You might also like
- 20140721-Operational Patient Care Pathway JSP 950 AnnexA Ed3 FinalDocument6 pages20140721-Operational Patient Care Pathway JSP 950 AnnexA Ed3 FinalgmantzaNo ratings yet
- Wi-Qhse-0045 Rev 1 Merp Rev-1.Document20 pagesWi-Qhse-0045 Rev 1 Merp Rev-1.Isam AlasmoiNo ratings yet
- Letter Reg Resource Allocation - NHM FY 222-23Document3 pagesLetter Reg Resource Allocation - NHM FY 222-23Rohit VermaNo ratings yet
- Medical Support in FieldDocument23 pagesMedical Support in FieldJabedNo ratings yet
- Persentasi OkeDocument11 pagesPersentasi OkeLALU HERYNo ratings yet
- DOH MenuDocument10 pagesDOH MenuJohn Philip TiongcoNo ratings yet
- Kami Ma 2019Document8 pagesKami Ma 2019Muh Taufik Dwi PutraNo ratings yet
- Binder 2Document16 pagesBinder 2dradotttNo ratings yet
- Survival Guide For Task Force Medical Platoon Leadersv3Document90 pagesSurvival Guide For Task Force Medical Platoon Leadersv3Tyler Jackson100% (2)
- Guidelines On The Management of SDRA 2019 PDFDocument27 pagesGuidelines On The Management of SDRA 2019 PDFZakkyMaulanaRahmatNo ratings yet
- Organization, Roles and Tasks Section 1 GeneralDocument7 pagesOrganization, Roles and Tasks Section 1 GeneralfnkfabNo ratings yet
- Ards Best PDFDocument27 pagesArds Best PDFfraolNo ratings yet
- Top Messages: Paediatric Life Support 2021Document6 pagesTop Messages: Paediatric Life Support 2021Mihai Ion GhioaldaNo ratings yet
- National Health Insurance Scheme: Career Opportunities For Health WorkersDocument3 pagesNational Health Insurance Scheme: Career Opportunities For Health Workersyusuf hamidNo ratings yet
- Guia de Manejo Sdra 2019Document27 pagesGuia de Manejo Sdra 2019Jorge VidalNo ratings yet
- Fms Plan خطط ادارة الخدمات والسلامةDocument195 pagesFms Plan خطط ادارة الخدمات والسلامةMosfer Al kerdemNo ratings yet
- Hospital Response To A Major Incident: Initial Considerations and Longer Term EffectsDocument5 pagesHospital Response To A Major Incident: Initial Considerations and Longer Term EffectsMinaz PatelNo ratings yet
- Walk-In Interview For Doctors On Contractual Basis in Hospitals of Bhilai Steel PlantDocument7 pagesWalk-In Interview For Doctors On Contractual Basis in Hospitals of Bhilai Steel PlantMohaideen SubaireNo ratings yet
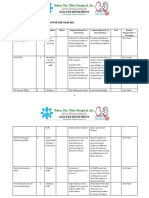
- Action Plan MHOMalungon SPHMalungonDocument5 pagesAction Plan MHOMalungon SPHMalungonClyde Cyril BaculioNo ratings yet
- IRHS ProfileDocument3 pagesIRHS ProfilesidharthNo ratings yet
- Teaching Experience Log 2019Document3 pagesTeaching Experience Log 2019د.حسن محمدNo ratings yet
- GL-PHYS-1 Total Hip ReplacementDocument8 pagesGL-PHYS-1 Total Hip Replacementmahmoud batnijiNo ratings yet
- Community Assessment Public Health - 2017Document7 pagesCommunity Assessment Public Health - 2017ardiansyah nochNo ratings yet
- Icm Ast Training Guide (For Trainees Commencing Icm Prior To 2017) (Updated Feb 2017)Document17 pagesIcm Ast Training Guide (For Trainees Commencing Icm Prior To 2017) (Updated Feb 2017)Del PalmeaNo ratings yet
- 2023 Reporting Requirements For HEDIS HOS and CAHPS 5-18-2022 GDocument9 pages2023 Reporting Requirements For HEDIS HOS and CAHPS 5-18-2022 GMintesinotNo ratings yet
- SDRA Guia Britanica 2019 PDFDocument27 pagesSDRA Guia Britanica 2019 PDFFernando IñiguezNo ratings yet
- Plasma Therapy PDocument12 pagesPlasma Therapy Plakshminivas PingaliNo ratings yet
