You might also like
- 5 Principles of Problem SolvingDocument2 pages5 Principles of Problem Solvinggupta_rk06100% (1)
- Unbreakable Minds Documentary AssignmentDocument6 pagesUnbreakable Minds Documentary Assignmentbonnie moenNo ratings yet
- Synthesis Essay OutlineDocument2 pagesSynthesis Essay OutlineKid KulafuNo ratings yet
- Ant and GrasshopperDocument12 pagesAnt and Grasshopperkenny stoneNo ratings yet
- Dyslexia Assessment For Languages of India (DALI) : October 2015Document4 pagesDyslexia Assessment For Languages of India (DALI) : October 2015Shaheen AlviNo ratings yet
- Research Paper On Mental HealthDocument63 pagesResearch Paper On Mental HealthDivyajeet SinghNo ratings yet
- The Satir Model: Yesterday and Today: John BanmenDocument16 pagesThe Satir Model: Yesterday and Today: John BanmenLaura LinaresNo ratings yet
- NIEPID Indian Test of IntelligenceDocument143 pagesNIEPID Indian Test of IntelligenceMalu RajanNo ratings yet
- Inventing Medical Devices – a Perspective from IndiaFrom EverandInventing Medical Devices – a Perspective from IndiaRating: 5 out of 5 stars5/5 (6)
- HGPQ2L2 - My Journey To A Stronger MeDocument9 pagesHGPQ2L2 - My Journey To A Stronger MeRico PalmaNo ratings yet
- Three-Level Model of FeedbackDocument19 pagesThree-Level Model of FeedbackRODOLFO R. SALIGAN67% (3)
- The Protocol For Correction of Birth TimeDocument277 pagesThe Protocol For Correction of Birth TimeAди С.100% (1)
- IndianJPsychiatry CPG Assessment CAPDocument19 pagesIndianJPsychiatry CPG Assessment CAPGFGFNo ratings yet
- Parental Care-Seeking Pathway and Challenges For Autistic SpectrumDocument8 pagesParental Care-Seeking Pathway and Challenges For Autistic SpectrumKarel GuevaraNo ratings yet
- The Positive Mental Health Instrument: Development and Validation of A Culturally Relevant Scale in A Multi-Ethnic Asian PopulationDocument19 pagesThe Positive Mental Health Instrument: Development and Validation of A Culturally Relevant Scale in A Multi-Ethnic Asian PopulationFebrio IglesiasNo ratings yet
- CORONA VIRUS - PublishedDocument8 pagesCORONA VIRUS - PublishedPremkant UparikarNo ratings yet
- Impact of Psychoeducation Intervention Module On Parents of Children With Autism Spectrum Disorders: A Preliminary StudyDocument7 pagesImpact of Psychoeducation Intervention Module On Parents of Children With Autism Spectrum Disorders: A Preliminary Studysushmita bhartiaNo ratings yet
- Research Paper 2Document5 pagesResearch Paper 2Máthé AdriennNo ratings yet
- Qualitative Research Methods in Psychiatry in India: Landscaping The TerrainDocument10 pagesQualitative Research Methods in Psychiatry in India: Landscaping The Terraingion.nandNo ratings yet
- Clinical Practice Guidelines For Assessment and Management of Intellectual DisabilityDocument17 pagesClinical Practice Guidelines For Assessment and Management of Intellectual DisabilityCristinaNo ratings yet
- IJP FamiyInterventionsPDFDocument10 pagesIJP FamiyInterventionsPDFspurthi_16No ratings yet
- IndianJPsychiatry CPG Assessment CAPDocument19 pagesIndianJPsychiatry CPG Assessment CAPMaia MachavarianiNo ratings yet
- Id and CBT SS21Document15 pagesId and CBT SS21Nathalie MarinhoNo ratings yet
- The Effect of Mindfulness-Based Cognitive TherapyDocument11 pagesThe Effect of Mindfulness-Based Cognitive Therapym01.abousalehNo ratings yet
- From The Desk of Vice President-Elect: Mrugesh VaishnavDocument1 pageFrom The Desk of Vice President-Elect: Mrugesh Vaishnavgion.nandNo ratings yet
