You might also like
- Inflammatory Bowel Disease (Ibd)Document28 pagesInflammatory Bowel Disease (Ibd)suhaNo ratings yet
- Inflammatory Bowel DiseaseDocument19 pagesInflammatory Bowel Diseasenathan asfahaNo ratings yet
- Clinical Manifestations, Diagnosis, and Prognosis of Crohn Disease in AdultsDocument17 pagesClinical Manifestations, Diagnosis, and Prognosis of Crohn Disease in AdultsAsclepioNo ratings yet
- Ulcerativecolitis 170323180448 PDFDocument88 pagesUlcerativecolitis 170323180448 PDFBasudewo Agung100% (1)
- Crohns DiseaseDocument32 pagesCrohns DiseaseMin Chi PakNo ratings yet
- Clinical-Manifestations-Diagnosis and Prognosis of Crohn DiseaseDocument46 pagesClinical-Manifestations-Diagnosis and Prognosis of Crohn DiseasejzainounNo ratings yet
- DefinitionDocument12 pagesDefinitionAylol 23No ratings yet
- Clinical Manifestations, Diagnosis, and Prognosis of Crohn Disease in Adults - UpToDateDocument45 pagesClinical Manifestations, Diagnosis, and Prognosis of Crohn Disease in Adults - UpToDateAsclepioNo ratings yet
- 28 - IbdDocument57 pages28 - IbdsitiNo ratings yet
- IBD - Shane Ryan ApperleyDocument63 pagesIBD - Shane Ryan Apperleyvivi avisaNo ratings yet
- Ulcerative ColitisDocument30 pagesUlcerative ColitisAndika SulistianNo ratings yet
- Ulcerative Colitis: DR Syed Ubaid Associate Professor of SurgeryDocument71 pagesUlcerative Colitis: DR Syed Ubaid Associate Professor of SurgeryFachry Al RafiqiNo ratings yet
- Boala Crohn Clinical ManifestationsDocument16 pagesBoala Crohn Clinical ManifestationsEdith CroitoruNo ratings yet
- Ulcerative ColitisDocument88 pagesUlcerative ColitisYulia DjatiwardaniNo ratings yet
- Inflammatory Bowel DiseaseDocument27 pagesInflammatory Bowel DiseaseMihai VladescuNo ratings yet
- Ulcerative Colitis: PseudopolypsDocument26 pagesUlcerative Colitis: PseudopolypsSocorro S. Gantalao-CorbedaNo ratings yet
- Inflammatory Bowel DiseaseDocument37 pagesInflammatory Bowel DiseaseDrTushar GoswamiNo ratings yet
- Set 3 COMP-2Document71 pagesSet 3 COMP-2Appu ayyalaNo ratings yet
- Lecture 2-Part 1Document90 pagesLecture 2-Part 1mashe1No ratings yet
- Inflammatory Bowel Disease: Is Bloody DiarrheaDocument8 pagesInflammatory Bowel Disease: Is Bloody Diarrheaissam_1994No ratings yet
- Gastro NotesDocument18 pagesGastro NoteslukeNo ratings yet
- Dr. Ali's Uworld Notes For Step 2 CK: GastroDocument32 pagesDr. Ali's Uworld Notes For Step 2 CK: GastrouyesNo ratings yet
- Inflammatory Bowel DiseaseDocument59 pagesInflammatory Bowel DiseaseLala Rahma Qodriyan SofiakmiNo ratings yet
- Inflammatoray Bowel DiseaseDocument14 pagesInflammatoray Bowel DiseaseSadr AkrmNo ratings yet
- IBD Obat Ganguan Saluran CernaDocument13 pagesIBD Obat Ganguan Saluran CernaKhumairah mohtarNo ratings yet
- Ulcerative ColitisDocument14 pagesUlcerative ColitisAstari Puspaningdyah100% (1)
- Inflammatory Bowel Disease .. Last EditDocument22 pagesInflammatory Bowel Disease .. Last EditRashed ShatnawiNo ratings yet
- Appendicitis: Dr. Aplin I, SPBDocument12 pagesAppendicitis: Dr. Aplin I, SPBAyu Kusuma NingrumNo ratings yet
- The Presentation - Crohn's Disease - (3course)Document17 pagesThe Presentation - Crohn's Disease - (3course)Kashif KhandaNo ratings yet
- Inflammatory Bowel DiseaseDocument15 pagesInflammatory Bowel DiseaseYanushka Bruce HerathNo ratings yet
- NCM-Ulcerative Colitis ReportDocument22 pagesNCM-Ulcerative Colitis ReportJocelyn RiveraNo ratings yet
- Praduman SirDocument38 pagesPraduman Sirguptaharshvardhan9565No ratings yet
- Ulcerative ColitisDocument12 pagesUlcerative Colitisthap87No ratings yet
