You might also like
- Emergency Care Algorithms 2022Document88 pagesEmergency Care Algorithms 2022Gustavo Paredes0% (1)
- NURSING CARE PLAN For Myocardial InfarctionDocument13 pagesNURSING CARE PLAN For Myocardial Infarctionbanyenye2593% (14)
- Assess Appropriateness For Clinical Condition. Heart Rate Typically 150/min If TachyarrhythmiaDocument1 pageAssess Appropriateness For Clinical Condition. Heart Rate Typically 150/min If TachyarrhythmiaSiti Nur R Firda FauziyahNo ratings yet
- AlgorithmACLS Tachycardia 200612Document1 pageAlgorithmACLS Tachycardia 200612YassarNo ratings yet
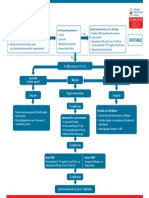
- AdultTachycardiaWithPulse AlgorithmDocument1 pageAdultTachycardiaWithPulse AlgorithmIsmail SlimNo ratings yet
- 2010 Integrated Updated Circulation ACLS Tachycardia AlgorithmDocument1 page2010 Integrated Updated Circulation ACLS Tachycardia AlgorithmRyggie ComelonNo ratings yet
- Tachycardia With A Pulse Algorithm: Assess Appropriateness For Clinical ConditionDocument1 pageTachycardia With A Pulse Algorithm: Assess Appropriateness For Clinical ConditionDendy Frannuzul RamadhanNo ratings yet
- AlgorithmACLStachycardiawithapulse PDFDocument1 pageAlgorithmACLStachycardiawithapulse PDFDendy Frannuzul RamadhanNo ratings yet
- AlgorithmACLS Tachycardia 200612Document1 pageAlgorithmACLS Tachycardia 200612must dietNo ratings yet
- Adult Tachycardia With A Pulse Algorithm: Doses/DetailsDocument1 pageAdult Tachycardia With A Pulse Algorithm: Doses/DetailsZakiyahulfahdwNo ratings yet
- Adult Tachycardia With A Pulse Algorithm: Doses/DetailsDocument1 pageAdult Tachycardia With A Pulse Algorithm: Doses/DetailsAlexis HospitalNo ratings yet
- Tachycardia AlgorythmDocument1 pageTachycardia AlgorythmUZNAPMNo ratings yet
- Algoritma Ambulance - PHCDocument11 pagesAlgoritma Ambulance - PHCYassarNo ratings yet
- Website Tachycardia Algorithm DiagramDocument1 pageWebsite Tachycardia Algorithm Diagramcolette zgheibNo ratings yet
- G2015 Adult Tachycardia PDFDocument1 pageG2015 Adult Tachycardia PDFPlabber JuneNo ratings yet
- G2015 Adult Tachycardia PDFDocument1 pageG2015 Adult Tachycardia PDFibbs91No ratings yet
- Adult Tachycardia (With Pulse) AlgorithmDocument1 pageAdult Tachycardia (With Pulse) AlgorithmJames ChoiNo ratings yet
- Managemen Disritmia: Dr. Rofika Hanifa, SPPDDocument20 pagesManagemen Disritmia: Dr. Rofika Hanifa, SPPDavivlabirdNo ratings yet
- Algoritmos AHA ACLS AdultoDocument4 pagesAlgoritmos AHA ACLS AdultoChristianFelipePorrasCastroNo ratings yet
- AlgorithmsDocument16 pagesAlgorithmsirish laglevaNo ratings yet
- Pediatric Tachycardia With A Pulse Algorithm: Yes NoDocument1 pagePediatric Tachycardia With A Pulse Algorithm: Yes NoRatna TambaNo ratings yet
- With A Pulse and Poor Perfusion: Pediatric TachycardiaDocument1 pageWith A Pulse and Poor Perfusion: Pediatric TachycardiaIin-Ignasia Diahayujulindah Mujiman0% (1)
- Obat-Obatan Dalam Bantuan Hidup LanjutDocument16 pagesObat-Obatan Dalam Bantuan Hidup LanjutTheresia SihotangNo ratings yet
- Tachycardia AlgorithmDocument1 pageTachycardia AlgorithmGideon BahuleNo ratings yet
