumarNo ratings yet
- Blue-Cross-Premier-Platinum-Extra-Dental-Vision CareerDocument8 pagesBlue-Cross-Premier-Platinum-Extra-Dental-Vision Careerapi-248930594No ratings yet
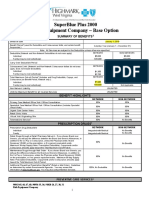
- Rish Equipment Base Plan Option Eff. 1.1.2019Document4 pagesRish Equipment Base Plan Option Eff. 1.1.2019michala anthonyNo ratings yet
- Blue Shield of California Shield Savings Plans IFP 1-2011Document2 pagesBlue Shield of California Shield Savings Plans IFP 1-2011Dennis AlexanderNo ratings yet
- 02 28 2019Document4 pages02 28 2019Deep khatkarNo ratings yet
- Kaiser Permanente: Good Health Is No SecretDocument6 pagesKaiser Permanente: Good Health Is No SecretThomas Dominic CazneauNo ratings yet
- Public Employees' Benefit Board: Plan Design Options: UpdatedDocument4 pagesPublic Employees' Benefit Board: Plan Design Options: UpdatedStatesman JournalNo ratings yet
- 2017 Anthem GHIP Benefits Booklet (Final)Document119 pages2017 Anthem GHIP Benefits Booklet (Final)Alexander NewberryNo ratings yet
- 2017 Anthem GHIP Benefits Booklet (Final)Document119 pages2017 Anthem GHIP Benefits Booklet (Final)Alexander NewberryNo ratings yet
- I A Bluechoice Ppo - Large Group (51+ Employees) Plan 4511Sx Benefit SummaryDocument3 pagesI A Bluechoice Ppo - Large Group (51+ Employees) Plan 4511Sx Benefit SummaryDave EmersonNo ratings yet
- Trinity Health 020 Traditional Ppo Plan 10202021Document10 pagesTrinity Health 020 Traditional Ppo Plan 10202021emily WNo ratings yet
- International Student Health Certificate Individual CoverageDocument40 pagesInternational Student Health Certificate Individual CoverageJialun ZhuNo ratings yet
- HSA Choice Plus Plan AIQM/02V: Important Questions Answers Why This MattersDocument8 pagesHSA Choice Plus Plan AIQM/02V: Important Questions Answers Why This MattersAnonymous PWVeGM5n9gNo ratings yet
- Kaiser Permanente: KP CA Silver 2000/45: This Is Only A SummaryDocument8 pagesKaiser Permanente: KP CA Silver 2000/45: This Is Only A SummaryKelly HoffmanNo ratings yet
- 2024 Salaried ICSDocument4 pages2024 Salaried ICSSaravanan MuniandiNo ratings yet
- 401k Separation From Service FormDocument9 pages401k Separation From Service FormSaravanan MuniandiNo ratings yet
- PG Scholar, Lecturer, HOD, Department of Maruthuvam,: Biography of Siddhars R.N.Hema, H.Nalini Sofia, S.MohanDocument7 pagesPG Scholar, Lecturer, HOD, Department of Maruthuvam,: Biography of Siddhars R.N.Hema, H.Nalini Sofia, S.MohanSaravanan MuniandiNo ratings yet
- Gratitude Journal Printable With PromptsDocument2 pagesGratitude Journal Printable With PromptsSaravanan MuniandiNo ratings yet
- TVA BOK 0018936 Encyclopaedia of Tamil LiteratureDocument694 pagesTVA BOK 0018936 Encyclopaedia of Tamil LiteratureSaravanan MuniandiNo ratings yet
- MicroDocument1 pageMicroSaravanan MuniandiNo ratings yet
- Coronavirus Economic Depression Survival PDFDocument42 pagesCoronavirus Economic Depression Survival PDFSaravanan MuniandiNo ratings yet
- QA Analyst - Automation TestingDocument1 pageQA Analyst - Automation TestingSaravanan MuniandiNo ratings yet
- SystemDocument1 pageSystemSaravanan MuniandiNo ratings yet
