You might also like
- EmotionalIntelligence TestDocument65 pagesEmotionalIntelligence Testjogutierrez100% (2)
- Internal Medicine #1Document167 pagesInternal Medicine #1Nikhil RayarakulaNo ratings yet
- 7 - Topnotch Pharmacology SuperExamDocument83 pages7 - Topnotch Pharmacology SuperExamVien Cervantes83% (6)
- Concepts of Personal BoundariesDocument11 pagesConcepts of Personal BoundarieshayazeNo ratings yet
- Summarised Clinchers Created For The Exam - Credits - Audi Maglalang-ReedDocument9 pagesSummarised Clinchers Created For The Exam - Credits - Audi Maglalang-ReedflashjetNo ratings yet
- Asthma COPD Overlap Syndrome - ACOSDocument59 pagesAsthma COPD Overlap Syndrome - ACOSdrmaqsoodaliNo ratings yet
- 2 - Respiratory Passmedicine Q. Bank PART I 2017Document336 pages2 - Respiratory Passmedicine Q. Bank PART I 2017'محمد علي' محمد لافي100% (1)
- Case Presentation On Chronic BronchitisDocument20 pagesCase Presentation On Chronic BronchitisSafoora RafeeqNo ratings yet
- PASSMEDICINE MCQs-RESPIRATORY MEDICINEDocument111 pagesPASSMEDICINE MCQs-RESPIRATORY MEDICINEHashim Ahmad83% (6)
- Pneumonia Case StudyDocument24 pagesPneumonia Case StudyDharylle Cariño100% (1)
- Patient Satisfaction Regarding Healthcare ServicesDocument30 pagesPatient Satisfaction Regarding Healthcare ServicesSagar Tanna67% (3)
- MPS and Item AnalysisDocument177 pagesMPS and Item AnalysisMary Ann Palima80% (5)
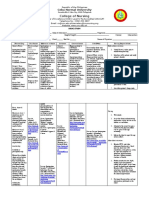
- College of Nursing: Cebu Normal UniversityDocument4 pagesCollege of Nursing: Cebu Normal UniversityChelsea Wu100% (1)
- Asma 2022 PDFDocument66 pagesAsma 2022 PDFBagas Trikuncoro BawonoNo ratings yet
- NPO Slides 110Document52 pagesNPO Slides 110Yaya ManNo ratings yet
- Salbutamol + IpratropiumDocument3 pagesSalbutamol + IpratropiumShiva TorinsNo ratings yet
- Management of Intraoperative Bronchospasm: Dr. ImranDocument49 pagesManagement of Intraoperative Bronchospasm: Dr. ImranhellodrvigneshwarNo ratings yet
- AsthmaDocument5 pagesAsthmaShalini ShanmugalingamNo ratings yet
- Respiratory Drugs Asthma COPD Allergic RhinitisDocument84 pagesRespiratory Drugs Asthma COPD Allergic RhinitisLyn LynNo ratings yet
- Respiratory PasTest MRCP II 2021Document1,050 pagesRespiratory PasTest MRCP II 2021kathi raja sekharNo ratings yet
- Global Strategyfor Asthma ManagementDocument88 pagesGlobal Strategyfor Asthma ManagementkhanhquphamNo ratings yet
- Pharmacology - Respiratory SystemDocument9 pagesPharmacology - Respiratory Systemwedikaf807No ratings yet
- AsthmaDocument7 pagesAsthmaSUSHIL KUMAR OLINo ratings yet
- Case Presentation On Respiratory Track InfectionDocument22 pagesCase Presentation On Respiratory Track InfectionNewtan DebNo ratings yet
- AsthmaDocument42 pagesAsthma7w2b96qznkNo ratings yet
- Cme Bronchial AsthmaDocument28 pagesCme Bronchial AsthmaameerabestNo ratings yet
- CASE-STUDY-Infectious DiseaseDocument8 pagesCASE-STUDY-Infectious DiseaseJoshua RamirezNo ratings yet
- 101-113 SBAsDocument222 pages101-113 SBAsRahul DhulipalaNo ratings yet
- Gina Asma 2019Document88 pagesGina Asma 2019Naufal HasanNo ratings yet
- Chronic Asthma Guidelines: in Adolescents & Adults 2007Document58 pagesChronic Asthma Guidelines: in Adolescents & Adults 2007Dark_loveNo ratings yet
- Asthma GowryDocument98 pagesAsthma Gowryv_vijayakanth7656No ratings yet
- Case Presentation On Ugi Bleed 2 ToDocument25 pagesCase Presentation On Ugi Bleed 2 ToMaira KhanNo ratings yet
- AsthmaDocument8 pagesAsthmahusainozelNo ratings yet
