You might also like
- Boundaries 101: WorkbookDocument13 pagesBoundaries 101: WorkbookSarah Merchant97% (30)
- Ineffective Breathing PatternDocument3 pagesIneffective Breathing PatternReichelle Perlas62% (13)
- 5 NCP LaryngectomyDocument29 pages5 NCP LaryngectomyICa MarlinaNo ratings yet
- TONSILITIS AND ADENOIDITIS - Baldoza.E.Document9 pagesTONSILITIS AND ADENOIDITIS - Baldoza.E.Monette Abalos MendovaNo ratings yet
- Chest Fisioterapy in BronchiektasisDocument11 pagesChest Fisioterapy in BronchiektasisKhalila DiantiNo ratings yet
- Thyroidectomy Nursing Care PlanDocument2 pagesThyroidectomy Nursing Care PlanRnspeakcom100% (1)
- NCP Ineffective Airway ClearanceDocument4 pagesNCP Ineffective Airway ClearanceMary Joyce Limoico100% (1)
- Recruitment and Selection: Chapter 8: TESTINGDocument5 pagesRecruitment and Selection: Chapter 8: TESTINGErynne MoralesNo ratings yet
- CER - OSCAR 3 - C.1.1 - Rev. 2Document101 pagesCER - OSCAR 3 - C.1.1 - Rev. 2santiago100% (1)
- Tracheostomy: S.No: Time Specific Objective Content Teachin G Activity Learning Activity Av Aids EvaluationDocument13 pagesTracheostomy: S.No: Time Specific Objective Content Teachin G Activity Learning Activity Av Aids EvaluationaparnaNo ratings yet
- Assessment Nursing Diagnosis Scientific Analysis Planning Intervention Rationale EvaluationDocument20 pagesAssessment Nursing Diagnosis Scientific Analysis Planning Intervention Rationale EvaluationKen BaxNo ratings yet
- Surgery OSCEDocument23 pagesSurgery OSCEsumith_gunawardhana100% (8)
- Nursing Intervention Diagnose 1 Purpose and Criteria Results Intervention Rational NIC Labels Respiratory MonitoringDocument10 pagesNursing Intervention Diagnose 1 Purpose and Criteria Results Intervention Rational NIC Labels Respiratory MonitoringFhicholy Davied VanrioNo ratings yet
- NCP KoDocument1 pageNCP Kojiellianemae100% (1)
- Assessment Nursing Diagnosis Scientific Analysis Planning Intervention Rationale EvaluationDocument13 pagesAssessment Nursing Diagnosis Scientific Analysis Planning Intervention Rationale EvaluationKen BaxNo ratings yet
- PT of Endotrachealt Tube IntubationDocument28 pagesPT of Endotrachealt Tube IntubationBabita DhruwNo ratings yet
- Asilo, Rosette Justine D. BSN3Y2-1 NCMB 312 LECDocument3 pagesAsilo, Rosette Justine D. BSN3Y2-1 NCMB 312 LECRosette AsiloNo ratings yet
- NCP ProperDocument9 pagesNCP Properstephanie eduarteNo ratings yet
- 3.ET Tube Insertion .-1Document29 pages3.ET Tube Insertion .-1priyasivanandam1985No ratings yet
- WEEK 2 Management of Patients With Chest and Lower Respiratory Tract DisordersDocument9 pagesWEEK 2 Management of Patients With Chest and Lower Respiratory Tract DisordersTin tinNo ratings yet
- Ineffective Airway ClearanceDocument1 pageIneffective Airway ClearancejomerdalonaNo ratings yet
- Assessment Nursing Diagnosis Background Knowledge Plan of Care/Goal Nursing Interventions Rationale EvlatuationDocument3 pagesAssessment Nursing Diagnosis Background Knowledge Plan of Care/Goal Nursing Interventions Rationale EvlatuationgoyaNo ratings yet
- Kel 7 - Nursing Care PlanDocument3 pagesKel 7 - Nursing Care PlanWahda PrameswariNo ratings yet
- Risk For AspirationDocument2 pagesRisk For AspirationGly Mtg100% (6)
- Ineffective Breathing PatternDocument2 pagesIneffective Breathing PatternEna Katherine CanonoNo ratings yet
- ABCDE Assessment LecturioDocument12 pagesABCDE Assessment LecturioChristine Joy DeañoNo ratings yet
- Cues Nursing Diagnosis Inference Planning Nursing Intervention Rationale EvaluationDocument3 pagesCues Nursing Diagnosis Inference Planning Nursing Intervention Rationale EvaluationNichol John MalabananNo ratings yet
