You might also like
- Fast Facts: Enfermedad inflamatoria intestinal Para Pacientes y las Personas que los Apoyan: Colitis ulcerativa y enfermedad de Crohn Información + Tomar el control = El mejor resultadoFrom EverandFast Facts: Enfermedad inflamatoria intestinal Para Pacientes y las Personas que los Apoyan: Colitis ulcerativa y enfermedad de Crohn Información + Tomar el control = El mejor resultadoNo ratings yet
- Crohn DiseaseDocument14 pagesCrohn DiseaseMike GNo ratings yet
- Inflammatory Bowel Disease (Ibd)Document28 pagesInflammatory Bowel Disease (Ibd)suhaNo ratings yet
- IBD - Shane Ryan ApperleyDocument63 pagesIBD - Shane Ryan Apperleyvivi avisaNo ratings yet
- Inflammatoray Bowel DiseaseDocument14 pagesInflammatoray Bowel DiseaseSadr AkrmNo ratings yet
- Ulcerative Colitis HandoutDocument1 pageUlcerative Colitis HandoutevedgebahNo ratings yet
- Ulcerative Colitis: PseudopolypsDocument26 pagesUlcerative Colitis: PseudopolypsSocorro S. Gantalao-CorbedaNo ratings yet
- UlcerativecolitisDocument27 pagesUlcerativecolitisMohamed Abdulrazaq100% (1)
- 01 14 2021 GERD Inflammatory Bowel Disease Irritable Bowel Syndrome ALLENDocument66 pages01 14 2021 GERD Inflammatory Bowel Disease Irritable Bowel Syndrome ALLENMikey ZhitnitskyNo ratings yet
- Inflammatory Bowel DiseaseDocument19 pagesInflammatory Bowel Diseasenathan asfahaNo ratings yet
- Ulcerative ColitisDocument12 pagesUlcerative Colitisthap87No ratings yet
- Ulcerative ColitisDocument17 pagesUlcerative ColitisCamille Joy Lucero Villegas100% (1)
- Ulcerative Colitis: DR Syed Ubaid Associate Professor of SurgeryDocument71 pagesUlcerative Colitis: DR Syed Ubaid Associate Professor of SurgeryFachry Al RafiqiNo ratings yet
- Ulcerativecolitis 170323180448 PDFDocument88 pagesUlcerativecolitis 170323180448 PDFBasudewo Agung100% (1)
- 28 - IbdDocument57 pages28 - IbdsitiNo ratings yet
- Crohns DiseaseDocument32 pagesCrohns DiseaseMin Chi PakNo ratings yet
- Gastro NotesDocument18 pagesGastro NoteslukeNo ratings yet
- Inflammatory Bowel Disease FinalDocument60 pagesInflammatory Bowel Disease FinalRawabi rawabi1997No ratings yet
- Ulcerative ColitisDocument88 pagesUlcerative ColitisYulia DjatiwardaniNo ratings yet
- Inflammatory Bowel DiseaseDocument59 pagesInflammatory Bowel DiseaseLala Rahma Qodriyan SofiakmiNo ratings yet
- Dr. Ali's Uworld Notes For Step 2 CK: GastroDocument32 pagesDr. Ali's Uworld Notes For Step 2 CK: GastrouyesNo ratings yet
- Q1 Describe The Clinical and Pathological Diagnostic Features That Distinguish InflammatoryDocument3 pagesQ1 Describe The Clinical and Pathological Diagnostic Features That Distinguish InflammatoryNicholasNo ratings yet
- IBD Final11Document41 pagesIBD Final11abraham debebeNo ratings yet
- Inflammatory Bowel DiseaseDocument15 pagesInflammatory Bowel DiseaseYanushka Bruce HerathNo ratings yet
- DefinitionDocument12 pagesDefinitionAylol 23No ratings yet
- IBD Obat Ganguan Saluran CernaDocument13 pagesIBD Obat Ganguan Saluran CernaKhumairah mohtarNo ratings yet
- Essay SuryaDocument5 pagesEssay SuryadewasayogaNo ratings yet
- Khalil PathoDocument43 pagesKhalil PathoMohammad zreadNo ratings yet
- Cholecystitis FinalDocument57 pagesCholecystitis FinalRajendra DesaiNo ratings yet
- Dr. S.P. Hewawasam (MD) Consultant Gastroenterologist/Senior Lecturer in PhysiologyDocument33 pagesDr. S.P. Hewawasam (MD) Consultant Gastroenterologist/Senior Lecturer in PhysiologyAjung SatriadiNo ratings yet