- COPD - Staff .TrainingDocument18 pagesCOPD - Staff .TrainingFun AppNo ratings yet
- COPD Flow SheetDocument2 pagesCOPD Flow SheetSachin PillaiNo ratings yet
- PulmCrit - Mastering The Dark Arts of BiPAP & HFNCDocument13 pagesPulmCrit - Mastering The Dark Arts of BiPAP & HFNCTusar KoleNo ratings yet
- Medical Case II NEWDocument31 pagesMedical Case II NEWTria MeirissaNo ratings yet
- Can Anyone Help Me With A Human Physiology Question? - What Is This Students Disorder? Heres The Assignment.?Document2 pagesCan Anyone Help Me With A Human Physiology Question? - What Is This Students Disorder? Heres The Assignment.?dr_finch511No ratings yet
- Asma 2020Document66 pagesAsma 2020sarifullatang laseNo ratings yet
- Inhaler Technique Info Paper 20180607 WebDocument16 pagesInhaler Technique Info Paper 20180607 WebHopeton SinclairNo ratings yet
- COPD Management (Read Code H3) : Severity POST Bronchodilator FEV (% of Predicted Value)Document6 pagesCOPD Management (Read Code H3) : Severity POST Bronchodilator FEV (% of Predicted Value)Anny AunNo ratings yet
- Paediatric Clinical GuidelinesDocument7 pagesPaediatric Clinical GuidelinesAndriNo ratings yet
- Atopic Disease Bronchial AsthmaDocument33 pagesAtopic Disease Bronchial AsthmaEmeraldyModyNo ratings yet
- Antiasthmatic DrugsDocument36 pagesAntiasthmatic DrugsJannah ZahraaNo ratings yet
- (Chronic Obstructive Pulmonary Disease) : Group 2Document47 pages(Chronic Obstructive Pulmonary Disease) : Group 2quocanh96110No ratings yet
- Acid Base WorksheetDocument1 pageAcid Base WorksheetMarshallMcGoughNo ratings yet
- Respiratory MRCP II Pastest 2023Document979 pagesRespiratory MRCP II Pastest 2023Tanzir Islam BrittoNo ratings yet
- Asma 2019Document64 pagesAsma 2019ajeng putriNo ratings yet
- Bronchial Asthma: Marshell Tendean, MD Departemen of Internal Medicine UKRIDA - JakartaDocument39 pagesBronchial Asthma: Marshell Tendean, MD Departemen of Internal Medicine UKRIDA - JakartamiazaraNo ratings yet
- 3 RRP COPD GuidelinesDocument4 pages3 RRP COPD Guidelinesjyothi vallabhaneniNo ratings yet
- GP Reg - Asthma and Spirometry 2011Document114 pagesGP Reg - Asthma and Spirometry 2011minerva_stanciuNo ratings yet
- Asthma and Atopic Eczema Asthma and Atopic Eczema Asthma and Atopic Eczema Asthma and Atopic EczemaDocument14 pagesAsthma and Atopic Eczema Asthma and Atopic Eczema Asthma and Atopic Eczema Asthma and Atopic EczemaTom Mallinson100% (1)
- Case Presentation ON Bronchial Asthma With Acute Copd ExacerbationDocument20 pagesCase Presentation ON Bronchial Asthma With Acute Copd ExacerbationJigeesha LakshmiNo ratings yet
- Peds 2 - Pulmonary Disorders of ChildrenDocument27 pagesPeds 2 - Pulmonary Disorders of ChildrenMinh Nguyễn Phương HồngNo ratings yet
- AECOPD GuidelineDocument1 pageAECOPD GuidelineOperations Manager - CMCNo ratings yet
- LinkoviDocument73 pagesLinkoviClementonicNo ratings yet
- Submodule Common DrugsDocument5 pagesSubmodule Common DrugsjackienospamNo ratings yet
- BR08Document19 pagesBR08Thao NguyenNo ratings yet
- Terapi Akne Ciproterone Acetate Oleh Dr. Abraham Arimuko SPKK Mars Finsdv FaadvDocument32 pagesTerapi Akne Ciproterone Acetate Oleh Dr. Abraham Arimuko SPKK Mars Finsdv FaadvshabrinaerinNo ratings yet
- c64 Section3 Spirometry 2014Document19 pagesc64 Section3 Spirometry 2014Mihai PetrescuNo ratings yet
- Difficult Asthma GuidelinesDocument6 pagesDifficult Asthma GuidelinesLee SakieNo ratings yet
