You might also like
- 10 1067@j Cpradiol 2009 07 005 PDFDocument19 pages10 1067@j Cpradiol 2009 07 005 PDFJess LejardeNo ratings yet
- Carotid Artery Stenosis ImagingDocument10 pagesCarotid Artery Stenosis ImagingCristhian RuizNo ratings yet
- Anomalous Coronary ArteriesDocument7 pagesAnomalous Coronary ArteriesYonatan Merchant PerezNo ratings yet
- AR 12 06 CTA BudoffDocument8 pagesAR 12 06 CTA BudoffYonatan Merchant PerezNo ratings yet
- Eajm 42 2 100Document3 pagesEajm 42 2 100Diana BanceuNo ratings yet
- CVM 2018 00540Document9 pagesCVM 2018 00540Seanglaw SituNo ratings yet
- Angiography of The Coronary ArteriesDocument14 pagesAngiography of The Coronary ArteriesYonatan Merchant PerezNo ratings yet
- Coronary CTA ReviewDocument4 pagesCoronary CTA ReviewRedhwan Abdullah qaid AlshubiNo ratings yet
- Using The 12-Lead ECG To Localize The Origin of Atrial and Ventricular Tachycardias. Part 2-Ventricular TachycardiaDocument9 pagesUsing The 12-Lead ECG To Localize The Origin of Atrial and Ventricular Tachycardias. Part 2-Ventricular Tachycardiarentedmule00No ratings yet
- Coronary Artery Anomalies: Thomas Knickelbine, Michael Bolooki, and Zeev VlodaverDocument33 pagesCoronary Artery Anomalies: Thomas Knickelbine, Michael Bolooki, and Zeev VlodaverIboy ZulhamNo ratings yet
- Cardiac CT: Specializing in Cardiac CTDocument9 pagesCardiac CT: Specializing in Cardiac CTAshvanee sharmaNo ratings yet
- Unenhanced MR Angiography: Martin Backens and Bernd SchmitzDocument20 pagesUnenhanced MR Angiography: Martin Backens and Bernd SchmitzEka Setyorini .A.No ratings yet
- Samol2012 PDFDocument8 pagesSamol2012 PDFnaniro orinanNo ratings yet
- Chest CT Angiography For Acute Aortic Pathologic Conditions: Pearls and PitfallsDocument26 pagesChest CT Angiography For Acute Aortic Pathologic Conditions: Pearls and PitfallsJelvis BofNo ratings yet
- Diagnoses SDocument25 pagesDiagnoses STudor DumitrascuNo ratings yet
- Intracranial Vascular Lesionsand Anatomical Variants All Residents Should KnowDocument20 pagesIntracranial Vascular Lesionsand Anatomical Variants All Residents Should Knowcrisvbarros8865No ratings yet
- Jurnal 14Document9 pagesJurnal 14Zella ZakyaNo ratings yet
- Claus 2015Document17 pagesClaus 2015Dr. Muha. Hasan Mahbub-Ur-RahmanNo ratings yet
- Subarachnoid Hemorrhage: Beyond Aneurysm: How To Manage?Document24 pagesSubarachnoid Hemorrhage: Beyond Aneurysm: How To Manage?heruNo ratings yet
- The Human Coronary Collateral Circulation: Christian SeilerDocument6 pagesThe Human Coronary Collateral Circulation: Christian Seilerabdeta gebreNo ratings yet
- Ultrasound Evaluation of Renal Artery StenosisDocument19 pagesUltrasound Evaluation of Renal Artery Stenosisroentgen169100% (1)
- Dca RahulDocument72 pagesDca RahulyuliaNo ratings yet
- Basic Cardiac ImagingDocument40 pagesBasic Cardiac ImagingSarah Sy-SantosNo ratings yet
- Crite RiosDocument8 pagesCrite RiosNilson Morales CordobaNo ratings yet
- Role of MDCT in Coronary Artery Disease: Swachchhanda Songmen 2071Document63 pagesRole of MDCT in Coronary Artery Disease: Swachchhanda Songmen 2071Dr KhanNo ratings yet
- Pulmonary ArtesiaDocument6 pagesPulmonary ArtesiaMaulani NurlatifahNo ratings yet
- Imaging of Traumatic Intracranial HemorrhageDocument8 pagesImaging of Traumatic Intracranial HemorrhageSariRahmaYentiNo ratings yet
- Cardiac AnatomyDocument17 pagesCardiac AnatomyAndreas Erick HaurissaNo ratings yet
- Computed Tomography Coronary A-2Document9 pagesComputed Tomography Coronary A-2ganda gandaNo ratings yet
- Determinación de La Importancia Del Flujo Inverso en La Arteria Carótida InternaDocument3 pagesDeterminación de La Importancia Del Flujo Inverso en La Arteria Carótida InternaJosè Julio Cejas SànchezNo ratings yet