- Diverticular Disease: Qbank Session Clinical Sciences LearnedDocument11 pagesDiverticular Disease: Qbank Session Clinical Sciences LearnedMike GNo ratings yet
- Ulcerative ColitisDocument14 pagesUlcerative ColitisAstari Puspaningdyah100% (1)
- Set 3 COMP-2Document71 pagesSet 3 COMP-2Appu ayyalaNo ratings yet
- Day 10. Choledocholitiasis, CholangitisDocument26 pagesDay 10. Choledocholitiasis, Cholangitisهنادي رازمNo ratings yet
- Inflammatory Bowel Disease .. Last EditDocument22 pagesInflammatory Bowel Disease .. Last EditRashed ShatnawiNo ratings yet
- Acute CholangitisDocument9 pagesAcute CholangitisMike GNo ratings yet
- What Is An Acute AbdomenDocument112 pagesWhat Is An Acute AbdomenLavasa SharmaNo ratings yet
- en Hematochezia in Young Patient Due To CroDocument3 pagesen Hematochezia in Young Patient Due To Croseptian_tjayaNo ratings yet
- CSS Ulcerative ColitisDocument28 pagesCSS Ulcerative ColitisAthiyyah HasnaNo ratings yet
- Pancreatitis Ercp Pain Amylase Lipase ErcpDocument24 pagesPancreatitis Ercp Pain Amylase Lipase ErcpPerplexed CeleryNo ratings yet
- Acute Cholecystitits, Choledocholithiasis and Acute CholangitisDocument16 pagesAcute Cholecystitits, Choledocholithiasis and Acute CholangitisKath de L'EnferNo ratings yet
- Askep IbdDocument43 pagesAskep IbdYou100% (1)
- Crohn ' S Disease (Regional EnteritisDocument26 pagesCrohn ' S Disease (Regional EnteritisRasti AmediNo ratings yet
- Cholecystitis: Causes and PathologyDocument12 pagesCholecystitis: Causes and PathologySher KhanNo ratings yet
- La Simulación Como Herramientas para Adquirir CompetenciasDocument10 pagesLa Simulación Como Herramientas para Adquirir Competenciasjuan camilo marquez montielNo ratings yet
- English ThemeDocument4 pagesEnglish ThemeJu BuNo ratings yet
- A Girl With Ulcerative Colitis in A Tertiary Care Hospital-A Case ReportDocument4 pagesA Girl With Ulcerative Colitis in A Tertiary Care Hospital-A Case ReportWyn AgustinNo ratings yet
- A Girl With Ulcerative Colitis in A Tertiary Care Hospital-A Case ReportDocument4 pagesA Girl With Ulcerative Colitis in A Tertiary Care Hospital-A Case ReportAbdullah KhanNo ratings yet
- Ulcerative ColitisDocument30 pagesUlcerative ColitisAndika SulistianNo ratings yet
- Colitis, Ulcerative: Whitney D. Lynch Ronald HsuDocument8 pagesColitis, Ulcerative: Whitney D. Lynch Ronald HsuAlexis DF SanchezNo ratings yet
- Examen IM-gastroenterologieDocument15 pagesExamen IM-gastroenterologieNicola BereholschiNo ratings yet
- Ulcerative ColitisDocument4 pagesUlcerative ColitisMohammad Yordan GandaraNo ratings yet
- Patologia de La EII en NiñoDocument8 pagesPatologia de La EII en NiñoAdriana LopezNo ratings yet
- There Are Many Potential Causes of Liver AbscessesDocument4 pagesThere Are Many Potential Causes of Liver AbscessesmarianmadhurNo ratings yet
- Pain in The Right Upper QuadrantDocument15 pagesPain in The Right Upper QuadrantMaryam JamilahNo ratings yet
- Cholangitis: Reported By: R. DongaranDocument18 pagesCholangitis: Reported By: R. DongaranVishnu Karunakaran100% (1)
- Acute PancreatitisDocument11 pagesAcute Pancreatitispeter_soósNo ratings yet
- Infections of Gastrointestinal TractDocument35 pagesInfections of Gastrointestinal Tract180045No ratings yet
- Ibd AnushaDocument32 pagesIbd AnushaRupesh R100% (1)
- Immediate Management of Life Iate Management of Life-Threatening Problems Threatening ProblemsDocument3 pagesImmediate Management of Life Iate Management of Life-Threatening Problems Threatening ProblemsMike GNo ratings yet