- 3nov newHCSTpaperDocument15 pages3nov newHCSTpaperSrilatha GirishNo ratings yet
- The Burden of Mental Disorders Across The States of India: The Global Burden of Disease Study 1990-2017Document15 pagesThe Burden of Mental Disorders Across The States of India: The Global Burden of Disease Study 1990-2017Dhawal PatelNo ratings yet
- 19BMS134 - Divyajeet Singh'Document63 pages19BMS134 - Divyajeet Singh'Divyajeet SinghNo ratings yet
- Monteiro (2020) - Mproving Work Performance - Examining The Role of Mindfulness and Perceived Control of Internal States in Work EngagementDocument8 pagesMonteiro (2020) - Mproving Work Performance - Examining The Role of Mindfulness and Perceived Control of Internal States in Work EngagementJessNo ratings yet
- Effectiveness of Parenting Skill Program On Childs Adaptive Behavioramong Parents of Children With Intellectual Developmental DisabilityDocument10 pagesEffectiveness of Parenting Skill Program On Childs Adaptive Behavioramong Parents of Children With Intellectual Developmental DisabilityIJAR JOURNALNo ratings yet
- Letter To The EditorDocument2 pagesLetter To The Editorkashish behlNo ratings yet
- Adaptation of The Mental Health Inventory MHI-38 For Adolescents - Indonesian VersionDocument12 pagesAdaptation of The Mental Health Inventory MHI-38 For Adolescents - Indonesian VersionREFIDA MUTIANo ratings yet
- Neeri Batra 2Document1 pageNeeri Batra 2Neeri BatraNo ratings yet
- Founding and Managing Health CareDocument9 pagesFounding and Managing Health CarekrishnaNo ratings yet
- Patanapu Effect of Motivation On Oral Hygiene and Caries Status Among YoungDocument7 pagesPatanapu Effect of Motivation On Oral Hygiene and Caries Status Among YoungbomonnhacongdongNo ratings yet
- Evaluation of IQ in Children With Developmental Coordination DisorderDocument4 pagesEvaluation of IQ in Children With Developmental Coordination DisorderInternational Journal of Innovative Science and Research Technology100% (1)
- Personal Growth Initiative Scale - INDIAN YOUTHDocument9 pagesPersonal Growth Initiative Scale - INDIAN YOUTHeva pandanaNo ratings yet
- The Effect of Cognitive Rehabilitation Physical AnDocument13 pagesThe Effect of Cognitive Rehabilitation Physical AnFlorentina FerariuNo ratings yet
- 1 s2.0 S2352081717300028 MainDocument6 pages1 s2.0 S2352081717300028 MainSantosh KumarNo ratings yet
- Intake Assessment and Diagnostic Accuracy of Attention Deficit Hyperactivity Disorder Diagnostic Scale Being Developed For Children in NepalDocument6 pagesIntake Assessment and Diagnostic Accuracy of Attention Deficit Hyperactivity Disorder Diagnostic Scale Being Developed For Children in NepalNarmada DevkotaNo ratings yet
- The Role of AYUSH in Mental Well BeingDocument16 pagesThe Role of AYUSH in Mental Well BeingMunja nikhithaNo ratings yet
- Agrawal 2015 Psychology - in - India - A - Career - With - Uncertain - OpportunitiesDocument8 pagesAgrawal 2015 Psychology - in - India - A - Career - With - Uncertain - OpportunitiesHvovi BhagwagarNo ratings yet
- Jurnal PenelitianDocument15 pagesJurnal PenelitianM . ARIF RAHMAN GUS RIWANo ratings yet
- Pep RDocument12 pagesPep Rnays meetNo ratings yet
- Mysore Kaku 2023 Predictors of Outcome in Autism Spectrum Disorders A Perspective For Clinicians and TherapistsDocument5 pagesMysore Kaku 2023 Predictors of Outcome in Autism Spectrum Disorders A Perspective For Clinicians and TherapistsIngrid OlmedoNo ratings yet
