You might also like
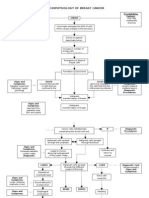
- Pathophysiology of Breast Cancer: Unkno Predisposing Factors: Precipitating FactorsDocument3 pagesPathophysiology of Breast Cancer: Unkno Predisposing Factors: Precipitating FactorsKevin Ercia100% (1)
- Pathophysiology Diagram: Breast Cancer: Predisposing Factors: Precipitating FactorsDocument2 pagesPathophysiology Diagram: Breast Cancer: Predisposing Factors: Precipitating FactorsMarinill Soliman100% (1)
- NCM 104 Cellular Aberration Lecture 2007Document104 pagesNCM 104 Cellular Aberration Lecture 2007api-378278992% (26)
- Thyroid CancerDocument5 pagesThyroid CancerZed P. EstalillaNo ratings yet
- Five Tips To Prevent Dog Bites PosterDocument1 pageFive Tips To Prevent Dog Bites PosterRama BiomantaraNo ratings yet
- Gastroenterology Medical Records SampleDocument1 pageGastroenterology Medical Records SampleMarisol Jane JomayaNo ratings yet
- NCM 104 Cellular Aberration Lecture 2007Document104 pagesNCM 104 Cellular Aberration Lecture 2007Kris TejereroNo ratings yet
- Understanding Cancer: Jasmin Saragena BetinolDocument104 pagesUnderstanding Cancer: Jasmin Saragena BetinolERAN MARK ROJASNo ratings yet
- Benign Malignant: Malignant Transformation: Retrovirus (RNA Virus)Document3 pagesBenign Malignant: Malignant Transformation: Retrovirus (RNA Virus)ChiNo ratings yet
- NCM 109 Cellular AbberationsDocument17 pagesNCM 109 Cellular AbberationsSittie Haneen Tabara100% (1)
- Cellular Aberrations Cancer, Malignant Neoplasm, Oncologic DisorderDocument5 pagesCellular Aberrations Cancer, Malignant Neoplasm, Oncologic DisorderIrish Eunice Felix100% (1)
- Neoplasm ADocument46 pagesNeoplasm ANur FaidahNo ratings yet
- Pathology of Neoplasia Cancer Malignant Benign Carcinoma Lecture PDFDocument8 pagesPathology of Neoplasia Cancer Malignant Benign Carcinoma Lecture PDFjax111No ratings yet
- Molecular Basis of Cancer:: Carcinogenesis & Regulator GenesDocument52 pagesMolecular Basis of Cancer:: Carcinogenesis & Regulator GenesFenny Cienta Damai ClaluNo ratings yet
- Neoplasia IIDocument44 pagesNeoplasia IIJeevan SunaNo ratings yet
- Medical SurgicalDocument42 pagesMedical SurgicaltabiNo ratings yet
- Cancer: By: Carolina Vidal, RNDocument49 pagesCancer: By: Carolina Vidal, RNCarolina VidalNo ratings yet
- Chemotherapy AgentsDocument12 pagesChemotherapy Agentsaaliyah frances habawelNo ratings yet
- Cancer Hallmark 1 (From Jargonwall - Com)Document9 pagesCancer Hallmark 1 (From Jargonwall - Com)eihimekpen02No ratings yet
- Netic Cancer Sem Jan 2022Document66 pagesNetic Cancer Sem Jan 2022AIMAN MUHAIMMIN HASNANNo ratings yet
- Prof. Dr. Ghada Helaly - (5) Introduction To Oncoviruses.Document23 pagesProf. Dr. Ghada Helaly - (5) Introduction To Oncoviruses.زهوة أحمد البازNo ratings yet
- Neoplasia and Cancer: Week 1Document8 pagesNeoplasia and Cancer: Week 1rise wiiinNo ratings yet
- Oncologic Nursing: Oncology: OverviewDocument156 pagesOncologic Nursing: Oncology: OverviewNathalie KerrNo ratings yet
- 1 Tumorigenesis, Mutasi, Ketidakstabilan GenetikDocument44 pages1 Tumorigenesis, Mutasi, Ketidakstabilan Genetikanon_945728920No ratings yet
- 4 - Malignant 2023Document62 pages4 - Malignant 2023drsafwatismailNo ratings yet
- Cellular Abberration Transes Lesson 1-3Document10 pagesCellular Abberration Transes Lesson 1-3RHEA ROSE GACHONo ratings yet
- Part2 OncologyDocument39 pagesPart2 OncologySamah AlshamiNo ratings yet
- Understanding CancerDocument5 pagesUnderstanding CancerEunice Villa CuñadaNo ratings yet
- Carcinogenesis (Neoplasm 2)Document84 pagesCarcinogenesis (Neoplasm 2)andialifpratama21No ratings yet
- An Introduction To Cancer Biology: When Good Cells Go BadDocument68 pagesAn Introduction To Cancer Biology: When Good Cells Go BadSavitaNo ratings yet