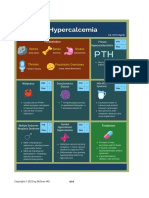
- HypercalcemiaDocument1 pageHypercalcemiaMike GNo ratings yet
- CBC DiffDocument8 pagesCBC DiffMike GNo ratings yet
- 2.15 Interpretasi Darah 3 Sudah Di Stabilo PDFDocument1 page2.15 Interpretasi Darah 3 Sudah Di Stabilo PDFalodiaNo ratings yet
- Neuro Dementia 2022Document5 pagesNeuro Dementia 2022Mike GNo ratings yet
- Chronic Mesenteric IschaemiaDocument2 pagesChronic Mesenteric IschaemiaMike GNo ratings yet
- Solid Visceral Injuries Solid Visceral Injuries Solid Visceral InjuriesDocument2 pagesSolid Visceral Injuries Solid Visceral Injuries Solid Visceral InjuriesMike GNo ratings yet
- Classification of ShockDocument3 pagesClassification of ShockYogi drNo ratings yet
- Differential Diagnosis of Neck Swellings PDFDocument3 pagesDifferential Diagnosis of Neck Swellings PDFSiddharth KatyalNo ratings yet
- Approach To Jundiced PatientDocument2 pagesApproach To Jundiced Patientmelinda SilalahiNo ratings yet
- Antaomy of GITDocument5 pagesAntaomy of GITMike GNo ratings yet
- Chapter 2 Surgical NutritionDocument3 pagesChapter 2 Surgical NutritionMike GNo ratings yet
- Gastrointestinal Bleeding PDFDocument1 pageGastrointestinal Bleeding PDFYogi drNo ratings yet
- Acute Coronary SyndromeDocument1 pageAcute Coronary SyndromeMike GNo ratings yet
- Chapter 35 NeurosurgeryDocument11 pagesChapter 35 NeurosurgeryMike GNo ratings yet
- Small Intenstine MedCosmos Surgery - MCQDocument29 pagesSmall Intenstine MedCosmos Surgery - MCQMike GNo ratings yet
- Stomach-Esophagus MedCosmos Surgery - MCQDocument39 pagesStomach-Esophagus MedCosmos Surgery - MCQMike G100% (1)
- Trauma and Burns MedCosmos Surgery - MCQDocument32 pagesTrauma and Burns MedCosmos Surgery - MCQMike GNo ratings yet
- Vascular Surgery MedCosmos Surgery - MCQDocument34 pagesVascular Surgery MedCosmos Surgery - MCQMike GNo ratings yet
- Spleen MedCosmos Surgery - MCQDocument11 pagesSpleen MedCosmos Surgery - MCQMike GNo ratings yet
- Chapter 36 Intracranial and Spinal TraumaDocument5 pagesChapter 36 Intracranial and Spinal TraumaMike GNo ratings yet
- Chapter 39 Obstetrics and GynecologyDocument3 pagesChapter 39 Obstetrics and GynecologyMike GNo ratings yet
- Chapter 33 Plastic and Reconstructive SurgeryDocument4 pagesChapter 33 Plastic and Reconstructive SurgeryMike GNo ratings yet
- Thyroid Gland MedCosmos Surgery - MCQDocument17 pagesThyroid Gland MedCosmos Surgery - MCQMike GNo ratings yet
- Chapter 34 Pediatric SurgeryDocument11 pagesChapter 34 Pediatric SurgeryMike G100% (1)
- Chapter 60: Headache: Section 10: NeurologyDocument16 pagesChapter 60: Headache: Section 10: NeurologyAnonymous Xmb6QQvRNo ratings yet
- Chapter 1 Cell Physiology and StructureDocument4 pagesChapter 1 Cell Physiology and StructureMike GNo ratings yet
- Section 11 - Selected Topics in General and Internal MedicineDocument65 pagesSection 11 - Selected Topics in General and Internal MedicineMike GNo ratings yet
- Hopkins Medicine Review Oncology Section PDFDocument39 pagesHopkins Medicine Review Oncology Section PDFaliaaNo ratings yet
- Hopkins Medicine Review HematologyDocument35 pagesHopkins Medicine Review HematologyGuna Babu100% (1)
- MRCS Recall All Jan Exams 2016 - 2021Document164 pagesMRCS Recall All Jan Exams 2016 - 2021muawazmuhammad2100% (4)
- Diarrhoea: More Than Just A Splash in The PanDocument16 pagesDiarrhoea: More Than Just A Splash in The PanIgor DemićNo ratings yet