- Efficacy of Psychoeducation To Improve Medication Adherence Among Bipolar Affective Disorder: A Systematic ReviewDocument6 pagesEfficacy of Psychoeducation To Improve Medication Adherence Among Bipolar Affective Disorder: A Systematic Reviewvaideeswari kumar100% (1)
- RuralUrbanCorrelates IntJComMedPubHealthOct2017Document9 pagesRuralUrbanCorrelates IntJComMedPubHealthOct2017dhruv goraiNo ratings yet
- Bmifa Girls Z 5 19 LabelsDocument16 pagesBmifa Girls Z 5 19 Labelsg_pinasthikaNo ratings yet
- New Microsoft Word Document Spiritual IntelligenceDocument10 pagesNew Microsoft Word Document Spiritual Intelligenceanon_428724820No ratings yet
- Cognitive RemediationDocument7 pagesCognitive RemediationDaniela Ulloa CarrascoNo ratings yet
- Impact of Vitamin D On Cognitive Functions in Healthy IndividualsDocument14 pagesImpact of Vitamin D On Cognitive Functions in Healthy IndividualsMarlene LírioNo ratings yet
- Complete Journal SRJI Vol-1 No-2 Year 2012Document42 pagesComplete Journal SRJI Vol-1 No-2 Year 2012Dr. Krishna N. SharmaNo ratings yet
- 1 s2.0 S0891422216301871 MainDocument10 pages1 s2.0 S0891422216301871 MainMartina GuzmanNo ratings yet
- FFMQ Validasi Bahasa 2022 Sinta 3Document20 pagesFFMQ Validasi Bahasa 2022 Sinta 3Human CapitalNo ratings yet
- MCFTL-02 Mental Health and Disorders - Supervised Practicum PDFDocument115 pagesMCFTL-02 Mental Health and Disorders - Supervised Practicum PDFBGangadharReddyNo ratings yet
- The Relationship Between Emotional Intelligence With General Health and Academic Achievement: A Case Study in Iran's Health SystemDocument6 pagesThe Relationship Between Emotional Intelligence With General Health and Academic Achievement: A Case Study in Iran's Health Systemarhyani paliNo ratings yet
- Assessment of Spiritual Intelligence Spiritual PraDocument11 pagesAssessment of Spiritual Intelligence Spiritual PraM. YusufNo ratings yet
- Beginning Steps in School Mental Health in India: A Teacher WorkshopDocument6 pagesBeginning Steps in School Mental Health in India: A Teacher WorkshopRohit Timothy KatumallaNo ratings yet
- Counsellors Manual For Family Intevention in Mental RetardationDocument79 pagesCounsellors Manual For Family Intevention in Mental RetardationDanielNo ratings yet
- Promotion and Prevention in Child Mental Health: Appropriate????Document8 pagesPromotion and Prevention in Child Mental Health: Appropriate????deepti sharmaNo ratings yet
- Counselingand Family Therapyin IndiaDocument13 pagesCounselingand Family Therapyin IndiaPooja GanekarNo ratings yet
- Ahmad Et AlDocument6 pagesAhmad Et AlAmyatenaNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument26 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- Pms 110 C 1139-1148Document10 pagesPms 110 C 1139-1148adnanjivrakNo ratings yet
- Early Stage Detection of Autism Spectrum Disorder Using Machine LearningDocument7 pagesEarly Stage Detection of Autism Spectrum Disorder Using Machine LearningIJRASETPublicationsNo ratings yet
- Efficacy of in Preterm Infants-A Comparative Pilot Study SuvarnaprashanDocument8 pagesEfficacy of in Preterm Infants-A Comparative Pilot Study SuvarnaprashanVENU B ANo ratings yet
- DR NuwanSMarasinhgacpaetyparticleDocument18 pagesDR NuwanSMarasinhgacpaetyparticleSanjanaNo ratings yet
- Impact of Psychosocial Intervention On Emotional Disorders and Medication Adherence in HIV/AIDSDocument227 pagesImpact of Psychosocial Intervention On Emotional Disorders and Medication Adherence in HIV/AIDS3PA21Kaysta Ardeia La NandaNo ratings yet
- EvaluationDocument1 pageEvaluationvasu1311No ratings yet
- REPORT1ADocument1 pageREPORT1Avasu1311No ratings yet