- Cancer Genetics Final 1Document44 pagesCancer Genetics Final 1Celestine MarivelezNo ratings yet
- Part 1 Student NCM 112 Oncology NotesDocument12 pagesPart 1 Student NCM 112 Oncology NotesJohn Kenley FerryNo ratings yet
- CA RevisedDocument19 pagesCA RevisedmarkyboiNo ratings yet
- Cancer NotesDocument7 pagesCancer NotesKyla Mae JumaritoNo ratings yet
- Neoplasm LectureDocument23 pagesNeoplasm LectureRianNo ratings yet
- Pathology Of: NeoplasiaDocument23 pagesPathology Of: NeoplasiaBryan de GuzmanNo ratings yet
- Neoplasia Summer 2020Document38 pagesNeoplasia Summer 2020Sharif HossainNo ratings yet
- 4 - HPV Infection and Vaccination - PaoloBonanniDocument99 pages4 - HPV Infection and Vaccination - PaoloBonanniqNo ratings yet
- Oncology AssignmentDocument18 pagesOncology AssignmentAngeline EspinasNo ratings yet
- NEOPLASIA ExpDocument17 pagesNEOPLASIA ExpYuris AriasNo ratings yet
- Radial N. Innervates The BEST!!!! Brachioradialis Extensors Supinator TricepsDocument57 pagesRadial N. Innervates The BEST!!!! Brachioradialis Extensors Supinator TricepsdrsilkNo ratings yet
- Biological Carcinogens: Infectious Cacrinogenesis BasicsDocument5 pagesBiological Carcinogens: Infectious Cacrinogenesis BasicsNalumenya MathewNo ratings yet
- Materi DR SuzanDocument26 pagesMateri DR SuzanputrihealthirezaNo ratings yet
- CancerDocument14 pagesCancerlove.mansijhaNo ratings yet
- Oncology NursingDocument3 pagesOncology NursingJalishia Mae DumdumaNo ratings yet
- Cancer Ms LecDocument16 pagesCancer Ms LecJulia Rae Delos Santos100% (1)
- Ch7 NeoplasmDocument96 pagesCh7 Neoplasmmormor80No ratings yet
- Cervic Tumour - SummaryDocument9 pagesCervic Tumour - SummaryRUDOLF YUSON BM20110052No ratings yet
- Neoplasia Lect. IV: Department Of: HereDocument19 pagesNeoplasia Lect. IV: Department Of: Herezeena abdulhuseinNo ratings yet
- Biokimia Blok NeoplasiaDocument65 pagesBiokimia Blok NeoplasiafaisalNo ratings yet
- Neoplasia OutlineDocument3 pagesNeoplasia OutlineQuazi Akif TahmidNo ratings yet
- Screenshot 2023-03-01 at 3.14.03 PMDocument17 pagesScreenshot 2023-03-01 at 3.14.03 PMmohameeedar1No ratings yet
- Pathophysiology of Transitional Cell CarcinomaDocument10 pagesPathophysiology of Transitional Cell CarcinomaJheanAlphonsineT.MeansNo ratings yet
- Cancer Pathophysiology: Radhika D Prabhu MS124129Document43 pagesCancer Pathophysiology: Radhika D Prabhu MS124129Radhika PrabhuNo ratings yet
- 212F - Oncology L1 - 2104Document25 pages212F - Oncology L1 - 2104Tyler LiuNo ratings yet
- TOXICOLOGY SemisDocument4 pagesTOXICOLOGY Semisppalalon96997No ratings yet
- The Natural History of Human Papillomavirus InfectionDocument12 pagesThe Natural History of Human Papillomavirus InfectionValentina GarciaNo ratings yet
- Oncology Nursing Oncology What Is Cancer?Document10 pagesOncology Nursing Oncology What Is Cancer?NeweeJoonYow100% (1)
- CarcinogenesisDocument40 pagesCarcinogenesisNatasha AmaldaNo ratings yet
- Oncology: Farrahiyah IsmailDocument33 pagesOncology: Farrahiyah IsmailaisyahambaliNo ratings yet
- Oncogenesis Topic by Laraib FiazDocument23 pagesOncogenesis Topic by Laraib FiazLaraib FiazNo ratings yet
- Aedes Aegypti Wolbachia: Limited Dengue Virus Replication in Field-Collected Mosquitoes Infected WithDocument10 pagesAedes Aegypti Wolbachia: Limited Dengue Virus Replication in Field-Collected Mosquitoes Infected WithRama BiomantaraNo ratings yet
- 1 IntroDocument62 pages1 IntroRama BiomantaraNo ratings yet
- Loperamide: Article OutlineDocument10 pagesLoperamide: Article OutlineRama Biomantara0% (1)
- Surgical Outcome Results From SWOG S1505: Asa PDocument6 pagesSurgical Outcome Results From SWOG S1505: Asa PElianaNo ratings yet
