You might also like
- Problem Based LearningDocument71 pagesProblem Based LearningMedCoffee100% (1)
- 209-Hematology Review - Case StudiesDocument129 pages209-Hematology Review - Case StudiesKhalid Khalidi100% (2)
- Life Cycle of Parasites CDCDocument15 pagesLife Cycle of Parasites CDCDioso, Alyca Proe0% (1)
- Aplastic Anemia Lecture 1aDocument39 pagesAplastic Anemia Lecture 1aniaaseta100% (2)
- Anemia Pres OrginalDocument61 pagesAnemia Pres OrginalenooNo ratings yet
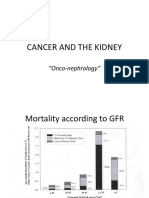
- Cancer and The KidneyDocument29 pagesCancer and The Kidney[ qιlα ]No ratings yet
- Bone Marrow Failure VoiceoverDocument18 pagesBone Marrow Failure Voiceoverياسر كوثر هانيNo ratings yet
- Fatigue: What Is Anemia?Document3 pagesFatigue: What Is Anemia?Annapurna DangetiNo ratings yet
- A. Thalassemia Is An Inherited Disorder of Hemoglobin (HB) Synthesis, So It Is An AnemiaDocument15 pagesA. Thalassemia Is An Inherited Disorder of Hemoglobin (HB) Synthesis, So It Is An AnemiaM Hairullah IrulNo ratings yet
- Aplast AnDocument9 pagesAplast Anj.doe.hex_87No ratings yet
- Anemia PPT - KeyDocument16 pagesAnemia PPT - KeyAyman RehmanNo ratings yet
- 1a.blood Notes 2Document4 pages1a.blood Notes 2deemahNo ratings yet
- 1 ThalassemiaDocument15 pages1 ThalassemiaMohamed Na3eemNo ratings yet
- Aplastic Anemia and HomoeopathyDocument3 pagesAplastic Anemia and HomoeopathyDr. Rajneesh Kumar Sharma MD Hom100% (1)
- Sickle Cell DiseaseDocument38 pagesSickle Cell DiseasemegaNo ratings yet
- Aplastic AnemiaDocument29 pagesAplastic AnemiaAshish SoniNo ratings yet
- Research ThalasimiaDocument11 pagesResearch ThalasimiaaminmofrehNo ratings yet
- Acute Myeloid LuekemiaDocument30 pagesAcute Myeloid LuekemiaKathleen DimacaliNo ratings yet
- Anemia and Pyometra in DogsDocument20 pagesAnemia and Pyometra in DogsVer FajaNo ratings yet
- Anaemia of Chronic Disorders (1) IntroductionDocument21 pagesAnaemia of Chronic Disorders (1) IntroductionTshwarelo LegodiNo ratings yet
- Leukemias 2Document56 pagesLeukemias 2Y. Beatrice AbigailNo ratings yet
- Hemopoietic SystemDocument28 pagesHemopoietic Systemyfzzhgv676No ratings yet
- Clinical Hematological: Assist Prof. Dr. Mudhir S. ShekhaDocument24 pagesClinical Hematological: Assist Prof. Dr. Mudhir S. ShekhaAhmed. Masud.OthmanNo ratings yet
- Hematological DisorderDocument49 pagesHematological DisorderSandeepNo ratings yet
- Blood DisordersDocument8 pagesBlood DisordersDeevashwer Rathee100% (1)
- Acute Myeloid Leukaemia (AML)Document27 pagesAcute Myeloid Leukaemia (AML)Immortal AndyNo ratings yet
- Gangguan TrombositDocument47 pagesGangguan TrombositLayli Nur ArniatiNo ratings yet
- (8-9) Hemolytic A.and AplasticDocument68 pages(8-9) Hemolytic A.and AplasticdfrdhpvbdxNo ratings yet
- Anemias Aplastic Anemia Is A Condition Where Bone Marrow Does Not Produce Sufficient NewDocument15 pagesAnemias Aplastic Anemia Is A Condition Where Bone Marrow Does Not Produce Sufficient NewZoreyca RiveraNo ratings yet