- Assessment Diagnosis Planning Interventions Rationale Evaluation Short-Term: Independent: A) Elevated Head of A) To TakeDocument2 pagesAssessment Diagnosis Planning Interventions Rationale Evaluation Short-Term: Independent: A) Elevated Head of A) To TakeANGEL AKIRA TORRESNo ratings yet
- NCP For Scenario BreathingDocument4 pagesNCP For Scenario Breathingmy moznNo ratings yet
- Assessment Nursing Diagnosis Scientific Analysis Planning Intervention Rationale Evaluation Subjective: (NoDocument19 pagesAssessment Nursing Diagnosis Scientific Analysis Planning Intervention Rationale Evaluation Subjective: (NoKen BaxNo ratings yet
- Cecilia, Issaiah Nicolle-Pneumothorax-NcpDocument7 pagesCecilia, Issaiah Nicolle-Pneumothorax-NcpIssaiah Nicolle Cecilia100% (1)
- Tim Keperawatan Gawat DaruratDocument53 pagesTim Keperawatan Gawat Daruratjihan febriyantiNo ratings yet
- Endotracheal Intubation-New and ImproveDocument5 pagesEndotracheal Intubation-New and ImprovePxPPxH ChanNo ratings yet
- Procedure PARACENTASISDocument11 pagesProcedure PARACENTASISaparnaNo ratings yet
- Leeson Plan New NebulizationDocument8 pagesLeeson Plan New NebulizationMakhanVerma100% (6)
- NCP For PneumoniaDocument3 pagesNCP For PneumoniaLeogalvez BedanoNo ratings yet
- Internet Scientific PublicationsDocument12 pagesInternet Scientific PublicationsAnonymous h0DxuJTNo ratings yet
- Nursing Process Care Plan For Ineffective Breathing Pattern Assessment Diagnosis Planning Implementation EvaluationDocument19 pagesNursing Process Care Plan For Ineffective Breathing Pattern Assessment Diagnosis Planning Implementation EvaluationZIANAH JOY FAMYNo ratings yet
- Morgan 307 342Document36 pagesMorgan 307 342Marta DumitracheNo ratings yet
- MS CourseTask8Document3 pagesMS CourseTask8Aria100% (1)
- SKILLS - Endo Defib ECartDocument8 pagesSKILLS - Endo Defib ECartDarwin AndalNo ratings yet
- AnesthesiaDocument24 pagesAnesthesiaakufahabaNo ratings yet
- MANAGEMENT PATIENT VENTILATION.2019.Ns - Nurma NewDocument93 pagesMANAGEMENT PATIENT VENTILATION.2019.Ns - Nurma NewHaris SaepulohNo ratings yet
- Assessme NT Diagnosis Planning Intervention Rationale EvaluationDocument6 pagesAssessme NT Diagnosis Planning Intervention Rationale EvaluationDan HizonNo ratings yet
- MCN NCPDocument4 pagesMCN NCPPEARL CHRISTINE CUDALNo ratings yet
- NCPDocument7 pagesNCPRuth MontebonNo ratings yet
- LP BSN (Askep Dispnea)Document8 pagesLP BSN (Askep Dispnea)rickyNo ratings yet
- Bukidnon State University: Subjective: Short Term: Short TermDocument1 pageBukidnon State University: Subjective: Short Term: Short TermSimbo Ralph JulesNo ratings yet
- D. Nursing Care Plan: Impaired Gas Exchange Related To Altered Oxygen Supply As Evidenced by Difficulty in BreathingDocument2 pagesD. Nursing Care Plan: Impaired Gas Exchange Related To Altered Oxygen Supply As Evidenced by Difficulty in BreathingReinette LastrillaNo ratings yet
- Nursing Care Plan Assessment Explanation of The Problem Goals and Objectives Intervention Rationale EvaluationDocument10 pagesNursing Care Plan Assessment Explanation of The Problem Goals and Objectives Intervention Rationale EvaluationGuile RilleraNo ratings yet
- Intubasi Endoktrakheal 2020Document53 pagesIntubasi Endoktrakheal 2020Octa VianiNo ratings yet
- NCP Acute BronchitisDocument9 pagesNCP Acute BronchitisCarl Simon CalingacionNo ratings yet
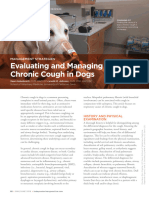
- TVP-2019-0506 Managing Chronic CoughDocument6 pagesTVP-2019-0506 Managing Chronic CoughRic Raphael PiodenaNo ratings yet
- Data NSG Diagnosis Goals & Outcomes NSG Interventions Rationale Evaluation O: StoDocument3 pagesData NSG Diagnosis Goals & Outcomes NSG Interventions Rationale Evaluation O: StoClaudineNo ratings yet
