You might also like
- Littelfuse EVI EV Charging Infrastructure Presentation PDFDocument19 pagesLittelfuse EVI EV Charging Infrastructure Presentation PDFRaka Pratindy100% (1)
- AMORC What Constitutes A High Degree Member in AMORC 2Document3 pagesAMORC What Constitutes A High Degree Member in AMORC 2Francis EjikeNo ratings yet
- Ayurvedam For Hair Related IssuesDocument14 pagesAyurvedam For Hair Related IssuesGangadhar Yerraguntla100% (1)
- Brewers Pallette PosterDocument1 pageBrewers Pallette PosterAnonymous hP6ab2D1ppNo ratings yet
- DR As TuberculosisDocument59 pagesDR As TuberculosisAchhar SinghNo ratings yet
- CardiomyopathyDocument1 pageCardiomyopathyTrisha VergaraNo ratings yet
- Basic SCBA: Self-Contained Breathing ApparatusDocument51 pagesBasic SCBA: Self-Contained Breathing ApparatusPaoloFregonaraNo ratings yet
- Grade 7-Advanced Science Environmental ScienceDocument8 pagesGrade 7-Advanced Science Environmental ScienceChrisel Luat LopezNo ratings yet
- Tuberculosis OrginalDocument11 pagesTuberculosis Orginalthanuja mathew100% (1)
- The Word Became Flesh An Exploratory Essay On Jesu 003Document62 pagesThe Word Became Flesh An Exploratory Essay On Jesu 003Alexios VrionisNo ratings yet
- Modified Atmosphere Packaging AssignmentDocument22 pagesModified Atmosphere Packaging AssignmentSanjhai PrakashNo ratings yet
- TB Case HistoryDocument4 pagesTB Case HistoryMarisa PetersonNo ratings yet
- Pulmonary TuberculosisDocument99 pagesPulmonary Tuberculosis'Emilya'No ratings yet
- Current Medical Management of Pulmonary TuberculosisDocument9 pagesCurrent Medical Management of Pulmonary TuberculosisFaradilla FirdausaNo ratings yet
- Case Study Group 4 - XI IPADocument15 pagesCase Study Group 4 - XI IPAkeisya angNo ratings yet
- Emergency MedDocument4 pagesEmergency MedbencleeseNo ratings yet
- TuberculosisDocument76 pagesTuberculosissashmita rautNo ratings yet
- Essential Update: FDA Approves Rifapentine For Latent TB InfectionDocument16 pagesEssential Update: FDA Approves Rifapentine For Latent TB InfectionAdriyan SikumalayNo ratings yet
- Bio Project Magazine About The Respiratory SystemDocument26 pagesBio Project Magazine About The Respiratory Systemamr.hazem311No ratings yet
- Types of TuberculosisDocument7 pagesTypes of TuberculosisYashaswi ANo ratings yet
- Tuberculosis - Disease Management - CompDocument17 pagesTuberculosis - Disease Management - CompAhsan kamalNo ratings yet
- Clinical Manifestations and Complications of Pulmonary Tuberculosis - UpToDateDocument20 pagesClinical Manifestations and Complications of Pulmonary Tuberculosis - UpToDatedixama9519No ratings yet
- 4 MMMMMMMDocument5 pages4 MMMMMMMSatriaAuliansyahNo ratings yet
- Tuberculosis: BackgroundDocument25 pagesTuberculosis: BackgroundLuis Alberto Basurto RomeroNo ratings yet
- Up To Date. Tuberculosis Clinical Manifestations and ComplicationsDocument41 pagesUp To Date. Tuberculosis Clinical Manifestations and ComplicationsGuardito PequeñoNo ratings yet
- Tuberculosis Unit 1 Lecture - 1Document39 pagesTuberculosis Unit 1 Lecture - 1Kubra Rasool100% (1)
- Tuberculosis. Like The Common Cold, It Spreads Through The Air. People WhoDocument16 pagesTuberculosis. Like The Common Cold, It Spreads Through The Air. People WhoNESPA LIZMANo ratings yet
- Mse) !) P (8x9e. h4, DDocument15 pagesMse) !) P (8x9e. h4, DKristel AnneNo ratings yet
- The LungsDocument9 pagesThe Lungsyogi pramanaNo ratings yet
- Search Termsearch Database: A Cherian SV ThomasDocument16 pagesSearch Termsearch Database: A Cherian SV ThomasHayelom Michael100% (1)