- 5.ALS Algorithms TachycardiaDocument1 page5.ALS Algorithms TachycardiaMassimo Di BenedettoNo ratings yet
- ALS Algorithms LS Tachycardia 2.0Document1 pageALS Algorithms LS Tachycardia 2.0Lucian Alin DinuNo ratings yet
- Initial Recommended Doses NarrowDocument1 pageInitial Recommended Doses NarrowwisgeorgekwokNo ratings yet
- Advanced Cardiac Life SupportDocument37 pagesAdvanced Cardiac Life SupportRoy Acosta GumbanNo ratings yet
- Adenosine: Scheduling BLS (CPR/First Aid) Acls PalsDocument4 pagesAdenosine: Scheduling BLS (CPR/First Aid) Acls PalsPhilippe Ceasar C. BascoNo ratings yet
- Pediatric Bradycardia With A Pulse and Poor Perfusion AlgorithmDocument1 pagePediatric Bradycardia With A Pulse and Poor Perfusion AlgorithmRadhiatul MardhiahNo ratings yet
- ACLS Algorithm Pulse No Yes: Stable Patient Unstable Patient Stable PatientDocument1 pageACLS Algorithm Pulse No Yes: Stable Patient Unstable Patient Stable PatientAhmed AlkhaqaniNo ratings yet
- 3 Combined AHA BLS ACLS Updates CombinedDocument5 pages3 Combined AHA BLS ACLS Updates Combinedamanrup randhawa100% (1)
- ACLS 2015 Guidelines Upate Nov 2016 For PostingDocument2 pagesACLS 2015 Guidelines Upate Nov 2016 For PostingOana - Andreea CristeaNo ratings yet
- Note: Dosage May Be Gradually Increased Over: AmlodipineDocument4 pagesNote: Dosage May Be Gradually Increased Over: Amlodipineanette katrinNo ratings yet
- Adult BradycardiaDocument1 pageAdult BradycardiaTista ApriyanaNo ratings yet
- ACLS Tachycardia Algorithm For Managing Stable TachycardiaDocument4 pagesACLS Tachycardia Algorithm For Managing Stable TachycardiaLady MuffinsNo ratings yet
- Cardiology Exam 2 - Lecture Notes: Treating Adult BradycardiaDocument5 pagesCardiology Exam 2 - Lecture Notes: Treating Adult BradycardiaAddieNo ratings yet
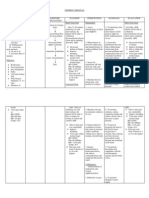
- Name of Drug Dosage/ Frequency / Timing/ Route Mechanism of Action Indication Contraindic Ation Adverse Effect Nursing ResponsibilitiesDocument3 pagesName of Drug Dosage/ Frequency / Timing/ Route Mechanism of Action Indication Contraindic Ation Adverse Effect Nursing ResponsibilitiesphoebeNo ratings yet
- Adult BradycardiaDocument1 pageAdult BradycardiaTista ApriyanaNo ratings yet
- Generic Name: Adult: IVDocument3 pagesGeneric Name: Adult: IVBasema HashhashNo ratings yet
- Dx. StudyDocument3 pagesDx. Studymayumitanaka8042No ratings yet
- Drug Study - AmlodipineDocument2 pagesDrug Study - AmlodipineKian HerreraNo ratings yet
- AdenosineDocument2 pagesAdenosinegovind_soni_150% (1)
- Algo Bradycardia DikonversiDocument5 pagesAlgo Bradycardia DikonversiDaniel SitungkirNo ratings yet
- Drug Classification of AmlodepineDocument5 pagesDrug Classification of Amlodepineshai raNo ratings yet
- Ecgs and Acute Cardiac Events: Yuniardi Alriyanto, MD Doris Sylvanus Hospital PalangkarayaDocument47 pagesEcgs and Acute Cardiac Events: Yuniardi Alriyanto, MD Doris Sylvanus Hospital PalangkarayaAuliaRusdiAllmuttaqienNo ratings yet
- Tachycardia Algorithm 2021Document1 pageTachycardia Algorithm 2021Ravin DebieNo ratings yet
