You might also like
- Diuretics 140628134114 Phpapp02Document45 pagesDiuretics 140628134114 Phpapp02P merugu100% (1)
- DiureticsDocument40 pagesDiureticsHarri HardiNo ratings yet
- Vidconf Diuretic Antidiuretic 2014Document51 pagesVidconf Diuretic Antidiuretic 2014naltrisilvianNo ratings yet
- The Heart and Circulatory System and The Kidney 2Document28 pagesThe Heart and Circulatory System and The Kidney 2Izzuddin AhmadNo ratings yet
- Diuretic DrugsDocument62 pagesDiuretic DrugsAbdul WahabNo ratings yet
- Ph'cology of Diuretics (RZH)Document48 pagesPh'cology of Diuretics (RZH)beby febyola siagianNo ratings yet
- Diuretic Agents: Dept. of Pharmacology & TherapeuticDocument44 pagesDiuretic Agents: Dept. of Pharmacology & Therapeuticangelica gloryNo ratings yet
- Pharmacology I, Diuretics NK-modified 2Document32 pagesPharmacology I, Diuretics NK-modified 289c8g7bvvvNo ratings yet
- Chapter 3 CVS & RenalDocument116 pagesChapter 3 CVS & RenalKIDUS YAREDNo ratings yet
- Pharmacology of Diuretics: DR - Datten Bangun MSC, SPFKDocument46 pagesPharmacology of Diuretics: DR - Datten Bangun MSC, SPFKRizky Pramata Simamora 19000029No ratings yet
- Diuretics NewDocument21 pagesDiuretics NewPawan RajNo ratings yet
- diuretics (2)Document58 pagesdiuretics (2)abenezergebrekirstosNo ratings yet
- Renal Drugs Diuretics Agents: by Desalegn Chilo (B.Pharm, MSC)Document54 pagesRenal Drugs Diuretics Agents: by Desalegn Chilo (B.Pharm, MSC)Remedan TahaNo ratings yet
- Diuretics: DR Sindwa KanyimbaDocument43 pagesDiuretics: DR Sindwa Kanyimbaedward kaumbaNo ratings yet
- Diuretics MergedDocument727 pagesDiuretics MergedRinkiNo ratings yet
- Lecture 9Document14 pagesLecture 9Aan KurniawanNo ratings yet
- DiureticsDocument29 pagesDiureticsdeepak askarNo ratings yet
- Diuretics: Diuretics Are Drugs That Increase The Volume of Urine FlowDocument35 pagesDiuretics: Diuretics Are Drugs That Increase The Volume of Urine FlowAmanuel Maru100% (1)
- DiureticsDocument10 pagesDiureticsSantosh RoyNo ratings yet
- Drugs Affecting Renal SystemDocument44 pagesDrugs Affecting Renal SystemRwapembe StephenNo ratings yet
- UntitledDocument59 pagesUntitledSafayet HossainNo ratings yet
- Diuretic Drugs: Thiazides Sites of ActionDocument52 pagesDiuretic Drugs: Thiazides Sites of Actionuzzal ahmedNo ratings yet
- Farmakoterapi Sistem RenalDocument89 pagesFarmakoterapi Sistem RenalNhovieNhowaaNo ratings yet
- Diuretics: BY-DR. Saurabh Kansal Dept. of Pharmacology Msy Medical College MeerutDocument33 pagesDiuretics: BY-DR. Saurabh Kansal Dept. of Pharmacology Msy Medical College MeerutPrakhar GoelNo ratings yet
- DiureticsDocument16 pagesDiureticsDr. PARMINDER NAINNo ratings yet
- Diuretics: Types, Mechanisms and Clinical UsesDocument43 pagesDiuretics: Types, Mechanisms and Clinical UsesAmanuel MaruNo ratings yet
- Diuretics: Pranjal Wagh Master of Pharmacy (2021-2023) Poona College of PharmacyDocument39 pagesDiuretics: Pranjal Wagh Master of Pharmacy (2021-2023) Poona College of PharmacyPranjalNo ratings yet
- Diuretic DrugsDocument2 pagesDiuretic DrugsEngku ElisaNo ratings yet
- Diuretics: Basic Pharmacology Block Pdnt/Pmed - PMSC/PPHR - 213Document19 pagesDiuretics: Basic Pharmacology Block Pdnt/Pmed - PMSC/PPHR - 213JedoNo ratings yet