- Review Jurnal Anfisman Grup G English VersionDocument11 pagesReview Jurnal Anfisman Grup G English VersionKayla NikenNo ratings yet
- Aplastic Anemia - An Overview: DR Aniruddh Shrivastava Guided By: DR S.H. Talib SIRDocument42 pagesAplastic Anemia - An Overview: DR Aniruddh Shrivastava Guided By: DR S.H. Talib SIRdoctoranswerit_84161No ratings yet
- Aplastic AnemiaDocument6 pagesAplastic AnemiaJoezer Gumangan VeranoNo ratings yet
- Anemi Aplastik Dan MielodisplasiaDocument34 pagesAnemi Aplastik Dan MielodisplasiaRoby KieranNo ratings yet
- Aplastic Anemia, 2008Document10 pagesAplastic Anemia, 2008j.doe.hex_87No ratings yet
- Feline Anemia Diagnostic AlgorithmDocument1 pageFeline Anemia Diagnostic AlgorithmEd BlackadderNo ratings yet
- Symtomps of Illness and DiseaseDocument4 pagesSymtomps of Illness and DiseaseSilvana SabillaNo ratings yet
- Caring For Clients With The Disorders of The Hematopoetic SystemDocument39 pagesCaring For Clients With The Disorders of The Hematopoetic SystemRose AlmanzorNo ratings yet
- Thalassemia: Dr. Shadab Jamal MakhdoomiDocument22 pagesThalassemia: Dr. Shadab Jamal MakhdoomiShadab JamalNo ratings yet
- Blood Diseases تقرير امراض الدمDocument7 pagesBlood Diseases تقرير امراض الدمBedo IbrahimNo ratings yet
- Caring For Patients With Hematologic DisordersDocument54 pagesCaring For Patients With Hematologic Disorderspioneergloria51No ratings yet
- Acute Myeloblastic Leukemia AML: Dr. Amged H.AbdelrhmanDocument23 pagesAcute Myeloblastic Leukemia AML: Dr. Amged H.Abdelrhmanد. أمجد حسين عبد الرحمنNo ratings yet
- MRCPass Notes For MRCP 1 - HEMATOLOGYDocument9 pagesMRCPass Notes For MRCP 1 - HEMATOLOGYsabdali100% (1)
- Anaemia - B12 and Folate Deficiency: SummaryDocument16 pagesAnaemia - B12 and Folate Deficiency: Summarymyat252100% (1)
- Blood and Its DisorderDocument29 pagesBlood and Its DisorderPrapti GautamNo ratings yet
- Blood Disorders 11Document50 pagesBlood Disorders 11Purnendu ParidaNo ratings yet
- Aplastic AnemiaDocument6 pagesAplastic AnemiaChukwu Henry ParadiseNo ratings yet
- Bio Case Study 1Document7 pagesBio Case Study 1Christian GallardoNo ratings yet
- Thesis AnemiaDocument7 pagesThesis AnemiaBuyPapersForCollegeSingapore100% (1)
- Emergency Medicine Clinics of North America Volume Issue 2014 (Doi 10.1016 - J.emc.2014.04.007) Vieth, Julie T. Lane, David R. - AnemiaDocument16 pagesEmergency Medicine Clinics of North America Volume Issue 2014 (Doi 10.1016 - J.emc.2014.04.007) Vieth, Julie T. Lane, David R. - AnemiaJeffrey Stefan Pal RiveraNo ratings yet
- CASE PRE - Acute Lymphoblastic LeukemiaDocument153 pagesCASE PRE - Acute Lymphoblastic Leukemiacecille_javier100% (4)
- Sickle-Cell AnemiaDocument11 pagesSickle-Cell Anemiahalzen_joyNo ratings yet
- Hematology Topics 16-20Document20 pagesHematology Topics 16-20Angelo Jude CobachaNo ratings yet
- Saint Luke's College Of: NursingDocument6 pagesSaint Luke's College Of: NursingApril Mae Magos LabradorNo ratings yet
- Genes and Human Disease: Monogenic DiseasesDocument8 pagesGenes and Human Disease: Monogenic DiseasesE.R.ONo ratings yet