- Clinical Significance of Primary Debulking Surgery and Neoadjuvant Chemotherapy-Interval Debulking Surgery in Advanced Ovarian Cancer. 2020Document8 pagesClinical Significance of Primary Debulking Surgery and Neoadjuvant Chemotherapy-Interval Debulking Surgery in Advanced Ovarian Cancer. 2020Prodromos KoutoukoglouNo ratings yet
- Uterine SarcomaDocument44 pagesUterine SarcomajojolilimomoNo ratings yet
- How Infectious Diseases Cause CancerDocument47 pagesHow Infectious Diseases Cause CancerRizki RakhmandaNo ratings yet
- HPV Test in Cervical Cancer ScreeningDocument25 pagesHPV Test in Cervical Cancer Screeningatha nafeezaNo ratings yet
- ASCO Educational Book 2021Document773 pagesASCO Educational Book 2021Sally Paredes NoguniNo ratings yet
- Newest Cervical CancerDocument14 pagesNewest Cervical CancerSAMMYNo ratings yet
- BJUI Compass - 2021 - Ory - Outcomes of Organ Sparing Surgery For Adult Testicular Tumors A Systematic Review of TheDocument16 pagesBJUI Compass - 2021 - Ory - Outcomes of Organ Sparing Surgery For Adult Testicular Tumors A Systematic Review of TheSeb TckNo ratings yet
- Pembrolizumab For Persistent, Recurrent, or Metastatic Carvical CancerDocument12 pagesPembrolizumab For Persistent, Recurrent, or Metastatic Carvical CancerluizaNo ratings yet
- Stadium CA LaringDocument4 pagesStadium CA LaringmunzirNo ratings yet
- 10.1038@s41572-018-0055-Y FisiopatologiaDocument26 pages10.1038@s41572-018-0055-Y FisiopatologiaJESUS GABRIEL RAMIREZ ESCALANTENo ratings yet
- Thesis Statement For Breast Cancer Paper PDFDocument6 pagesThesis Statement For Breast Cancer Paper PDFgcq5c1pv100% (1)
- Vadina 1Document38 pagesVadina 1api-3702141No ratings yet
- Datta 2016Document5 pagesDatta 2016faris nagibNo ratings yet
- TumorDocument8 pagesTumorputyCeria86No ratings yet
- Diagnosis and Management of Squamous Cell Carcinoma of Unknown Primary in The Head and Neck - ASCO GuidelineDocument29 pagesDiagnosis and Management of Squamous Cell Carcinoma of Unknown Primary in The Head and Neck - ASCO GuidelineFabian Camelo OtorrinoNo ratings yet
- Seren Award Masterclass 2Document13 pagesSeren Award Masterclass 2Angelika LauNo ratings yet
- Drug Study BevacizumabDocument1 pageDrug Study BevacizumabBARRISTERFLOWERSEAURCHIN6No ratings yet
- Retrospective Diagnosis of Malignant Struma Ovarii After Discovery of PulmonaryDocument17 pagesRetrospective Diagnosis of Malignant Struma Ovarii After Discovery of PulmonaryGeorge LazarNo ratings yet
- Curriculum Vitae Dr. Ari AstramDocument4 pagesCurriculum Vitae Dr. Ari AstramBedah ManadoNo ratings yet
- Malignant Proliferating Trichilemmal Tumor One Case and Literature ReviewDocument4 pagesMalignant Proliferating Trichilemmal Tumor One Case and Literature ReviewIJAR JOURNALNo ratings yet
- 19-109 Putri Amalia CSS Radiologi PDFDocument20 pages19-109 Putri Amalia CSS Radiologi PDFPutri AmaliaNo ratings yet
- BreastCalcifications PDFDocument2 pagesBreastCalcifications PDFmoeNo ratings yet
- Biliary Tract Cancers: NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines)Document96 pagesBiliary Tract Cancers: NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines)Sabbir RaihanNo ratings yet
- Breast Cancer SurgeryDocument6 pagesBreast Cancer SurgeryΔρ Βαιος ΑγγελοπουλοςNo ratings yet
- Day 2Document1 pageDay 2Minerva Medical Treatment Pvt LtdNo ratings yet
- Care of Clients With Cellular Aberrations: NCM 106/ NCM 112Document22 pagesCare of Clients With Cellular Aberrations: NCM 106/ NCM 112Janelle Cabida SupnadNo ratings yet
- Case Presentation: DR Tariq Masood TMO Radiology Department, HMCDocument82 pagesCase Presentation: DR Tariq Masood TMO Radiology Department, HMCg1381821No ratings yet
- Dennis Slamon Ribociclib Plus Endocrine Therapy inDocument12 pagesDennis Slamon Ribociclib Plus Endocrine Therapy inandre.manzanoqNo ratings yet