- Diuretics and Anti Diuretics: Year Iii Pharm.D Dr. V. ChitraDocument49 pagesDiuretics and Anti Diuretics: Year Iii Pharm.D Dr. V. ChitranikithaNo ratings yet
- Diuretics and Their Mechanism of Action in the NephronDocument52 pagesDiuretics and Their Mechanism of Action in the NephronKulgaurav RegmiNo ratings yet
- Effects and mechanisms of diuretics in the kidneyDocument34 pagesEffects and mechanisms of diuretics in the kidneyJosephine SNo ratings yet
- DiureticsDocument83 pagesDiureticsKarami BrutusNo ratings yet
- PDF DiureticsDocument20 pagesPDF DiureticsIhjas HabeebNo ratings yet
- Introducton Renal Physiolgy: Physiology Department Medical School, University of Methodist IndonesiaDocument47 pagesIntroducton Renal Physiolgy: Physiology Department Medical School, University of Methodist IndonesiaHachi Nini Shop II100% (1)
- DIURETICS LECTURE ZebDocument52 pagesDIURETICS LECTURE ZebPROF DR SHAHMURAD100% (2)
- Obat-Obat KardiovaskulerDocument50 pagesObat-Obat KardiovaskulerMuhammad IqbalNo ratings yet
- DIURETICSDocument55 pagesDIURETICSRAVISHNo ratings yet
- CVS - DiureticsDocument8 pagesCVS - Diureticshlouis8No ratings yet
- DR Yosra Diuretics 2023Document46 pagesDR Yosra Diuretics 2023gntawfeqNo ratings yet
- DR - Datten Bangun MSC, SPFK: Dept - Farmakologi & Therapeutik Fak - Kedokteran UhnDocument39 pagesDR - Datten Bangun MSC, SPFK: Dept - Farmakologi & Therapeutik Fak - Kedokteran UhnTeus FatamorganaNo ratings yet
- Classification of Antihypertensive Drugs: DiureticsDocument36 pagesClassification of Antihypertensive Drugs: DiureticsArvi KhanNo ratings yet
- Diuretics 1Document34 pagesDiuretics 1ياسمين مجديNo ratings yet
- DIURETICSDocument25 pagesDIURETICSHUZAIFA YAMAANNo ratings yet
- 5 RenalDocument10 pages5 RenalAli EllaffiNo ratings yet
- DiureticsDocument12 pagesDiureticslandita683No ratings yet
- 6.1. AntihipertensiDocument52 pages6.1. AntihipertensiDada DoniNo ratings yet
- Diuretic DrugsDocument16 pagesDiuretic DrugslabillabooNo ratings yet
- DIURETICSDocument39 pagesDIURETICSFrancisNo ratings yet
- Diuretics: Sumolly Anak DavidDocument29 pagesDiuretics: Sumolly Anak Davidfarmasi_hmNo ratings yet
- 15 Diuretic AgentsDocument50 pages15 Diuretic AgentsAngelyn Si100% (1)
- Diuretics AaupDocument25 pagesDiuretics AaupSabrina ShalhoutNo ratings yet
- DiureticsDocument61 pagesDiureticsJoyce WacukaNo ratings yet
- Diuretics - AMBOSS PDFDocument9 pagesDiuretics - AMBOSS PDFOpio Isaac100% (1)
- DiureticsDocument28 pagesDiureticsAnkita TatheNo ratings yet
- Cardiovascular For PharmacologDocument134 pagesCardiovascular For Pharmacologephremtigabie7No ratings yet
- Diuretics: Haitham Mahmood AlwaliDocument32 pagesDiuretics: Haitham Mahmood Alwaligaurav adhikariNo ratings yet
- c15 Diuretic AgentsDocument13 pagesc15 Diuretic AgentsmohammadNo ratings yet
- Diuretics: A. Overview of The Clinical Use of Diuretics B. Classification of DiureticsDocument22 pagesDiuretics: A. Overview of The Clinical Use of Diuretics B. Classification of DiureticsSteven GonzalesNo ratings yet
- DM3xxx Accessory List LeafletDocument2 pagesDM3xxx Accessory List LeafletAdvantec SrlNo ratings yet
- Pres. Quirino Treasured Child School, Inc.: Grade 8-St. Joseph & ST MatthewDocument2 pagesPres. Quirino Treasured Child School, Inc.: Grade 8-St. Joseph & ST MatthewChristian jade QuijanoNo ratings yet