- Health Emergency Kits Training 2019 PDFDocument33 pagesHealth Emergency Kits Training 2019 PDFrema_rhere95No ratings yet
- Staff Development Plan 2023Document5 pagesStaff Development Plan 2023SSNHI Dialysis Training CenterNo ratings yet
- Acut Care Surgery in Rural SVARASDocument37 pagesAcut Care Surgery in Rural SVARASJOHANES BERECHMANS PRANOTO RUMARATUNo ratings yet
- 2879 - AMedP-1.10 EDA V1 EDocument30 pages2879 - AMedP-1.10 EDA V1 EMiller ZeaNo ratings yet
- Clinical Volume 11 ISBAR Handover/Communication PolicyDocument4 pagesClinical Volume 11 ISBAR Handover/Communication PolicyArive Haruzz BizzaNo ratings yet
- CPBRD: NotesDocument12 pagesCPBRD: NotesSHIELA MAE ONIANo ratings yet
- Management of COPDDocument2 pagesManagement of COPDFreakyRustlee LeoragNo ratings yet
- Computational Uid Dynamics Modelling in Cardiovascular MedicineDocument12 pagesComputational Uid Dynamics Modelling in Cardiovascular MedicineMasterAlbus3dNo ratings yet
- 4-B (DILG) Consolidated NGA PAPs and CapDev - V. Sep 12 2022Document82 pages4-B (DILG) Consolidated NGA PAPs and CapDev - V. Sep 12 2022leonora.antonio58No ratings yet
- Approximate Dynamic Programming For Military Medical Evacuation Dispatching PoliciesDocument26 pagesApproximate Dynamic Programming For Military Medical Evacuation Dispatching PoliciesYessenia vela villcapazaNo ratings yet
- J Applied Clin Med Phys - 2023 - Liu - A Two Step Treatment Planning Strategy Incorporating Knowledge Based Planning ForDocument11 pagesJ Applied Clin Med Phys - 2023 - Liu - A Two Step Treatment Planning Strategy Incorporating Knowledge Based Planning ForPiotr JankowskiNo ratings yet
- Med SP Plan: Presented by Capt Imran Hossain 101 FD AmbDocument20 pagesMed SP Plan: Presented by Capt Imran Hossain 101 FD AmbShah NawazNo ratings yet
- PIIS0735675720302138Document2 pagesPIIS0735675720302138umpahNo ratings yet
- NABH Series2 COPDocument63 pagesNABH Series2 COPPallavi Deepak DongreNo ratings yet
- WHO AF CDS 03 - 2019 EngDocument52 pagesWHO AF CDS 03 - 2019 EngHossam El DefrawyNo ratings yet
- ACTIVITY DESIGN-FinalDocument3 pagesACTIVITY DESIGN-Finalnesrine kae zapantaNo ratings yet
- ICU Procedures ManualDocument64 pagesICU Procedures Manualenumula kumar100% (1)
- PD2014 025Document13 pagesPD2014 025brookie8868No ratings yet
- Notificationno.13/Dm&Ho/Atp/2020-21Dated. .11.2021Document4 pagesNotificationno.13/Dm&Ho/Atp/2020-21Dated. .11.2021matangi ramaraoNo ratings yet
- Sem.8.Surgery Timetable From 11.3.2019Document10 pagesSem.8.Surgery Timetable From 11.3.2019SharveenNo ratings yet
- Guidance For Prone Positioning in Adult Critical CareDocument40 pagesGuidance For Prone Positioning in Adult Critical CareAnnisa Eka FebryantiNo ratings yet
- EMP2 2 E12483Document9 pagesEMP2 2 E12483Akhmad KusairiNo ratings yet
- Prone Position in Adult Critical Care 2019 PDFDocument40 pagesProne Position in Adult Critical Care 2019 PDFKuroi RavenNo ratings yet
- Cdmp2015 HandbookDocument90 pagesCdmp2015 HandbookTony NgNo ratings yet
- CAP Regulation 60-5 - 08/17/2002Document3 pagesCAP Regulation 60-5 - 08/17/2002CAP History LibraryNo ratings yet
- STEMI Guidline 23.11.2022Document60 pagesSTEMI Guidline 23.11.2022NATARAJAN RAJENDRANNo ratings yet
- CAP Regulation 160-1 - 05/06/2002Document3 pagesCAP Regulation 160-1 - 05/06/2002CAP History LibraryNo ratings yet
- Bmjspcare 2018 001746.fullDocument8 pagesBmjspcare 2018 001746.fullepraetorianNo ratings yet