- Tuberculosis: Presentation by Roll Number 45Document29 pagesTuberculosis: Presentation by Roll Number 45You FoolNo ratings yet
- Clinical Manifestations and Evaluation of Pulmonary TuberculosisDocument30 pagesClinical Manifestations and Evaluation of Pulmonary TuberculosisSaid Plazola MercadoNo ratings yet
- Tuberculosis: (For July 2014 Intake)Document60 pagesTuberculosis: (For July 2014 Intake)PETER STEPHEN BANDANo ratings yet
- Extrapulmonary Tuberculosis: Key PointsDocument6 pagesExtrapulmonary Tuberculosis: Key PointsRetno ManggalihNo ratings yet
- TUGAS Visite HarianDocument13 pagesTUGAS Visite HarianYosuairvanNo ratings yet
- Jurnal Bahasa InggrisDocument12 pagesJurnal Bahasa InggrisVanessa Angelica SitepuNo ratings yet
- T Tuberculosis-230127-125842Document36 pagesT Tuberculosis-230127-125842Leong Sze XieNo ratings yet
- Nursing Care Management 103 Cap MRDocument9 pagesNursing Care Management 103 Cap MRkarenfaye00No ratings yet
- 3 PneumoniaDocument17 pages3 PneumoniaMohamed Na3eemNo ratings yet
- Tuberculosis: DR .. Magdi Elbaloola Ahmed Physcian & GastrohepatologistDocument59 pagesTuberculosis: DR .. Magdi Elbaloola Ahmed Physcian & GastrohepatologistÅbübâkêř Äbd-ëřhēēm BãřřîNo ratings yet
- Respiratory Problems in PregnancyDocument16 pagesRespiratory Problems in PregnancyYvette Carmelle Barroma GellangNo ratings yet
- Pulmonary TuberculosisDocument32 pagesPulmonary Tuberculosissara M.H.No ratings yet
- English in Nursing Science Assignment Name: Devi SetiawanDocument12 pagesEnglish in Nursing Science Assignment Name: Devi SetiawanDevi SetiawanNo ratings yet
- Universidad Nacional de TrujilloDocument13 pagesUniversidad Nacional de TrujilloWendy Santos MonteroNo ratings yet
- Assignment: - TuberculosisDocument9 pagesAssignment: - TuberculosisAakash SahaNo ratings yet
- Tuberculosis & Leprosy: Alkan Health Science Business and Technology CollegeDocument59 pagesTuberculosis & Leprosy: Alkan Health Science Business and Technology CollegejibrailNo ratings yet
- Infectious Tuberculosis-18 (Muhadharaty)Document11 pagesInfectious Tuberculosis-18 (Muhadharaty)dr.salam.hassaniNo ratings yet
- Pneumonia: Related Diagnostic TestsDocument2 pagesPneumonia: Related Diagnostic TestsBenj VillanuevaNo ratings yet
- Chapter 1Document30 pagesChapter 1Ayro Business CenterNo ratings yet
- TuberculosisDocument4 pagesTuberculosisDr Mangesti Utami PKM Kebaman BanyuwangiNo ratings yet
- RESPI (PBL2) - Mohamad Arbian Karim - FMUI20Document8 pagesRESPI (PBL2) - Mohamad Arbian Karim - FMUI20Mohamad Arbian KarimNo ratings yet
- Houston2014Document5 pagesHouston2014Retno ManggalihNo ratings yet
- Referat TBDocument16 pagesReferat TBRobert ChristevenNo ratings yet
- Microbiolspec - TNMI7 0032 2016Document13 pagesMicrobiolspec - TNMI7 0032 2016Dhea Dwi AnandaNo ratings yet
- Tuberculosis in ChildrenDocument80 pagesTuberculosis in ChildrenEslam HamadaNo ratings yet
- Assignment 1Document10 pagesAssignment 1Ilhaashini krishnanNo ratings yet
- Cap HR With PTBDocument6 pagesCap HR With PTBReese Alessandra GandulfoNo ratings yet
- CompilationDocument24 pagesCompilationKath RubioNo ratings yet
- Tuberculosis: DR.D D Mishra AGM, Medical ServicesDocument31 pagesTuberculosis: DR.D D Mishra AGM, Medical ServicesSHUBHAMNo ratings yet
- Tuberculosis in HaitiDocument8 pagesTuberculosis in HaitianthonykarabanowNo ratings yet
- Pulmonary TuberculosisDocument2 pagesPulmonary Tuberculosismgamboa_10No ratings yet