- SP EduDocument2 pagesSP Eduvasu1311No ratings yet
- Quality AssuranceDocument1 pageQuality Assurancevasu1311No ratings yet
- CASE1BDocument2 pagesCASE1Bvasu1311No ratings yet
- Intro 1 ADocument1 pageIntro 1 Avasu1311No ratings yet
- IntrDocument1 pageIntrvasu1311No ratings yet
- Results: For 2014, The Overall Prevalence of ASD Among The 11 ADDM SitesDocument1 pageResults: For 2014, The Overall Prevalence of ASD Among The 11 ADDM Sitesvasu1311No ratings yet
- MethodDocument2 pagesMethodvasu1311No ratings yet
- Mindful ParentingDocument3 pagesMindful Parentingvasu1311No ratings yet
- De-Escalation StratergiesDocument4 pagesDe-Escalation Stratergiesvasu1311No ratings yet
- Mindful ParentingDocument3 pagesMindful Parentingvasu1311No ratings yet
- AnxietyDocument2 pagesAnxietyvasu1311No ratings yet
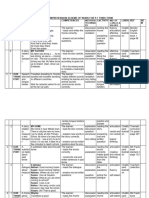
- P.1 English Comprehension Scheme of Work For Third TermDocument5 pagesP.1 English Comprehension Scheme of Work For Third TermBagambe BarnarbasNo ratings yet
- p2 QuestionsDocument8 pagesp2 QuestionsVibha RaviNo ratings yet
- Obadiah PPT Final DefenseDocument37 pagesObadiah PPT Final DefenseZenaida FeliasNo ratings yet
- Interviwe Questions (Inspector Customs)Document4 pagesInterviwe Questions (Inspector Customs)jumper200No ratings yet
- Best Practices in Math and Art PotteryDocument1 pageBest Practices in Math and Art Potteryapi-78060499No ratings yet
- Rubric Site VisitDocument3 pagesRubric Site Visitapi-501066857No ratings yet
- The Triangular Theory of LoveDocument12 pagesThe Triangular Theory of LoveJasmine PeraltaNo ratings yet
- HUM ND ETH 1st Year CourseDocument2 pagesHUM ND ETH 1st Year CourseWarrior SoulNo ratings yet
- 6 SWOT AnalysisDocument2 pages6 SWOT AnalysisScooby DooNo ratings yet
- Numbers Class 4Document2 pagesNumbers Class 4anitaNo ratings yet
- Lesson 1the Discipline of Counseling-Goals-Part 2 PDFDocument23 pagesLesson 1the Discipline of Counseling-Goals-Part 2 PDFEmelita Riego RodelasNo ratings yet
- Formal and Informal Words With Meanings and Phrases For Esl Igcse 0510Document5 pagesFormal and Informal Words With Meanings and Phrases For Esl Igcse 0510rehaumzainNo ratings yet
- Importance of Quantitative Research Across FieldDocument6 pagesImportance of Quantitative Research Across FieldAdaill JosephNo ratings yet
- IDC 2022 The Leadership Project1Document3 pagesIDC 2022 The Leadership Project1vcontini04No ratings yet
- 4.9.1. How To Teach GrammarDocument27 pages4.9.1. How To Teach GrammarPhiwokuhle ThubelihleNo ratings yet
- (Tài Liệu KYS) U1 TheoryDocument22 pages(Tài Liệu KYS) U1 TheoryHùng TrươngNo ratings yet
- Signal LearningDocument3 pagesSignal LearningJan Lemuel Fortaleza RefuncionNo ratings yet
- Jacob Gewirtz - J. B. Watson's Approach To Learning: Why Pavlov? Why Not Thorndike?Document3 pagesJacob Gewirtz - J. B. Watson's Approach To Learning: Why Pavlov? Why Not Thorndike?Irving Pérez MéndezNo ratings yet
- Module 1 - Lesson 1 Page 7-8 OnlyDocument12 pagesModule 1 - Lesson 1 Page 7-8 OnlyJosenia ConstantinoNo ratings yet
- Interpersonal and Intrapersonal Intelligences Do TDocument5 pagesInterpersonal and Intrapersonal Intelligences Do TDaniela SolisNo ratings yet
- Initial Assessment Template 3Document3 pagesInitial Assessment Template 3JORGE MARINNo ratings yet
- Court of Dragons and Ashes The Dragon Crown Series Book 3 1St Edition G Bailey Full ChapterDocument67 pagesCourt of Dragons and Ashes The Dragon Crown Series Book 3 1St Edition G Bailey Full Chapterjohn.haase983100% (4)