- Impex Kitchen Appliances PDFDocument4 pagesImpex Kitchen Appliances PDFqwqw11No ratings yet
- Engineering Services for Abadan Petrochemical Plant VCM Unloading Station Piping DesignDocument28 pagesEngineering Services for Abadan Petrochemical Plant VCM Unloading Station Piping DesignMehdi NouriNo ratings yet
- API Calcs Rev1 (Version 2)Document112 pagesAPI Calcs Rev1 (Version 2)Jake Sparrow100% (1)
- Oxford SuprEsser ManualDocument34 pagesOxford SuprEsser ManualaaaNo ratings yet
- About Softprom by ERCDocument26 pagesAbout Softprom by ERCMaryna KuryshchenkoNo ratings yet
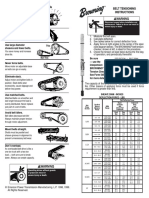
- Browning Belt Tension GaugeDocument2 pagesBrowning Belt Tension GaugeJasperken2xNo ratings yet
- 22 Imobilisasi Pada Usia LanjutDocument34 pages22 Imobilisasi Pada Usia LanjutGian KalalembangNo ratings yet
- Worthy - Elevation WorshipDocument1 pageWorthy - Elevation WorshipSabine J.100% (1)
- Fesh S A0001171549 1Document7 pagesFesh S A0001171549 1ismuNo ratings yet
- LUKAS Product Information-2Document2 pagesLUKAS Product Information-2Flavian ZfmNo ratings yet
- Labcelldivision ErikagutierrezDocument10 pagesLabcelldivision Erikagutierrezapi-336047220No ratings yet
- Rites of Acceptance For Altar Servers PDFDocument3 pagesRites of Acceptance For Altar Servers PDFJohn Carl Aparicio100% (1)
- Actual Freedom - Made Easy (Print Friendly Edition)Document186 pagesActual Freedom - Made Easy (Print Friendly Edition)Justine100% (5)
- Regulation 1 Regulation 2 Regulation 3 Regulation 4 Regulation 5 Regulation 6 Regulation 7 Regulation 8 Regulation 9 AppendixDocument10 pagesRegulation 1 Regulation 2 Regulation 3 Regulation 4 Regulation 5 Regulation 6 Regulation 7 Regulation 8 Regulation 9 AppendixAnonymous 7gJ9alpNo ratings yet
- MODULE-2-VETTECH325 (2)Document31 pagesMODULE-2-VETTECH325 (2)cejproiloNo ratings yet
- Kant On Religion and ScienceDocument21 pagesKant On Religion and ScienceEduardo CharpenelNo ratings yet
- Science: Pure Substances Vs MixturesDocument33 pagesScience: Pure Substances Vs MixturesElle Ma Rie100% (1)
- Figure of SpeechDocument27 pagesFigure of SpeechSabel Ross CaliliwNo ratings yet
- BARACARBDocument2 pagesBARACARBYudha Satria50% (2)
- Jacobi Progressive Speed Agility Training For High School Middle School AthletesDocument39 pagesJacobi Progressive Speed Agility Training For High School Middle School AthletesAnthony Mckay100% (1)
- Flange Insulation Sets: Technical SpecificationDocument6 pagesFlange Insulation Sets: Technical SpecificationNor Azlan AwangNo ratings yet
- Changing Landscape and Ecotourism Development in A Large Dam SiteDocument16 pagesChanging Landscape and Ecotourism Development in A Large Dam Siteವಿನಯ್ ಎಮ್. ಆರ್No ratings yet
- SilverDocument16 pagesSilversharma_shruti0% (1)
- Chapter 1 and 2Document67 pagesChapter 1 and 2Tle SupawidNo ratings yet
- PAForge D20 Weapons CompendiumDocument29 pagesPAForge D20 Weapons Compendiumdjbonefish100% (1)
- Quarter 1-Module 2 Modern ArtDocument20 pagesQuarter 1-Module 2 Modern ArtKimberly Trocio Kim100% (1)
- Growth, Stagnation or Decline? Agfficulturalproductm'Iy in British IndiaDocument290 pagesGrowth, Stagnation or Decline? Agfficulturalproductm'Iy in British IndiaHarshadeep BiswasNo ratings yet
- Heliflex Hose CatalogueDocument119 pagesHeliflex Hose CatalogueAugustine DharmarajNo ratings yet