- 2019 Pitfalls in Cardiac CTDocument8 pages2019 Pitfalls in Cardiac CTsabaxlentNo ratings yet
- Circep 119 008210Document12 pagesCircep 119 008210Paul CalbureanNo ratings yet
- 347 FullDocument7 pages347 FulldediNo ratings yet
- Assessment of Left Ventricular Myocardial Diseases With Cardiac Computed TomographyDocument19 pagesAssessment of Left Ventricular Myocardial Diseases With Cardiac Computed Tomographysyifa auliaNo ratings yet
- Broad Complex TachyDocument8 pagesBroad Complex TachyarnabNo ratings yet
- Carotid-Cavernous Fistula Imaging - Practice Essentials, Computed Tomography, Magnetic Resonance ImagingDocument7 pagesCarotid-Cavernous Fistula Imaging - Practice Essentials, Computed Tomography, Magnetic Resonance ImagingClarithq LengguNo ratings yet
- Coronary Artery AnatomyDocument10 pagesCoronary Artery Anatomy徐振瑋No ratings yet
- Coronary Artery Plaque Characteristics Associated With Adverse Outcomes in The SCOT-HEART StudyDocument11 pagesCoronary Artery Plaque Characteristics Associated With Adverse Outcomes in The SCOT-HEART StudySTOCARE DATENo ratings yet
- Stirrup - Comparison of ESC and ACC:AHA Guidelines For Myocardial RevascularizationDocument8 pagesStirrup - Comparison of ESC and ACC:AHA Guidelines For Myocardial RevascularizationM. PurnomoNo ratings yet
- Ryct 2021200378Document14 pagesRyct 2021200378Vimal NishadNo ratings yet
- 5.RCA or LCX in Inferior MIDocument7 pages5.RCA or LCX in Inferior MIAshraf ChowdhuryNo ratings yet
- Criss-Cross Heart With Double-Outlet Right VentricleDocument4 pagesCriss-Cross Heart With Double-Outlet Right Ventriclejuana lopezNo ratings yet
- Recommendations For Accurate CT Diagnosis of SuspeDocument10 pagesRecommendations For Accurate CT Diagnosis of SuspeallthewayhomeNo ratings yet
- Vainikiniø Arterijø Ávertinimo DaugiapjûviuDocument74 pagesVainikiniø Arterijø Ávertinimo DaugiapjûviuneringajakaityteNo ratings yet
- VT in CAD PDFDocument10 pagesVT in CAD PDFTor JaNo ratings yet
- Journal of Electrocardiology: ArticleinfoDocument6 pagesJournal of Electrocardiology: ArticleinfoVlada SiricNo ratings yet
- Revchilanestv 5007101119Document4 pagesRevchilanestv 5007101119Javier HdezNo ratings yet
- Coronary 23716Document32 pagesCoronary 23716Luis David Sanchez MayoNo ratings yet
- Imaging Stroke in MinutesDocument23 pagesImaging Stroke in MinutesAnonymous iea4m0ZRNo ratings yet
- RRC Art-1aqDocument12 pagesRRC Art-1aqCristi AlexandruNo ratings yet
- Cardiac Imaging and BiomarkersDocument23 pagesCardiac Imaging and BiomarkersShreyas NayakNo ratings yet
- Cerebrovascular DiseaseDocument3 pagesCerebrovascular DiseaseLourdes VillelaNo ratings yet
- Cardio Vascular PDFDocument148 pagesCardio Vascular PDFStefana RoxanaNo ratings yet
- Ghid Aplicatii Clinice Ale CT Cardiac Partea 1 2022Document16 pagesGhid Aplicatii Clinice Ale CT Cardiac Partea 1 2022Anca LunguNo ratings yet
- Joint Segmentation and Classification of Retinal Arteries/Veins From Fundus ImagesDocument15 pagesJoint Segmentation and Classification of Retinal Arteries/Veins From Fundus Imageszj xiaoNo ratings yet
- Conexinas y Nodo AV. Heart Rhythm 2013Document8 pagesConexinas y Nodo AV. Heart Rhythm 2013Ernesto J. Rocha ReyesNo ratings yet
- Porcelain AortaDocument10 pagesPorcelain AortaomarfaridtawfikNo ratings yet
- Essential Cardiac Electrophysiology: The Self-Assessment ApproachFrom EverandEssential Cardiac Electrophysiology: The Self-Assessment ApproachNo ratings yet
- Journal Reading Anestesi RianDocument21 pagesJournal Reading Anestesi RianRian AprizaNo ratings yet
- Accepted Manuscript: Journal of Cardiothoracic and Vascular AnesthesiaDocument27 pagesAccepted Manuscript: Journal of Cardiothoracic and Vascular AnesthesiaRian AprizaNo ratings yet