- AlgorithmACLSBradycardiawithapulse PDFDocument1 pageAlgorithmACLSBradycardiawithapulse PDFjohndoe1995No ratings yet
- Pals Pediatric BradycardiaDocument1 pagePals Pediatric BradycardiadarlingcarvajalduqueNo ratings yet
- Ecg ReadingsDocument11 pagesEcg ReadingsAnton Laurenciana100% (5)
- Ecg Dysrythmias Nursing Responsibilitu Sinus Node 1.) Sinus BradycardiaDocument2 pagesEcg Dysrythmias Nursing Responsibilitu Sinus Node 1.) Sinus BradycardiaNickha LazoNo ratings yet
- Pals TachycardiaDocument1 pagePals TachycardiadarlingcarvajalduqueNo ratings yet
- ACLS Drug TherapyDocument8 pagesACLS Drug TherapySahrensNo ratings yet
- Bradycardia AlgorithmDocument1 pageBradycardia AlgorithmGideon BahuleNo ratings yet
- DRUG STUDY ICU and ACSDocument22 pagesDRUG STUDY ICU and ACSSheila Mae ReyesNo ratings yet
- Drug Study On Emergency DrugsDocument28 pagesDrug Study On Emergency DrugsRaidis PangilinanNo ratings yet
- Nursing CS Treatment-Of-Atrial-Dysrhythmias 02Document1 pageNursing CS Treatment-Of-Atrial-Dysrhythmias 02frankshro156No ratings yet
- Dundee Epidemiology and Biostatistics Unit: Measures of AgreementDocument36 pagesDundee Epidemiology and Biostatistics Unit: Measures of AgreementYudhistira AdiNo ratings yet
- Subject-Verb Agreement: Brenham Writing Room Created by D. HerringDocument13 pagesSubject-Verb Agreement: Brenham Writing Room Created by D. HerringYudhistira AdiNo ratings yet
- DRAFT V1.0 - 2/26/04: Memorandum of UnderstandingDocument4 pagesDRAFT V1.0 - 2/26/04: Memorandum of UnderstandingYudhistira AdiNo ratings yet
- Protocol AddendumDocument9 pagesProtocol AddendumYudhistira AdiNo ratings yet
- AP Graduate Admissions Form 2016Document4 pagesAP Graduate Admissions Form 2016Yudhistira AdiNo ratings yet
- Graduate Instruction and Research in Astronomy at Bologna UniversityDocument25 pagesGraduate Instruction and Research in Astronomy at Bologna UniversityYudhistira AdiNo ratings yet
- Agreement On Cooperation in Astrophysics: Article 1Document9 pagesAgreement On Cooperation in Astrophysics: Article 1Yudhistira AdiNo ratings yet
- Higgs QNDocument40 pagesHiggs QNYudhistira AdiNo ratings yet
- 160802Document1 page160802Yudhistira AdiNo ratings yet
- Quot Myanmar Type DDocument1 pageQuot Myanmar Type DYudhistira AdiNo ratings yet
- Berdikari 2296Document1 pageBerdikari 2296Yudhistira AdiNo ratings yet
- Higgs Boson and Beyond:: The Quest For New Laws of PhysicsDocument1 pageHiggs Boson and Beyond:: The Quest For New Laws of PhysicsYudhistira AdiNo ratings yet
- Case ReportDocument8 pagesCase ReportYudhistira AdiNo ratings yet
- Case Report:: Cystic MeningiomaDocument11 pagesCase Report:: Cystic MeningiomaYudhistira AdiNo ratings yet
- 14.1 The Hole Inside The Heart ABSTRAKDocument11 pages14.1 The Hole Inside The Heart ABSTRAKYudhistira AdiNo ratings yet
- Pathophysiology Congenital Heart Disease-1Document54 pagesPathophysiology Congenital Heart Disease-1single_ladyNo ratings yet
- Emergency Red Flags: DR - Magdy Khames AlyDocument58 pagesEmergency Red Flags: DR - Magdy Khames AlyJerry AbleNo ratings yet