- Genes and Human Disease: Monogenic DiseasesDocument8 pagesGenes and Human Disease: Monogenic DiseasesE.R.ONo ratings yet
- Medical Disorder Considerations in Orthodontic Patients NDocument115 pagesMedical Disorder Considerations in Orthodontic Patients Nshubhangi_jain_10No ratings yet
- Normocytic AnemiaDocument16 pagesNormocytic AnemiaPaula ArayaNo ratings yet
- Hematology: Done By: Ahmed AlsolamiDocument52 pagesHematology: Done By: Ahmed AlsolamiEmad Manni100% (1)
- Physical ExamDocument15 pagesPhysical ExamDr AbdulkadirNo ratings yet
- Chest PainDocument19 pagesChest PainDr AbdulkadirNo ratings yet
- Plasma University: Guriel-GalgadudDocument26 pagesPlasma University: Guriel-GalgadudDr AbdulkadirNo ratings yet
- Plasma University: Guriel-GalgadudDocument12 pagesPlasma University: Guriel-GalgadudDr AbdulkadirNo ratings yet
- Physical ExamDocument15 pagesPhysical ExamDr AbdulkadirNo ratings yet
- Physical ExamDocument15 pagesPhysical ExamDr AbdulkadirNo ratings yet
- DR Abdikadir Medicine and Clinical DiagnosisDocument3 pagesDR Abdikadir Medicine and Clinical DiagnosisDr AbdulkadirNo ratings yet
- Plasma University: Guriel-GalgadudDocument12 pagesPlasma University: Guriel-GalgadudDr AbdulkadirNo ratings yet
- Cardiovascular DiseaseDocument20 pagesCardiovascular DiseaseDr AbdulkadirNo ratings yet
- Hem Morag HeDocument12 pagesHem Morag HeDr AbdulkadirNo ratings yet
- Aplastic AnemiaDocument19 pagesAplastic AnemiaDr AbdulkadirNo ratings yet
- Cardiovascular DiseaseDocument20 pagesCardiovascular DiseaseDr AbdulkadirNo ratings yet
- Chest PainDocument19 pagesChest PainDr AbdulkadirNo ratings yet
- Plasma University: Guriel-GalgadudDocument26 pagesPlasma University: Guriel-GalgadudDr AbdulkadirNo ratings yet
- Plasma University: Guriel-GalgadudDocument12 pagesPlasma University: Guriel-GalgadudDr AbdulkadirNo ratings yet
- Chest PainDocument19 pagesChest PainDr AbdulkadirNo ratings yet
- Plasma University: Guriel-GalgadudDocument12 pagesPlasma University: Guriel-GalgadudDr AbdulkadirNo ratings yet
- Cardiovascular DiseaseDocument20 pagesCardiovascular DiseaseDr AbdulkadirNo ratings yet
- Plasma University: Guriel-GalgadudDocument12 pagesPlasma University: Guriel-GalgadudDr AbdulkadirNo ratings yet
- Plasma University: Guriel-Galgadud RegionDocument17 pagesPlasma University: Guriel-Galgadud RegionDr AbdulkadirNo ratings yet
- Aplastic AnemiaDocument19 pagesAplastic AnemiaDr AbdulkadirNo ratings yet
- Chest PainDocument19 pagesChest PainDr AbdulkadirNo ratings yet
- Aplastic AnemiaDocument19 pagesAplastic AnemiaDr AbdulkadirNo ratings yet
- Cardiovascular DiseaseDocument20 pagesCardiovascular DiseaseDr AbdulkadirNo ratings yet
- Chest PainDocument19 pagesChest PainDr AbdulkadirNo ratings yet
- Bed Side Teaching: By: Elda AriyaniDocument13 pagesBed Side Teaching: By: Elda Ariyanielda ariyaniNo ratings yet
- English 5 Quarter 3 Week 1 Las 3Document2 pagesEnglish 5 Quarter 3 Week 1 Las 3Cristine Joy Villajuan AndresNo ratings yet
- 30secondary GlaucomasDocument9 pages30secondary GlaucomasArtha CimutNo ratings yet