- AnnalsATS 202003-233PSDocument4 pagesAnnalsATS 202003-233PSambitiousamit1No ratings yet
- NIP Interim Guidelines On Chikiting Bakunation DaysDocument30 pagesNIP Interim Guidelines On Chikiting Bakunation DaysJL CalvinNo ratings yet
- ABBRDocument2 pagesABBRRuijia ZengNo ratings yet
- Battle Field Medical Force – Planning for 21St Century Medical ReadinessFrom EverandBattle Field Medical Force – Planning for 21St Century Medical ReadinessNo ratings yet
- Target Volume Delineation for Pediatric CancersFrom EverandTarget Volume Delineation for Pediatric CancersStephanie A. TerezakisNo ratings yet
- One gjjjj35566 TuuDocument2 pagesOne gjjjj35566 TuuShah NawazNo ratings yet
- Weekend CourseDocument1 pageWeekend CourseShah NawazNo ratings yet
- Technical Bulletin2 PDFDocument15 pagesTechnical Bulletin2 PDFShah NawazNo ratings yet
- Evsjv 'K M Ru: Iwr÷Vw© Bs WW G-1Document27 pagesEvsjv 'K M Ru: Iwr÷Vw© Bs WW G-1sohelalamNo ratings yet
- New 00999Document2 pagesNew 00999Shah NawazNo ratings yet
- Academic Cover LettersDocument5 pagesAcademic Cover Letterscoxo_designNo ratings yet
- HKG 45321600098Document2 pagesHKG 45321600098Shah NawazNo ratings yet
- Academic Cover LettersDocument5 pagesAcademic Cover Letterscoxo_designNo ratings yet
- Academic Cover LettersDocument5 pagesAcademic Cover Letterscoxo_designNo ratings yet
- File 222211383614033818Document27 pagesFile 222211383614033818Shah NawazNo ratings yet
- Syphilis Staging Chart PDFDocument2 pagesSyphilis Staging Chart PDFShah NawazNo ratings yet
- Paper 1 Model Test 3 FCPSDocument6 pagesPaper 1 Model Test 3 FCPSShah NawazNo ratings yet
- CircularDocument2 pagesCircularShah NawazNo ratings yet
- Med SP Plan: Presented by Capt Imran Hossain 101 FD AmbDocument20 pagesMed SP Plan: Presented by Capt Imran Hossain 101 FD AmbShah NawazNo ratings yet
- Med SP Plan: Presented by Capt Imran Hossain 101 FD AmbDocument20 pagesMed SP Plan: Presented by Capt Imran Hossain 101 FD AmbShah NawazNo ratings yet
- Paper 1 Model Test 3 FCPSDocument6 pagesPaper 1 Model Test 3 FCPSShah NawazNo ratings yet
- Med SP Plan: Presented by Capt Imran Hossain 101 FD AmbDocument20 pagesMed SP Plan: Presented by Capt Imran Hossain 101 FD AmbShah NawazNo ratings yet
- Fluid Electrolytes Acid-Base and ShockDocument18 pagesFluid Electrolytes Acid-Base and Shockjosephabram051590100% (1)
- Fluid and ElectrolytesDocument20 pagesFluid and ElectrolytesWyn Agustin100% (1)
- Mock Test 2 FcpsDocument4 pagesMock Test 2 FcpsShah NawazNo ratings yet
- Sba Mock Test Fcps BcpsDocument10 pagesSba Mock Test Fcps BcpsShah NawazNo ratings yet
- Mock Test 4Document3 pagesMock Test 4Shah NawazNo ratings yet
- Derma MCQ Ch01 PDFDocument20 pagesDerma MCQ Ch01 PDFShah NawazNo ratings yet
- Artery and VeinDocument12 pagesArtery and VeinShah NawazNo ratings yet
- dv09144 PDFDocument1 pagedv09144 PDFSaliha ZainabNo ratings yet
- Derma MCQ Ch01 PDFDocument20 pagesDerma MCQ Ch01 PDFShah NawazNo ratings yet
- Fluids and Electrolytes MCQ S LJDocument5 pagesFluids and Electrolytes MCQ S LJVicviclookThekingNo ratings yet
- Multiple-Choice Questions: For All Questions, Select The Single Best Answer Unless Otherwise DirectedDocument67 pagesMultiple-Choice Questions: For All Questions, Select The Single Best Answer Unless Otherwise DirectedShah NawazNo ratings yet
- Dermatopathology Q - ADocument55 pagesDermatopathology Q - AKhalifa AL-Wishahi100% (7)