- 10 1053@j Jvca 2019 01 039Document152 pages10 1053@j Jvca 2019 01 039Rian AprizaNo ratings yet
- 10 1053@j Jvca 2019 01 039Document152 pages10 1053@j Jvca 2019 01 039Rian AprizaNo ratings yet
- Inhaled streptokinase improves oxygenation in severe ARDSDocument28 pagesInhaled streptokinase improves oxygenation in severe ARDSRian AprizaNo ratings yet
- Bartos Z Ko 2018Document9 pagesBartos Z Ko 2018Rian AprizaNo ratings yet
- Norepinephrine Infusion For Preventing Postspinal Anesthesia Hypotension During Cesarean DeliveryDocument8 pagesNorepinephrine Infusion For Preventing Postspinal Anesthesia Hypotension During Cesarean DeliveryRian AprizaNo ratings yet
- Bartoszko 2018Document9 pagesBartoszko 2018Rian AprizaNo ratings yet
- Pi Is 0002934314009073Document7 pagesPi Is 0002934314009073Rian AprizaNo ratings yet
- JR Cvcu RianDocument16 pagesJR Cvcu RianRian AprizaNo ratings yet
- 12 - 265berita Terkini-Manfaat DAPT Aspirin Dan Clopidogrel Sebagai Pengganti Aspirin Dan TicagrelorDocument8 pages12 - 265berita Terkini-Manfaat DAPT Aspirin Dan Clopidogrel Sebagai Pengganti Aspirin Dan TicagrelorAmelNo ratings yet
- Dr. Rian Apriza Pembimbing: DR - Hilfan Ade Putra Lubis, SPJP (K)Document25 pagesDr. Rian Apriza Pembimbing: DR - Hilfan Ade Putra Lubis, SPJP (K)Rian AprizaNo ratings yet
- Inhaled streptokinase improves oxygenation in severe ARDSDocument28 pagesInhaled streptokinase improves oxygenation in severe ARDSRian AprizaNo ratings yet
- Accepted Manuscript: Journal of Cardiothoracic and Vascular AnesthesiaDocument27 pagesAccepted Manuscript: Journal of Cardiothoracic and Vascular AnesthesiaRian AprizaNo ratings yet
- JR Integrasi InvasiveDocument72 pagesJR Integrasi InvasiveRian AprizaNo ratings yet
- Norepinephrine Infusion For Preventing Postspinal Anesthesia Hypotension During Cesarean DeliveryDocument8 pagesNorepinephrine Infusion For Preventing Postspinal Anesthesia Hypotension During Cesarean DeliveryRian AprizaNo ratings yet
- Husebye 2017Document9 pagesHusebye 2017Rian AprizaNo ratings yet
- T J M P: HE EAN Onnet RogramDocument80 pagesT J M P: HE EAN Onnet RogramRian AprizaNo ratings yet
- Who Reccomendation MalnutritionDocument123 pagesWho Reccomendation MalnutritionAgaipNo ratings yet
- Circinterventions 117 005528Document10 pagesCircinterventions 117 005528Rian AprizaNo ratings yet
- IMAM Guidelines Final VersionDocument137 pagesIMAM Guidelines Final VersionRian Apriza0% (1)
- PreventionDocument3 pagesPreventionRian AprizaNo ratings yet
- BAP Sleep GuidelinesDocument25 pagesBAP Sleep GuidelinesRian AprizaNo ratings yet
- InsomniaDocument4 pagesInsomniaCatalin-Nicusor DuminicaNo ratings yet
- 6 PeritonDocument18 pages6 PeritonRian AprizaNo ratings yet
- Data Bocah2Document3 pagesData Bocah2Rian AprizaNo ratings yet
- PreventionDocument3 pagesPreventionRian AprizaNo ratings yet
- 3 FullDocument10 pages3 FullRian AprizaNo ratings yet
- ON-K5 Cancer PreventionDocument9 pagesON-K5 Cancer PreventionRian AprizaNo ratings yet
- Coronary Artery Stent Thrombosis - Incidence and Risk Factors - UpToDateDocument21 pagesCoronary Artery Stent Thrombosis - Incidence and Risk Factors - UpToDateCarlos Rubio LópezNo ratings yet
- Modified Jailed Balloon Technique For Coronary Artery Bifurcation LesionsDocument3 pagesModified Jailed Balloon Technique For Coronary Artery Bifurcation LesionsMonica TrifitrianaNo ratings yet
- Klasifikasi Prosedur ICD9CMDocument258 pagesKlasifikasi Prosedur ICD9CMJivitaBasarahNo ratings yet