- Granulomatous Colitis: More Than A Canine Disease? A Case of Escherichia Coli-Associated Granulomatous Colitis in An Adult CatDocument5 pagesGranulomatous Colitis: More Than A Canine Disease? A Case of Escherichia Coli-Associated Granulomatous Colitis in An Adult Catclara FNo ratings yet
- Metab II DiverticulosisDocument94 pagesMetab II DiverticulosisEthel Lourdes Cornejo AmodiaNo ratings yet
- Post-Test GIT: Prepared By: Prof. EJ FlaminianoDocument5 pagesPost-Test GIT: Prepared By: Prof. EJ FlaminianoKristele Joy Bagarino - Raralio0% (1)
- Ulcerative ColitisDocument5 pagesUlcerative ColitisAngelica RelanaNo ratings yet
- NP 3 Test BanksDocument12 pagesNP 3 Test BanksHeart Maechille CampomayorNo ratings yet
- Inflammatory Bowel Disease: DefinitionDocument4 pagesInflammatory Bowel Disease: Definitionkarl abiaadNo ratings yet
- Ulcerative ColitisDocument13 pagesUlcerative ColitisAlis GomezNo ratings yet
- Approach To Patient With Gastrointestinal SystemDocument23 pagesApproach To Patient With Gastrointestinal SystemMarshell TendeanNo ratings yet
- All Therapy 200 RATOS 2010Document284 pagesAll Therapy 200 RATOS 2010Bhargavi SunkiNo ratings yet
- Clinical Feature and Diagnosis of IbdDocument56 pagesClinical Feature and Diagnosis of IbdVicks Vikash KumarNo ratings yet
- Ulcerative Colitis and Crohn's DiseaseDocument72 pagesUlcerative Colitis and Crohn's DiseasedalibormilenkovicNo ratings yet
- Colitis PDFDocument11 pagesColitis PDFicoanamareNo ratings yet
- Takes For Treatment Impetigo Hemolytic The Following Is The Thi in ThiDocument46 pagesTakes For Treatment Impetigo Hemolytic The Following Is The Thi in Thisam3557No ratings yet
- Zuhir PBL-I (Inflammatory Bowel Disease)Document43 pagesZuhir PBL-I (Inflammatory Bowel Disease)darkwarrior_mfh22No ratings yet
- 22 - 7 - 22 Clinical Trials On Gamma OryzanolDocument113 pages22 - 7 - 22 Clinical Trials On Gamma OryzanolShivamNo ratings yet
- Gastrointestinal Pathology Case Studies ParDocument2 pagesGastrointestinal Pathology Case Studies Pardr nirupamaNo ratings yet
- Case Study 11Document28 pagesCase Study 11api-301883277No ratings yet
- Eosinophilic Colitis and Colonic EosinophiliaDocument9 pagesEosinophilic Colitis and Colonic EosinophiliadkbritobNo ratings yet
- Diet PlanDocument1 pageDiet PlanmpvmenonNo ratings yet
- Ibd AnushaDocument32 pagesIbd AnushaRupesh R100% (1)
- Chronic DiarrheaDocument66 pagesChronic DiarrheaJulita Yanti100% (1)
- English 8 Q2 FDocument40 pagesEnglish 8 Q2 FHoneylet bernardinoNo ratings yet
- Full Download Medical Surgical Nursing Critical Thinking For Collaborative Care PDF Full ChapterDocument36 pagesFull Download Medical Surgical Nursing Critical Thinking For Collaborative Care PDF Full Chapterjasonjohnsonfzcjibytag100% (16)
- Typhlitis: Clinical Presentation and DiagnosisDocument2 pagesTyphlitis: Clinical Presentation and DiagnosisMUWANGUZI ALEXANDERNo ratings yet
- Which of The Following Complications Is Thought To Be The Most Common Cause of AppendicitisDocument15 pagesWhich of The Following Complications Is Thought To Be The Most Common Cause of AppendicitisKristine CastilloNo ratings yet
- Application Details: About YouDocument11 pagesApplication Details: About YouMarius LixandruNo ratings yet
- Ulcerative ColitisDocument15 pagesUlcerative Colitisapi-252717471100% (1)
- Practice Guidelines For The Management of Infectious DiarrheaDocument21 pagesPractice Guidelines For The Management of Infectious DiarrheaJose Alfredo Cruz HernandezNo ratings yet