- Literature Review 3 TopicDocument27 pagesLiterature Review 3 TopicBharathi Sneha PeriasamyNo ratings yet
- Tuberculous Meningitis: Challenges in Diagnosis and ManagementDocument7 pagesTuberculous Meningitis: Challenges in Diagnosis and ManagementNursyahidah IdrisNo ratings yet
- Jnma00736 0021Document3 pagesJnma00736 0021talenticaxo1No ratings yet
- Pulmonary Tuberculosis: Muhammad Omar Warsame Adam Elmi AdamDocument20 pagesPulmonary Tuberculosis: Muhammad Omar Warsame Adam Elmi AdamMuhammad075No ratings yet
- 08 Pneumonia Review ofDocument4 pages08 Pneumonia Review ofMonika Margareta Maria ElviraNo ratings yet
- Chapter-46 - Tuberculosis of Kidney and Urinary TractDocument12 pagesChapter-46 - Tuberculosis of Kidney and Urinary TractmanaNo ratings yet
- TuberculosisDocument20 pagesTuberculosisBader AljarboaNo ratings yet
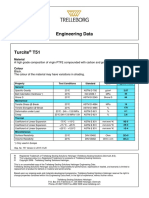
- Turcite T51 Engineering DataDocument1 pageTurcite T51 Engineering DataAntonio Rivera VillavicencioNo ratings yet
- Seajet 118 Ultra-Build Epoxy PrimerDocument2 pagesSeajet 118 Ultra-Build Epoxy PrimerRai Hasnain Ahmad DahaNo ratings yet
- RfI SB Listening ScriptsDocument18 pagesRfI SB Listening ScriptsKate PolissyaNo ratings yet
- Design and Fabrication of Single Cylinder Solenoid EngineDocument7 pagesDesign and Fabrication of Single Cylinder Solenoid EngineVIVA-TECH IJRINo ratings yet
- ISKRA Letak MC3xx 2016 Ver.4.0 2016.compressedDocument6 pagesISKRA Letak MC3xx 2016 Ver.4.0 2016.compressedmelanitisNo ratings yet
- Theoretical Foundations of Nursing - Review MaterialDocument10 pagesTheoretical Foundations of Nursing - Review MaterialKennethNo ratings yet
- AUSMAT Student Guide 2011Document16 pagesAUSMAT Student Guide 2011Sunway UniversityNo ratings yet
- Installation 3G Network ElementsDocument108 pagesInstallation 3G Network ElementsSDE RF WESTNo ratings yet
- Thin Film DepositionDocument34 pagesThin Film Depositionsenthil100% (2)
- Dr. M. Syed Jamil Asghar: Paper Published: 80Document6 pagesDr. M. Syed Jamil Asghar: Paper Published: 80Awaiz NoorNo ratings yet
- Indigenous Resources ActivitiesDocument17 pagesIndigenous Resources Activitiesscribbler49971100% (1)
- International StandardDocument8 pagesInternational Standardnazrul islamNo ratings yet
- Material Balance & Energy Balance - Reactor-2Document32 pagesMaterial Balance & Energy Balance - Reactor-2Xy karNo ratings yet
- Lecture5 (4) Mech of SolidsDocument18 pagesLecture5 (4) Mech of Solids'jhony' Fauzan NurdinNo ratings yet
- GFRC Floating Concrete Hearth For Concrete Wood FiDocument11 pagesGFRC Floating Concrete Hearth For Concrete Wood FiJuliano. PQMNo ratings yet
- Our Changing WorldDocument3 pagesOur Changing Worlddinesh869863% (8)
- Criaturas Do Reino DistanteDocument53 pagesCriaturas Do Reino DistanteDaniel Marinho100% (1)
- 300+ TOP Production and Operation Management MCQs & AnswersDocument14 pages300+ TOP Production and Operation Management MCQs & AnswersPranoy SarkarNo ratings yet
- Embedded Systems (Eceg-5702) : Arduino ProgrammingDocument25 pagesEmbedded Systems (Eceg-5702) : Arduino ProgrammingmigadNo ratings yet
- Georgia Habitats Lesson PlansDocument5 pagesGeorgia Habitats Lesson PlansBecky BrownNo ratings yet
- View Result - CUMS Comprehensive University Management System - M.K.Bhavnagar University Powered by AuroMeera A College Management System ProviderDocument1 pageView Result - CUMS Comprehensive University Management System - M.K.Bhavnagar University Powered by AuroMeera A College Management System ProviderKiaanNo ratings yet