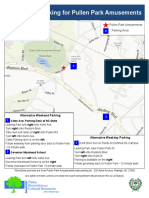
- Alternative Parking For Pullen Park AmusementsDocument1 pageAlternative Parking For Pullen Park AmusementsSaravanan MuniandiNo ratings yet
- Delivery Manager: The Main Responsibilities of The Post AreDocument4 pagesDelivery Manager: The Main Responsibilities of The Post AreSaravanan MuniandiNo ratings yet
- Factors Affecting StaffingDocument1 pageFactors Affecting Staffingbabbusinghmann007No ratings yet
- 1978 Mowday, Steers, L.W. PorterThe Measurement of Organizational CommitmentDocument58 pages1978 Mowday, Steers, L.W. PorterThe Measurement of Organizational CommitmentÁtila de AssisNo ratings yet
- Professional EthicsDocument11 pagesProfessional EthicsConnie LopicoNo ratings yet
- Baylor ComplaintDocument22 pagesBaylor ComplaintDeadspinNo ratings yet
- Osha NotesDocument4 pagesOsha NotesYee JingyeNo ratings yet
- Written HW4Document14 pagesWritten HW4aplesgjskNo ratings yet
- Psea - 19 Advance Payment For Maternity BenefitDocument1 pagePsea - 19 Advance Payment For Maternity BenefitForemost HRNo ratings yet
- Letter On Staff Welfare MeasuresDocument2 pagesLetter On Staff Welfare Measuresdsk4678No ratings yet
- Element 3 Case Study: Change in Organizational Culture at JaguarDocument3 pagesElement 3 Case Study: Change in Organizational Culture at JaguarRohaan a.k.a HoneyNo ratings yet
- The HR Scorecard AND The Balanced Scorecard: Presented By: MAYURI DAS (10BSP1061)Document21 pagesThe HR Scorecard AND The Balanced Scorecard: Presented By: MAYURI DAS (10BSP1061)Mayuri DasNo ratings yet
- ASM2 EV THẦY DŨNGDocument7 pagesASM2 EV THẦY DŨNGNguyễn Thành Nam 12C4 25.No ratings yet
- Domestic Contract 2024Document5 pagesDomestic Contract 2024vicky.sharon2No ratings yet
- Qa7-Assessment and Training Staff Registration FormDocument3 pagesQa7-Assessment and Training Staff Registration FormDang Minh HuongNo ratings yet
- Unitop PayrollDocument2 pagesUnitop Payrolldelacruzstevewyatt0208No ratings yet
- Federal Civil Servants ProclamationDocument35 pagesFederal Civil Servants ProclamationephremNo ratings yet
- Effect of Glob On WomenDocument36 pagesEffect of Glob On WomenRahul JeshnaniNo ratings yet
- Business Operations AND ImplementationDocument45 pagesBusiness Operations AND ImplementationDar LynnNo ratings yet
- Group 1 Chapters 1 3Document11 pagesGroup 1 Chapters 1 3Julius Miguel SarmientoNo ratings yet
- Mayor Annise Parker Inaugural Address January 3, 2012: I Love This City!Document4 pagesMayor Annise Parker Inaugural Address January 3, 2012: I Love This City!Houston ChronicleNo ratings yet
- Socio-Economic Status of Daily Wage Earners in Cuddalore TownDocument8 pagesSocio-Economic Status of Daily Wage Earners in Cuddalore TownarcherselevatorsNo ratings yet
- Clare BerminghamDocument93 pagesClare BerminghamBryan Ken TanNo ratings yet
- Labour Law Cheat SheetDocument34 pagesLabour Law Cheat SheetAnjana P NairNo ratings yet
- HR Guide Xto10x 4b781550b0Document35 pagesHR Guide Xto10x 4b781550b0Yatharth SahooNo ratings yet
- Family Particular FormDocument2 pagesFamily Particular FormYin ChuangNo ratings yet