- Milan Sonka, J. Michael Fitzpatrick - Handbook of Medical Imaging, Volume 2. Medical Image Processing and Analysis-SPIE PDFDocument1,284 pagesMilan Sonka, J. Michael Fitzpatrick - Handbook of Medical Imaging, Volume 2. Medical Image Processing and Analysis-SPIE PDFThương LêNo ratings yet
- Relation of Lipid Content of Coronary Plaque to Level of Serum Uric AcidDocument5 pagesRelation of Lipid Content of Coronary Plaque to Level of Serum Uric AciddidingNo ratings yet
- Top10ReasonsToUseIVUS PDFDocument71 pagesTop10ReasonsToUseIVUS PDFDiana PânteaNo ratings yet
- Impact of Artificial Intelligence On Interventional CardiologyDocument27 pagesImpact of Artificial Intelligence On Interventional CardiologyASIK1144No ratings yet
- Core Curriculum Subadventitial Techniques For Chronic Total Occlusion Percutaneous Coronary InterventionDocument10 pagesCore Curriculum Subadventitial Techniques For Chronic Total Occlusion Percutaneous Coronary InterventiongunaoNo ratings yet
- Cardiac Stress TestDocument32 pagesCardiac Stress Testarahman168No ratings yet
- Icd 9 CM (Tabulasi) 2012Document263 pagesIcd 9 CM (Tabulasi) 2012M Taufik Harahap100% (1)
- Advances in Bio-Mechanical Systems and Materials Ashkan JavadzadeganDocument148 pagesAdvances in Bio-Mechanical Systems and Materials Ashkan JavadzadeganNoa Noa ReyNo ratings yet
- Evolocumab 2Document13 pagesEvolocumab 2Rania El-DesokyNo ratings yet
- Chapter 3: Clinical Evaluation and InvestigationsDocument6 pagesChapter 3: Clinical Evaluation and Investigationsyunie0959No ratings yet
- Ashish Sarraju Atherosclerotic Plaque StabilizationDocument11 pagesAshish Sarraju Atherosclerotic Plaque Stabilizationdarkangelmx1No ratings yet
- Icd 9 CM 2010Document81 pagesIcd 9 CM 2010P17430203075 FANIA SEVI YULISTIRANo ratings yet
- Stagiu1-Cardiologie-Anul 4Document56 pagesStagiu1-Cardiologie-Anul 4Ozana CopyShopNo ratings yet
- Artis Zee Ceiling Datasheet 5.7.2019Document36 pagesArtis Zee Ceiling Datasheet 5.7.2019CeoĐứcTrường33% (3)
- ICD9CM2010Document666 pagesICD9CM2010Thyka MayasariNo ratings yet
- Esc Guidelines 2020 Nste-Acs FinalDocument34 pagesEsc Guidelines 2020 Nste-Acs FinalabcdefNo ratings yet
- EAT STEMI Volume Gohbara2016Document7 pagesEAT STEMI Volume Gohbara2016Wyah MpNo ratings yet
- P110019S075d PDFDocument319 pagesP110019S075d PDFCarlos ArroyoNo ratings yet
- CVT CompetencyDocument10 pagesCVT CompetencychirudarsiNo ratings yet
- Atherosclerosis: A Disease of ArteriesDocument35 pagesAtherosclerosis: A Disease of ArteriesSevda MemetNo ratings yet
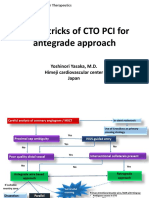
- Tips & Tricks of CTO PCI For Antegrade Approach: Yoshinori Yasaka, M.D. Himeji Cardiovascular Center JapanDocument21 pagesTips & Tricks of CTO PCI For Antegrade Approach: Yoshinori Yasaka, M.D. Himeji Cardiovascular Center JapanEll KlazureNo ratings yet
- Electrocardiography in Ischemic Heart Disease Clinical and Imaging Correlations and Prognostic ImplicationsDocument422 pagesElectrocardiography in Ischemic Heart Disease Clinical and Imaging Correlations and Prognostic ImplicationsAndonis AngelovNo ratings yet
- Minoca AhjDocument3 pagesMinoca AhjSundaresan SankarNo ratings yet
- Clinical Expert Consensus Document On Rotational Atherectomy From The Japanese Association of Cardiovascular Intervention and TherapeuticsDocument18 pagesClinical Expert Consensus Document On Rotational Atherectomy From The Japanese Association of Cardiovascular Intervention and TherapeuticsTeng Hsin-INo ratings yet
- Kawasaki DiseaseDocument33 pagesKawasaki Diseasejoshianandk100% (2)
- Catheter WiresDocument56 pagesCatheter WiresSaud ShirwanNo ratings yet
- Practical Aspects of IVUS-Guided Percutaneous Coronary InterventionDocument7 pagesPractical Aspects of IVUS-Guided Percutaneous Coronary InterventionRajesh JayakumarNo ratings yet