- Disease Rectum. - Inflammatory Disease Colon Intestine (Nonspecific Ulcerative Colitis, Crohn's Disease) - Colon Cancer IntestineDocument22 pagesDisease Rectum. - Inflammatory Disease Colon Intestine (Nonspecific Ulcerative Colitis, Crohn's Disease) - Colon Cancer IntestineTojan Faisal AlzoubiNo ratings yet
- Surgery: Crohn's DiseaseDocument9 pagesSurgery: Crohn's Diseaseapi-3829364No ratings yet
- Gastrointestinal Tuberculosis Imaging: Chest Radiograph Reveals Calcified Hilar Tuberculous LymphadenitisDocument14 pagesGastrointestinal Tuberculosis Imaging: Chest Radiograph Reveals Calcified Hilar Tuberculous Lymphadenitisafudaru6043No ratings yet
- Imaging in Inflammatory Bowel DiseaseDocument38 pagesImaging in Inflammatory Bowel DiseaseIqbalAmriFauzalNo ratings yet
- Ulcerative ColitisDocument9 pagesUlcerative ColitisMike GNo ratings yet
- 01 14 2021 GERD Inflammatory Bowel Disease Irritable Bowel Syndrome ALLENDocument66 pages01 14 2021 GERD Inflammatory Bowel Disease Irritable Bowel Syndrome ALLENMikey ZhitnitskyNo ratings yet
- Fight Back Against Inflammatory Bowel DiseaseDocument28 pagesFight Back Against Inflammatory Bowel DiseaseSabbra CadabraNo ratings yet
- UlcerativecolitisDocument27 pagesUlcerativecolitisMohamed Abdulrazaq100% (1)
- Inflammatory Bowel Disease FinalDocument60 pagesInflammatory Bowel Disease FinalRawabi rawabi1997No ratings yet
- Crohn DiseaseDocument14 pagesCrohn DiseaseMike GNo ratings yet
- 1 IbdDocument11 pages1 Ibdmarinamaher14No ratings yet
- Pathology of Small & Large Intestine: Developmental LesionsDocument5 pagesPathology of Small & Large Intestine: Developmental LesionsaiadalkhalidiNo ratings yet
- Ulcerative ColitisDocument21 pagesUlcerative ColitisShofiyyah SaniNo ratings yet
- Large Intestine L2Document51 pagesLarge Intestine L2Yousif AlaaNo ratings yet
- AppendicitisDocument36 pagesAppendicitisPetro MyronovNo ratings yet
- Inflammatory Bowel DiseaseDocument19 pagesInflammatory Bowel DiseaseDranreb Berylle MasangkayNo ratings yet
- Valentina Miacci VI Anno 2018/2019Document20 pagesValentina Miacci VI Anno 2018/2019valentina miacciNo ratings yet
- Pancreatitis Ercp Pain Amylase Lipase ErcpDocument24 pagesPancreatitis Ercp Pain Amylase Lipase ErcpPerplexed CeleryNo ratings yet
- Inflammatory Bowel Disease (Ibd)Document41 pagesInflammatory Bowel Disease (Ibd)api-19916399No ratings yet
- Afrisya Bimo Siwendro Marisha Yadian Putri Preceptor: DR - Liza Nursanty, Spb. FinacsDocument32 pagesAfrisya Bimo Siwendro Marisha Yadian Putri Preceptor: DR - Liza Nursanty, Spb. FinacsirmaNo ratings yet
- Ulcerative ColitisDocument17 pagesUlcerative ColitisCamille Joy Lucero Villegas100% (1)
- CH16 Patho D&R AgamDocument29 pagesCH16 Patho D&R AgamBio CheNo ratings yet
- Cholecystitis FinalDocument57 pagesCholecystitis FinalRajendra DesaiNo ratings yet
- Uc - MinDocument18 pagesUc - Minminhaj_2086No ratings yet
- 01 Gastritis & PUDxxDocument51 pages01 Gastritis & PUDxxTor Koang ThorNo ratings yet
- Fast Facts: Enfermedad inflamatoria intestinal Para Pacientes y las Personas que los Apoyan: Colitis ulcerativa y enfermedad de Crohn Información + Tomar el control = El mejor resultadoFrom EverandFast Facts: Enfermedad inflamatoria intestinal Para Pacientes y las Personas que los Apoyan: Colitis ulcerativa y enfermedad de Crohn Información + Tomar el control = El mejor resultadoNo ratings yet
- 3-Anorectal Abscess (3)Document24 pages3-Anorectal Abscess (3)Rasti AmediNo ratings yet
- StomasDocument16 pagesStomasRasti AmediNo ratings yet
- Report About: TitleDocument9 pagesReport About: TitleRasti AmediNo ratings yet
- Report About: TitleDocument3 pagesReport About: TitleRasti AmediNo ratings yet
- Report About: TitleDocument9 pagesReport About: TitleRasti AmediNo ratings yet
- Chapter 21 PancreasDocument102 pagesChapter 21 PancreasMACON824No ratings yet