- Copd FK Unhas 2015Document28 pagesCopd FK Unhas 2015Muhammad Nur DelaphanEnamNo ratings yet
- Management VasculopatyDocument23 pagesManagement VasculopatyAgus SusantoNo ratings yet
- Terpenoids: Recent Advances in Extraction, Biochemistry and BiotechnologyFrom EverandTerpenoids: Recent Advances in Extraction, Biochemistry and BiotechnologyNo ratings yet
- SS7 Training and Sigtran Training Provided by SS7Document13 pagesSS7 Training and Sigtran Training Provided by SS7parulparas1100% (2)
- Important Instructions:: Theories of Communication Mcm511Document2 pagesImportant Instructions:: Theories of Communication Mcm511Nasir AslamNo ratings yet
- Missing or Stolen Property Investigation Checklist PDFDocument1 pageMissing or Stolen Property Investigation Checklist PDFJigme ThinleyNo ratings yet
- A Study On Customer Satisfaction Towards Parachute Hair Oil With Reference To Coimbatore CityDocument3 pagesA Study On Customer Satisfaction Towards Parachute Hair Oil With Reference To Coimbatore CityAbner Alexander Luiz86% (7)
- Tool - ROI CalculatorDocument10 pagesTool - ROI CalculatorTan TanNo ratings yet
- PIL Lecture Notes - Week 1Document3 pagesPIL Lecture Notes - Week 1Yoshita SoodNo ratings yet
- Impaired Social InteractionDocument3 pagesImpaired Social InteractionJOYCE ANNE SUERTE DAGDAGANNo ratings yet
- Basic Résumé Types: 1. Chronological ResumeDocument9 pagesBasic Résumé Types: 1. Chronological ResumeDegee O. GonzalesNo ratings yet
- Rahail's ResumeDocument3 pagesRahail's ResumeRahailSalamatNo ratings yet
- Adjuvant Icotinib Versus Observation in Patients WDocument11 pagesAdjuvant Icotinib Versus Observation in Patients WVanilson BorgesNo ratings yet
- Romanian Language Not As We Know ItDocument35 pagesRomanian Language Not As We Know ItMiryamCriNo ratings yet
- Original PDF Deviant Behavior 11th Edition by Erich Goode PDFDocument41 pagesOriginal PDF Deviant Behavior 11th Edition by Erich Goode PDFcynthia.stewart295100% (32)
- 1984 Chapter One WorksheetDocument1 page1984 Chapter One WorksheetSteven DaviesNo ratings yet
- Rizal Report - 19TH CenturyDocument25 pagesRizal Report - 19TH CenturyNamja PyosiNo ratings yet
- Unit 7 Memory Cognition Checks For Understanding Answers Fall 2013Document6 pagesUnit 7 Memory Cognition Checks For Understanding Answers Fall 2013api-261267976No ratings yet
- Sources of Islamic LawDocument7 pagesSources of Islamic LawTayyab H. HashmiNo ratings yet
- A20Document15 pagesA20abdNo ratings yet
- LibreView Guide - Italian PaperDocument12 pagesLibreView Guide - Italian PaperJesus MuñozNo ratings yet
- CBSE Tuts: NCERT Class 10 Science Lab Manual - Image Formation by A Convex LensDocument16 pagesCBSE Tuts: NCERT Class 10 Science Lab Manual - Image Formation by A Convex LensVinodKumarTummalurNo ratings yet
- M1 Questions REV SP23Document2 pagesM1 Questions REV SP23Melia MorrisNo ratings yet
- Case Study 2Document15 pagesCase Study 2Abdullah ghauriNo ratings yet
- Sample Exam COMP 9444 NEURAL NETWORKS PDFDocument7 pagesSample Exam COMP 9444 NEURAL NETWORKS PDFAlshabwani SalehNo ratings yet
- Clinical Field Experience A Week 2 ECE-230 D.laneDocument1 pageClinical Field Experience A Week 2 ECE-230 D.laneDeborah laneNo ratings yet
- Feeding Power To Arduino - The Ultimate GuideDocument24 pagesFeeding Power To Arduino - The Ultimate GuideMUSTAFANo ratings yet
- Abc Chapter 2Document22 pagesAbc Chapter 2ZNo ratings yet
- Course Hero 41Document5 pagesCourse Hero 41Maria Helen MarcelinoNo ratings yet