- Modern Anaesthesia:: A Concise Guide to the Study and Practice of Anaesthesia.From EverandModern Anaesthesia:: A Concise Guide to the Study and Practice of Anaesthesia.No ratings yet
- Monitoring Mechanical Ventilation Using Ventilator WaveformsFrom EverandMonitoring Mechanical Ventilation Using Ventilator WaveformsNo ratings yet
- Percutaneous Emergency Oxygenation Strategies in the “Can’t Intubate, Can’t Oxygenate” Scenario: PEOS in the CICO Scenario, #2From EverandPercutaneous Emergency Oxygenation Strategies in the “Can’t Intubate, Can’t Oxygenate” Scenario: PEOS in the CICO Scenario, #2No ratings yet
- Unit 4 - Emergency Drugs - Table FormDocument5 pagesUnit 4 - Emergency Drugs - Table FormTESORO Zeus DavidNo ratings yet
- How To Positive CBTDocument21 pagesHow To Positive CBTJASMINE JOSEPH 2270082No ratings yet
- Reverse Facial Mask PDFDocument6 pagesReverse Facial Mask PDFمحمد عبدالهادي إسماعيلNo ratings yet
- History TakingDocument51 pagesHistory TakingJAMES TONNY OKINYINo ratings yet
- Understanding Bipolar Disorder The Essential Family Guide (BPD) (Aimee Daramus)Document151 pagesUnderstanding Bipolar Disorder The Essential Family Guide (BPD) (Aimee Daramus)Tanvi Gupta100% (1)
- EkgDocument75 pagesEkgRamot Tribaya Recardo PardedeNo ratings yet
- 5 LD02 Week 1 SlidesDocument51 pages5 LD02 Week 1 SlidesDunjaNo ratings yet
- 3 Kerala PSC Staff Nurse Insurance Medical Services Previous Question - Kerala PSC QuestionsDocument9 pages3 Kerala PSC Staff Nurse Insurance Medical Services Previous Question - Kerala PSC QuestionsMrudula SureshNo ratings yet
- Versele Laga Wegwijzer Duivencataloog 2017 4t Final Oe LRDocument148 pagesVersele Laga Wegwijzer Duivencataloog 2017 4t Final Oe LRTomitaNo ratings yet
- LGBTQDocument2 pagesLGBTQAkuryo ChaNo ratings yet
- The Complete Google Manual - 5th Edition 2020Document147 pagesThe Complete Google Manual - 5th Edition 2020dentaraNo ratings yet
- How Are Habits Formed - Modelling Habit Formation in The Real World PDFDocument13 pagesHow Are Habits Formed - Modelling Habit Formation in The Real World PDFWesley RicardoNo ratings yet
- Self MonitoringDocument6 pagesSelf MonitoringHilal KhattakNo ratings yet
- Acceptable Prescribing Terms and Abbreviations PosterDocument1 pageAcceptable Prescribing Terms and Abbreviations PosterAdelNo ratings yet
- Neuman S System ModelDocument12 pagesNeuman S System ModelmajoodhNo ratings yet
- IGCSE Coursework Practise - Thunberg Assignment 1Document22 pagesIGCSE Coursework Practise - Thunberg Assignment 1sony reactsNo ratings yet
- Bias in Research: A Review PaperDocument7 pagesBias in Research: A Review PaperNora ElaNo ratings yet
- VRTS114 Final Exam-1Document2 pagesVRTS114 Final Exam-1ivy bernalNo ratings yet
- Nursing Patient InteractionDocument2 pagesNursing Patient InteractionAnneMyl's OL'ShoppeNo ratings yet
- Mancera Medication SheetDocument2 pagesMancera Medication SheetVince ManceraNo ratings yet
- Barriers To Addressing Conflict & Recommended ResponsesDocument1 pageBarriers To Addressing Conflict & Recommended ResponsesJerry Manzano Caberto Jr.No ratings yet
- Sun 2013Document7 pagesSun 2013Sirine LimemeNo ratings yet
- Orient - Family Care - HAAD - Medical Application Form - Apr 2019Document7 pagesOrient - Family Care - HAAD - Medical Application Form - Apr 2019AAMIRNo ratings yet
- Phil-Iri 2021-2022Document6 pagesPhil-Iri 2021-2022ShaiAbretilNieloMalinaoNo ratings yet
- Internship PresentationDocument23 pagesInternship Presentationapi-556937362No ratings yet
- IQ SampleDocument6 pagesIQ SamplenesumaNo ratings yet
- Gap Filling 2Document10 pagesGap Filling 2cocoNo ratings yet