- Headache HarrisonDocument21 pagesHeadache HarrisonJega PandianNo ratings yet
- Article On Legality of COVID Lockdown in IndiaDocument1 pageArticle On Legality of COVID Lockdown in IndiaKanhaiya SinghalNo ratings yet
- Bipolar Disorders - 2023 - Ponzer - Lithium and Risk of Cardiovascular Disease Dementia and Venous ThromboembolismDocument11 pagesBipolar Disorders - 2023 - Ponzer - Lithium and Risk of Cardiovascular Disease Dementia and Venous ThromboembolismKonstantinos RantisNo ratings yet
- Hodgkin's LymphomaDocument14 pagesHodgkin's LymphomaBeulah AlexNo ratings yet
- Diskusi Kasus Kelas B 1.: Characteristic ResultDocument6 pagesDiskusi Kasus Kelas B 1.: Characteristic ResultBagas aninditoNo ratings yet
- Peran IPCNDocument38 pagesPeran IPCNSANITASI LINGKUNGAN RSPBGNo ratings yet
- ch4 Question Bank-1-3Document3 pagesch4 Question Bank-1-3AAYUSHI PARMARNo ratings yet
- Aegypti and Aedes Albopictus. There Are Four DistinctDocument5 pagesAegypti and Aedes Albopictus. There Are Four DistinctChia Yin NgNo ratings yet
- Important QuestionsDocument31 pagesImportant QuestionssandeepNo ratings yet
- Volume3 Issue4 Jul Aug No.329 665 667Document3 pagesVolume3 Issue4 Jul Aug No.329 665 667MadeKurniawanAsNo ratings yet
- Thyroid CrisisDocument11 pagesThyroid CrisisKoka KolaNo ratings yet
- Accoplishment Report Feeding Program Jan Feb20Document8 pagesAccoplishment Report Feeding Program Jan Feb20Ana Abatay RamosNo ratings yet
- Inflammatory Bowel Disease (IBD)Document41 pagesInflammatory Bowel Disease (IBD)ririNo ratings yet
- Sexually Transmitted Infections: BY: DR Olasinde Abdulazeez Ayodeji Department of Community Medicine, ABUTH ZariaDocument14 pagesSexually Transmitted Infections: BY: DR Olasinde Abdulazeez Ayodeji Department of Community Medicine, ABUTH ZariaSalihu MustaphaNo ratings yet
- تقرير اشعه اسنانDocument10 pagesتقرير اشعه اسنانSaif HashimNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : Section A - Patient DetailsDocument2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : Section A - Patient DetailsDEE QC CHittoorNo ratings yet
- 9 Clinical IndicatorDocument7 pages9 Clinical IndicatorJatoveda HaldarNo ratings yet
- DRUG STUDY (Head Injury)Document3 pagesDRUG STUDY (Head Injury)Paula Suplico NiangarNo ratings yet
- Understanding Your Hepatitis B Blood TestsDocument2 pagesUnderstanding Your Hepatitis B Blood TestsSam Sep A SixtyoneNo ratings yet
- Kode Diagnosa BpjsDocument6 pagesKode Diagnosa BpjsRahma SkincareNo ratings yet
- LR 364372Document9 pagesLR 364372Fredgar22No ratings yet
- Mathur 2015Document7 pagesMathur 2015Maximiliano OliveraNo ratings yet
- Volume 9 No 1Document94 pagesVolume 9 No 1ChristopherLawrenceNo ratings yet
- Covid19 InvestigationDocument9 pagesCovid19 InvestigationAndreArtigasNo ratings yet
- McDonald Criteria 2005Document2 pagesMcDonald Criteria 2005api-3828181100% (1)
- Office of The Secretary: 0 0013 OrderDocument23 pagesOffice of The Secretary: 0 0013 OrderChristian Christopher LopezNo ratings yet