- GIT 08-09 2nd Year PhysiotherapyDocument96 pagesGIT 08-09 2nd Year Physiotherapydileca1448No ratings yet
- HaemoglobinDocument47 pagesHaemoglobinPreethi AbhilashNo ratings yet
- Heart Failure With Reduced Ejection FractionDocument11 pagesHeart Failure With Reduced Ejection Fractionpricilia ardianiNo ratings yet
- Association Between Periodontitis and Glycosylated HaemoglobinDocument11 pagesAssociation Between Periodontitis and Glycosylated HaemoglobinAndrea MorenoNo ratings yet
- A Guide To Peripheral EdemaDocument7 pagesA Guide To Peripheral Edemadanny17phNo ratings yet
- Skinner 2001Document13 pagesSkinner 2001Dany ZailaniNo ratings yet
- FON Question BankDocument5 pagesFON Question Bankramzan aliNo ratings yet
- Instruction Manual: Multi Modality Electrical StimulatorDocument49 pagesInstruction Manual: Multi Modality Electrical StimulatorBrendaNo ratings yet
- Quiz 4Document12 pagesQuiz 4abezareljvenNo ratings yet
- High Yield Surgery Compatible Version PDFDocument20 pagesHigh Yield Surgery Compatible Version PDFSurgery CSC1No ratings yet
- PDF Basic Physiology For Anaesthetists 2Nd Edition David Chambers Ebook Full ChapterDocument53 pagesPDF Basic Physiology For Anaesthetists 2Nd Edition David Chambers Ebook Full Chaptersamuel.eskind860100% (2)
- Rheumatic Heart Disease: Infectious Diseases of The HeartDocument5 pagesRheumatic Heart Disease: Infectious Diseases of The HeartVoid LessNo ratings yet
- 2015 Updated Beers CriteriaDocument20 pages2015 Updated Beers CriteriaJuniorNo ratings yet
- 99 TMCPractice QuestionsDocument31 pages99 TMCPractice QuestionsGustavo OlguinNo ratings yet
- NURS 1301 Editing CVA CASE Study Need To FinishDocument13 pagesNURS 1301 Editing CVA CASE Study Need To FinishabbieNo ratings yet
- Paediatric Cardiovascular Examination OSCE GuideDocument24 pagesPaediatric Cardiovascular Examination OSCE GuideJeremiah KollieNo ratings yet
- GIO: Study The Organs Involved in The Excretory System. SioDocument4 pagesGIO: Study The Organs Involved in The Excretory System. SioAngelica BelleNo ratings yet
- Medical Examiner InvestigationDocument11 pagesMedical Examiner InvestigationColleen WelcherNo ratings yet
- CPR Critical SkillsDocument2 pagesCPR Critical SkillsErickson Tiu100% (1)
- Common Non-Communicable DiseasesDocument28 pagesCommon Non-Communicable DiseasesDanica AdamosNo ratings yet
- Refractory Anaphylaxis Algorithm 2021Document1 pageRefractory Anaphylaxis Algorithm 2021ay254No ratings yet
- SepsisDocument8 pagesSepsisLEONELA VALDES CABELLONo ratings yet
- Dengue Guidelines For Electronic Circulation - CompressedDocument73 pagesDengue Guidelines For Electronic Circulation - CompressedakeelNo ratings yet
- AIIMS (MBBS) Solved Question Paper 2010Document34 pagesAIIMS (MBBS) Solved Question Paper 2010cbsestudymaterialsNo ratings yet
- Adobe Scan 13 May 2021Document5 pagesAdobe Scan 13 May 2021Harisree SNo ratings yet
- Diabetic Ketoacidosis (DKA) VS. Hyperosmolar Hyperglycemic Syndrome (HHS)Document5 pagesDiabetic Ketoacidosis (DKA) VS. Hyperosmolar Hyperglycemic Syndrome (HHS)MrRightNo ratings yet