- MIDTERMSDocument24 pagesMIDTERMSCherish Marie HurbodaNo ratings yet
- Jurnal Volvulus InternaDocument6 pagesJurnal Volvulus InternaSiti Hardianty SugehaNo ratings yet
- Barium Swallow (Esophagram) :: Positions and Barium Images PurposeDocument3 pagesBarium Swallow (Esophagram) :: Positions and Barium Images PurposeAaron SmithNo ratings yet
- Overview of Gallstone Disease in Adults - UpToDateDocument22 pagesOverview of Gallstone Disease in Adults - UpToDateJoseNo ratings yet
- Final Surgery Exam-4 Year Medical StudentsDocument15 pagesFinal Surgery Exam-4 Year Medical Studentsmotasem alsharifNo ratings yet
- Lab 1 Med. Virology & ParasitologyDocument4 pagesLab 1 Med. Virology & ParasitologyHussein AlaNo ratings yet
- Probiotics Can Cause D-Lactic Acidosis and Brain FDocument2 pagesProbiotics Can Cause D-Lactic Acidosis and Brain FRiccardo MartaNo ratings yet
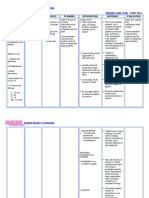
- Nursing Care Plan Peptic UlcerDocument3 pagesNursing Care Plan Peptic UlcerJefferson Baluyot PalmaNo ratings yet
- Drug Absorption Gastrointestinal TractDocument23 pagesDrug Absorption Gastrointestinal TractJose PerezNo ratings yet
- L10 - Liver CirrhosisDocument10 pagesL10 - Liver CirrhosisMerehan El RoosNo ratings yet
- Insolube Fibers Group-3 PDFDocument19 pagesInsolube Fibers Group-3 PDFHind almazrouei100No ratings yet
- Liver Function Tests (LFTS) : Laboratory InsightsDocument3 pagesLiver Function Tests (LFTS) : Laboratory InsightsmahithNo ratings yet
- Role of Flexible Transnasal Esophagoscopy and Patient Education in The Management of Globus Pharyngeus (CHENG 2012)Document5 pagesRole of Flexible Transnasal Esophagoscopy and Patient Education in The Management of Globus Pharyngeus (CHENG 2012)DANDYNo ratings yet
- Gastrointestinal Tract Bleeding: DR Stefanus Nangoi, M.Biomed, SPBDocument29 pagesGastrointestinal Tract Bleeding: DR Stefanus Nangoi, M.Biomed, SPBNindyNo ratings yet
- Micro Teaching On Colitis: School of Nursing Science and Research Sharda UniversityDocument21 pagesMicro Teaching On Colitis: School of Nursing Science and Research Sharda UniversityPooja SahuNo ratings yet
- GI BleedingDocument38 pagesGI BleedingNicklaus RiveraNo ratings yet
- Lax-Sachets: Read All of This Leaflet Carefully Before You Start Taking This MedicineDocument5 pagesLax-Sachets: Read All of This Leaflet Carefully Before You Start Taking This MedicineNeneNo ratings yet
- Abdominal ExaminationDocument20 pagesAbdominal ExaminationRacquel WilsonNo ratings yet
- Biological Drawing Lab 3 FHSC1224Document6 pagesBiological Drawing Lab 3 FHSC1224Ming LingNo ratings yet
- Disturbances in DigestionDocument2 pagesDisturbances in DigestionAnabelle RicoNo ratings yet
- NCP DiarrheaDocument2 pagesNCP DiarrheaPrincess Xzmae RamirezNo ratings yet
- ConstipationDocument1 pageConstipationVương TúNo ratings yet
- AUF SOM - Dse of Small Intestine PDFDocument166 pagesAUF SOM - Dse of Small Intestine PDFYestin Reece Corpus ArcegaNo ratings yet
- AnatomyvsPhysiology1 11Document12 pagesAnatomyvsPhysiology1 11Florilyn CabezoNo ratings yet
- Stool ElectrolyteDocument7 pagesStool ElectrolyteshoebNo ratings yet
- A MCQ: Si - No Sub Topics NameDocument2 pagesA MCQ: Si - No Sub Topics NameInzamamul Haque ShihabNo ratings yet
- 7-Neonatal Surgical EmergenciesDocument29 pages7-Neonatal Surgical EmergenciesResti Rangga SusiloNo ratings yet
- Bariatric and Metabolic Surgery: Luigi Angrisani EditorDocument209 pagesBariatric and Metabolic Surgery: Luigi Angrisani EditorBadri KobalavaNo ratings yet
- The Management of Anastomotic Leak: John Hartley Academic Surgical Unit University of HullDocument28 pagesThe Management of Anastomotic Leak: John Hartley Academic Surgical Unit University of Hullzieky yoansyahNo ratings yet