- ProgrammableFlow Intro - Sep2011Document39 pagesProgrammableFlow Intro - Sep2011Serge StasovNo ratings yet
- Soundarya Lahari Translation in EnglishDocument50 pagesSoundarya Lahari Translation in EnglishRanganatha Gowda100% (1)
- Technology and The Transformation of Performance - Chris Salter PDFDocument49 pagesTechnology and The Transformation of Performance - Chris Salter PDFFelipe Merker Castellani100% (1)
- (Ronald Weed, John Von Heyking (Eds.) ) Civil ReligiDocument375 pages(Ronald Weed, John Von Heyking (Eds.) ) Civil ReligiskaspeNo ratings yet
- Vo 1263 AaDocument8 pagesVo 1263 Aa801400No ratings yet
- Manila Revenue Code, As Amended (Ordinance No. 7988)Document121 pagesManila Revenue Code, As Amended (Ordinance No. 7988)Charles Augustine AlbañoNo ratings yet
- Aircraft Performance NPTELDocument538 pagesAircraft Performance NPTELShabbir Ali100% (2)
- Some Lower Bounds On The Reach of An Algebraic Variety: Chris La Valle Josué Tonelli-CuetoDocument9 pagesSome Lower Bounds On The Reach of An Algebraic Variety: Chris La Valle Josué Tonelli-CuetospanishramNo ratings yet
- Pharmaceutics Exam 3 - This SemesterDocument6 pagesPharmaceutics Exam 3 - This Semesterapi-3723612100% (1)
- COVID-19 Impact On Global Food IndustryDocument8 pagesCOVID-19 Impact On Global Food IndustryRavirajNo ratings yet
- The Hidden Word Is: The CluesDocument2 pagesThe Hidden Word Is: The CluesИра НикулочкинаNo ratings yet
- A 204Document1 pageA 204AnuranjanNo ratings yet
- Adios CancerDocument66 pagesAdios CancerQuoc Thai Qld100% (2)
- EST110-Dec 2021 Q&ADocument14 pagesEST110-Dec 2021 Q&ASreejith S NairNo ratings yet
- Land PollutionDocument2 pagesLand PollutionmoniqueNo ratings yet
- The Empire in FlamesDocument73 pagesThe Empire in FlamesSergio Esperalta Gata100% (2)
- PB Alumec EnglishDocument12 pagesPB Alumec EnglishByron RodriguezNo ratings yet
- Thermal Engineering IDocument30 pagesThermal Engineering IRamphani NunnaNo ratings yet
- Hyundai D4FB Diesel Fuel System 2Document727 pagesHyundai D4FB Diesel Fuel System 2Alexey Koshelnik100% (1)
- Lisa-Operation Manual: Installation and Operation Instructions (Part B)Document41 pagesLisa-Operation Manual: Installation and Operation Instructions (Part B)majdNo ratings yet
- Acetaldehyde Solution SDSDocument10 pagesAcetaldehyde Solution SDSJuan Carlos Blanco LeónNo ratings yet
- Title: "The Effect of Flooding in The Tourism Industry in Dagupan City" Rationale and Background of The StudyDocument4 pagesTitle: "The Effect of Flooding in The Tourism Industry in Dagupan City" Rationale and Background of The StudyTaehyung KimNo ratings yet
- Carte Tehnica Panou Fotovoltaic Cu Celule Policristaline Eging 250 WDocument1 pageCarte Tehnica Panou Fotovoltaic Cu Celule Policristaline Eging 250 WConstantin CilibiuNo ratings yet
- Anatomy-Head and NeckDocument94 pagesAnatomy-Head and NeckXahid IqbalNo ratings yet
- Computer Graphics Chapter-1Document61 pagesComputer Graphics Chapter-1abdi geremewNo ratings yet
- BS en 480-6-2005Document5 pagesBS en 480-6-2005Abey Vettoor0% (1)
- OCDM2223 Tutorial7solvedDocument5 pagesOCDM2223 Tutorial7solvedqq727783No ratings yet
- Berk-2009-Journal of Forensic SciencesDocument9 pagesBerk-2009-Journal of Forensic SciencesClaudio NovaesNo ratings yet
- 2011 33 MaintenanceDocument16 pages2011 33 MaintenanceKrishna Khandige100% (1)
- Aviation GeographyDocument22 pagesAviation Geographyweed cokeNo ratings yet